
Abstract
This is the second in a two-part series that aims to summarise answers to common questions facing dentists in general practice. The first part of this series is entitled 'Periodontal care in general practice: 20 important FAQs − Part one' (Br Dent J 2019;226: 850-854) and contains the first set of ten FAQs.
Similar content being viewed by others



Key points
-
Covers the management of patients with drug-influenced gingival enlargement and those with occlusal trauma.
-
Discusses indications for splinting, the use of antibiotics in periodontitis, and factors to consider when placing dental implants in periodontal patients.
-
Advises on risk assessment, supportive periodontal therapy, specialist referral guidelines and minimising risks of litigation.
1: How do I manage patients with drug-influenced gingival enlargement?
Drug-influenced gingival enlargement is now classified as a form of plaque-induced gingivitis according to the 2017 World Workshop Classification of periodontal diseases and conditions, recognising that certain drugs may modify the inflammatory-immune response to plaque accumulation and that improved plaque control reduces the enlargement.1 Gingival enlargement, or 'overgrowth' as it has been referred to, is an overarching clinical description that does not necessitate a diagnosis based upon the histologic composition of the affected gingival tissues. Moreover, it comprises a mixture of processes that include hyperplasia, hypertrophy of several cell types, increased extracellular matrix production and an inflammatory component, hence justifying a non-specific term like 'enlargement'. Drug-influenced gingival enlargement can be associated with calcium channel blockers (for example, amlodipine), immunosupressants (for example, ciclosporin) or anticonvulsants (for example, phenytoin). The first signs of change are reported to arise about 1-3 months following the start of dosing and there would appear to be minimal threshold plasma levels of the drugs below which drug-related gingival overgrowth is unlikely to occur.2,3,4 However, the evidence base is rather lacking and prevalence data varies significantly (for review see Heasman & Hughes 2014).5
The clinical appearance varies according to the causative drug, phenytoin giving rise to a largely fibrotic and pink enlargement, whereas calcium channel blockers are associated with a more vascular overgrowth. The interdental papillae become swollen with a granular, pebbly surface which may enlarge further to become nodular and lobulated as the tissues coalesce to affect the marginal and attached gingiva.5 Enlarged tissues usually have two components: a fibrosis component involving excess collagen deposition, and an inflammatory one that is initiated by bacterial plaque accumulation. While the two components present in the enlarged gingivae are likely to be a result of distinct pathogenic processes, they are almost always observed in combination. The role of bacterial plaque in the overall pathogenesis of drug-influenced gingival enlargement is now regarded as important, with the majority of studies indicating that plaque is a prerequisite for the gingival overgrowth to occur.
Steps for management in practice:
-
1.
Ensure you have an up-to-date medical history for all your patients, including a drug history
-
2.
Contact the patient's general medical practitioner to find out if it would be feasible to replace the drug with an alternative. This might be carried out following initial therapy or at the start if the overgrowth is severe. It is important to emphasise that this decision rests with the prescribing medical practitioner and the dentist's role is only to advise. The decision to replace the drug will depend on the assessment of the potential benefits against the medical risks. However, it is also inappropriate to manage medical conditions/drug side effects surgically and therefore when alternative drugs exist, which is the case for ciclosporin (tacrolimus) and calcium channel blocking drugs (diuretics, beta-blockers, ACE-inhibitors etc), then the case for drug substitution is strong. In the case of epilepsy, this may be more challenging in patients who have been stable taking phenytoin for many years, as suffering a fit if it is substituted may impact upon their ability to drive. Drug substitution has been reported to result in spontaneous resolution of drug-influenced gingival enlargement6
-
3.
Oral hygiene reinforcement - effective home care is important in those who have developed drug-influenced gingival enlargement, but also for those who are at risk of developing it. Highlight the importance of this to patients and show the patient how they can achieve this. Modification of brushing technique with particular attention to angulation into the gingival sulcus area and use of interproximal cleaning aids would be important. Single-tufted brushes might be helpful around large areas of overgrowth where the use of interdental brushes is not physically possible
-
4.
Complete a BPE and six-point pocket chart if indicated. Radiographic examination is essential to determine the extent and severity of any bone loss, given that probing measures are likely to be confounded by the enlargement and thus inaccurate as measures of gingival attachment
-
5.
Carry out supragingival debridement and root surface debridement as necessary. Ensure any plaque retentive factors, such as overhanging restorations, have been corrected
-
6.
Where cause-related therapy has failed to bring adequate resolution of gingival overgrowth and interference with speech, function or aesthetics persists, surgery may be indicated. Even if complete resolution is unlikely without surgery, the non-surgical approach should be attempted in the first instance to reduce inflammation and risk of recurrence post-operatively. Referral to a specialist may be required. Surgery for these cases is of a resective nature, which aims to make the gingival tissues more amenable to plaque control (Fig. 1). However, patients should be aware that long-term recurrence will occur in around 40% of cases if there is no change in the drug treatment7
Fig. 1 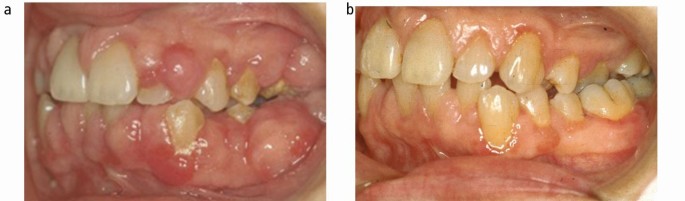
(a) Phenytoin-related gingival enlargement; (b) Following non-surgical and surgical periodontal therapy.
-
7.
Regular periodontal supportive therapy/maintenance would be important to minimise the risk of recurrence.

2: What is occlusal trauma, and does it impact on periodontitis?
Traumatic occlusal force is defined as any occlusal force resulting in injury of the teeth and/or the periodontal attachment apparatus.8 Occlusal trauma is a term used to describe the injury to the periodontal attachment apparatus A clinical diagnosis of occlusal trauma may be made in the presence of one or more of the following: progressive tooth mobility, adaptive tooth mobility (fremitus), radiographically widened periodontal ligament space, tooth migration, discomfort/pain on chewing, and root resorption.
Primary occlusal trauma has been defined as injury resulting in tissue changes from traumatic occlusal forces applied to a tooth or teeth with normal periodontal support. This manifests itself clinically with adaptive mobility and is not progressive. Secondary occlusal trauma has been defined as injury resulting in tissue changes from normal or traumatic occlusal forces applied to a tooth or teeth with reduced support,8 ie in patients with periodontitis. Teeth with progressive mobility may also exhibit migration and pain on function.
Occlusal trauma is a co-factor that can increase the rate of progression of periodontitis. When treating patients with secondary occlusal trauma, the treatment of the periodontitis itself should remain the primary focus. In addition to this, if the patient has parafunctional habits, provision of an occlusal splint should be considered. If occlusal adjustments are indicated to help correct occlusal disharmonies, these must be carried out carefully in order to preserve centric stops.
3: When might permanent splinting in periodontitis patients be considered?
The key indications for permanent splinting are:
To immobilise mobile teeth that are causing discomfort or affecting function
To immobilise teeth where there is progressive increase in mobility; and
To prevent further movement of teeth, including drifting, overeruption, or relapse of orthodontically treated teeth.9
Prior to splinting, it is imperative that the periodontitis has been addressed as a splint will make plaque control around teeth more difficult. A range of different materials have been described for splinting. One of the most common is using composite resin. However, composite resin alone is weak and brittle, so will fracture easily. Fibreglass-reinforced composite or archwire and composite would be more appropriate options (Fig. 2). The latter is preferable whenever possible as it allows some independent tooth movement, thus stimulating the periodontal ligament and alveolar bone, preventing atrophy. The use of fibre-reinforced composite resin produces a more rigid splint that can result in alveolar bone atrophy and ultimately the need to extract the tooth.

(a) Severe periodontitis case with archwire and composite splint; (b) Pre-operative radiographs
4: When should I consider using antibiotics when treating periodontitis patients?
With antimicrobial resistance on the increase, the prescription of antibiotics for the treatment of periodontitis should be carefully considered and if possible avoided. Antibiotics should only be prescribed when the amount of disease is clearly not consistent with existing aetiological factors or if the response to standard non-surgical treatment has been unusual - this will often be in the previously called 'aggressive periodontitis' patients. The term 'Grade C' periodontitis is now used in the 2017 classification system, and where the rate of destruction of periodontal attachment is not consistent with local factors (for example, the patient has good oral hygiene and does not have sub-gingival calculus) in Grade C disease, antibiotics may be required. In general practice, this will only be for a very limited number of patients as patients with Grade C disease are likely to be referred for specialist care. Other less common examples include those with necrotising periodontitis.
If antibiotics are considered, these should be systemic as the evidence-base for local antibiotics employed at multiple sites is limited. Studies for local antibiotics show that probing depth reductions following repeat root surface debridement alone are equal to or better than that achieved with local antimicrobials.10,11,12 Systemic antimicrobials should be used as an adjunct to root surface debridement and not as a monotherapy as there is a need to disturb the biofilm first. The antibiotics should be taken following the final session of root surface debridement and all debridement completed in 7-14 days.13,14 There is no optimal protocol for antimicrobial type or regime, however empirical evidence and practicality are usually taken into account. For example, in a penicillin-allergic patient 100 mg doxycycline might be beneficial. Those with a significant amount of infection may benefit from a combination of metronidazole and amoxicillin. Azithromycin is popular as compliance is easy with only one tablet per day for 3 days. Table 1 provides a summary of common antibiotic regimes used in the treatment of periodontitis.
5: What are the key factors to be aware of when considering dental implants for periodontitis patients?
A. Risk of peri-implant disease
Patients with existing periodontitis have a greater risk of developing peri-implantitis.15 Moreover, patients with a history of periodontitis, over a long term exhibit: greater probing depths and bone loss around implants, a higher incidence of peri-implantitis16 and higher overall failure rates.17 Implants placed in periodontally susceptible patients have been shown to experience significantly higher amounts of bone loss compared to periodontally healthy patients irrespective of the implant type chosen.18 For this reason, it is imperative to treat the periodontitis first and aim to eliminate any deep periodontal probing depths before implant placement. Individuals with a history of periodontitis should be warned from the outset and as part of the informed consent process that they are at a higher risk of complications.
B. Implant position
Implants should not be positioned too close together as this may impair access for adequate plaque control. It is advisable to aim to maintain 3 mm spacing between implants where this is possible. Prior to implant placement, historical loss of hard and soft tissues may result in the inability to place an implant in the correct three-dimensional position. Incorrect bucco-lingual implant placement can lead to restorations with uncleansable overhangs. Deep placement may create deep probing depths and an extensive subgingival environment impairing optimal plaque control. It is important to be aware of these complications during the planning stage and consider bone and/or soft tissue grafting if indicated.
C. Screw vs cement
Screw-retained restorations are preferable where possible. Caution is required if using cemented restorations due to the risk of the extrusion of excess cement into the peri-implant sulcus when seating the restoration. The amount of excess cement is generally greater with deeper crown margins.19 Cement remnants may provide a rough surface for microorganisms to colonise leading to peri-implant mucositis and possibly peri-implantitis. Cement may also act as a foreign body and provoke an inflammatory response that might result in peri-implantitis.
D. Removable options
It may not always be necessary to provide a fixed restoration. Overdentures are often a more cleansable and safer long-term solution for some patients. A removable prosthesis replaces both hard and soft tissue, which might provide a better aesthetic outcome as well as allowing better access to the peri-implant tissues for plaque control.
E. Supportive therapy
Longitudinal studies have shown that a lack of supportive therapy is associated with a higher frequency of peri-implantitis.20 For this reason, supportive periodontal therapy is integral in minimising risks. Recall intervals should be tailored according to previous periodontal therapy, location of the soft tissues, implant location and prosthesis design.
F. Extracting teeth to replace with implants
There is now a growing body of evidence to suggest that maintaining periodontally involved teeth can provide better survival outcomes and can also be more cost-effective than placing implant-retained crowns.21,22 Thus there is a gradual move towards retaining periodontally involved teeth for as long as possible, before replacement with implants, as a general principle.
6: Why is it important to formally risk assess my patients with periodontal disease?
Risk assessment uses the current evidence base to identify patients who have a higher likelihood of developing a specific disease and provides them with enhanced preventive care pathways.23
Periodontitis is a complex condition in that it involves a series of interactions between the host's inflammatory-immune responses, which are influenced by genetic, environmental and lifestyle factors and the plaque biofilm. The risk factors for periodontitis carry different weights and interactions. For this reason, periodontal risk assessment is not a simple process. A recent consensus meeting by the European Federation of Periodontology, which analysed the latest systematic reviews in this area, supported two systems: PreViser (also provided through DEPPA, the Denplan PreViser Patient Assessment in the UK)24 and the Periodontal Risk Assessment (PRA) tool.25 The validity and predictive ability of these systems has been demonstrated in a number of studies.26,27
PreViser/DEPPA technology is commonly used in general dental practice (Fig. 3). It involves an online assessment that evaluates 11 factors: patient age, smoking, diabetes, history of periodontal surgery, pocket depth, bleeding on probing, furcation involvements, subgingival restorations, root calculus, radiographic bone height and the presence of vertical bone lesions. A patient report is then designed as a biofeedback and communication tool. This includes numeric and traffic light coded representations of periodontal disease risk (scale of 1-5) and severity (scale of 1-100). A graph is also produced which tracks changes in comparison to the previous assessment. Suggested treatment options are provided depending on the initial inputs. A randomised controlled trial (RCT) showed that this system improves psychological outcomes for the patient.28,29 The use of the system as a biofeedback tool has also been shown in a RCT performed in the primary care sector to improve plaque scores, bleeding and self-reported interdental cleaning. This is the first time a risk assessment tool has been demonstrated to improve oral health.30

DEPPA print out for periodontal risk
The PRA is an online tool that has been widely used in specialist teaching programmes (Fig. 4). It is often referred to as the spider diagram. It produces a functional graphical representation of a patient's risk based on six clinical, systemic and environmental factors, including: percentage bleeding on probing, number of residual periodontal pockets ≥5 mm, number of lost teeth, alveolar bone loss in relation to patient age, systemic and/or genetic predispositions and environmental factors such as tobacco use. This tool is designed to be used after periodontal therapy has been completed.

PRA spider diagram
The key aim of risk assessment is to identify patients who are at risk before irreversible damage occurs. The clinician is able to determine the high-risk patient's care plan in terms of recall periods, reduction of risk factors, intensity of treatment and referral to specialists more effectively. In the same way, risk-based prevention also helps to prevent over-treatment. In addition, quantifying risk and disease by means of scores allows the success of care plans to be objectively measured. This would be valuable on an individual, practice and population level. Perhaps most importantly, personalised risk communication to patients appears effective in stimulating behaviour change and has important medico-legal implications regarding the engagement of patients in their own health behaviours.
7: Can periodontitis be stabilised for life so my patients can retain their teeth?
There is now overwhelming evidence that well performed periodontal therapy in an engaged patient works well. Successful treatment can mean patients retain their teeth for life. Even with an improved periodontal outcome that is not absolutely optimal, the lifespan of the teeth will be improved. The key to maintaining improvements and preventing tooth loss is optimal oral hygiene and regular supportive periodontal therapy.31,32 Figure 5 illustrates a case where only non-surgical periodontal therapy was carried out. Most might consider extracting this tooth but through effective non-surgical periodontal therapy the probing depths have reduced significantly and there is also evidence of bony infill when examining the radiographs.

Non-surgical periodontal therapy (a) Before; (b) Six months after
8: What is the importance of supportive periodontal therapy?
Supportive periodontal therapy or maintenance is an effective and integral component of managing periodontitis patients. Its importance should be emphasised to patients before commencing any active treatment. With supportive periodontal therapy, periodontal health can be maintained in the majority of patients, even in advanced cases.33,34 Rosling and colleagues (2001) demonstrated that over a 12-year period of risk-directed periodontal maintenance, tooth loss could be minimised and the periodontal condition of high-risk individuals could be maintained in a largely stable situation; in low risk individuals, the periodontitis was virtually eliminated.35
The aims of supportive periodontal therapy would be to:
Monitor whether the condition is stable and provide an opportunity to initiate treatment if progression is detected
Remove aetiological factors before the disease progresses
Reinforce smoking cessation and organise referral if appropriate.
Recall intervals should be based on the patient's risk profile but the default is usually 3 months. However, evidence-based algorithms are being developed to direct recall intervals in a more personalised approach.36
9: What are the guidelines for referring patients for specialist care?
It is important to minimise any delay in referral for specialist care if indicated. It is much easier for patients to allege, after the 'event' (usually tooth loss), that they would have preferred a referral for specialist care. Failure to refer at an appropriate time is a common reason for litigation when considering periodontal cases.
The British Society of Periodontology's guidelines on specialist referral37 suggest complexity 3 cases should mostly be referred. This includes a BPE score of 4 in any sextant as well as one or more of the following additional factors:
A medical factor that is affecting the periodontal tissues, such as diabetes
Complicating root morphologies and anatomical factors adversely affecting prognosis
Previous classification as 'aggressive periodontitis'
No response to previous optimally carried out treatment
Patient's requiring surgical procedures
Medical history significantly affecting clinical management (history of head/neck radiotherapy or intravenous bisphosphonate therapy)
Immunocompromised/immunosuppressed, significant bleeding disorder, potential drug interactions
Regular tobacco smoking (10+ cigarettes/day)
Concurrent mucogingival disease such as erosive lichen planus.
If referring to a hospital rather than private practice, it is also important to be aware of the hospital's guidelines and acceptance criteria.
10. How can I minimise my chances of litigation through record keeping?
Specific phrases in your record-keeping templates can help minimise chances of missing important discussion points with patients. It is important that the templates used are true, appropriate and tailored to each individual patient. Here are a few examples of phrases that may be helpful:
'Patient advised of mild/moderate/severe periodontal disease'
'Patient warned of tooth mobility and tooth loss related to periodontal disease'
'Patient advised that they are at risk of developing periodontitis'
'Patient informed on the risks of smoking in relation to periodontal disease - discussed increased risk for the condition and likely poorer response to therapy'
'Patient advised that oral hygiene is not adequate to support formal periodontal therapy. Guided to improve plaque levels to support periodontal therapy'
'Patient shown how to use interdental brushes and advised on the following sizes:...'
'Discussed referral to periodontal specialist.'
Change history
24 January 2020
Author's correction note: When this article was initially published, the following boxes in Table 1 were incorrect: In the top row of the Dosage column, 'Doxycyline 200 mg (loading dose), 100 mg OD for 14 days' should have read 'Doxycyline 200 mg (loading dose), 100 mg OD for 21 days' In the top r...
References
Murakami S, Mealey B L, Mariotti A, Chapple I L C. Dental plaque-induced gingival conditions. J Clin Periodontol 2018; 45 (Suppl 20): S17-S27.
Tipton D A, Stricklin G P, Dabbous M K. Fibroblast heterogeneity of collagenolytic response to cyclosporine. J Cell Biochem 1991; 46: 152-165.
Hallmon W W, Rossman J A. The role of drugs in the pathogenesis of gingival overgrowth. A collective review of current concepts. Periodontol 2000 1999; 21: 176-196.
Nishikawa S, Taha H, Hamasaki A et al. Nifedipine-induced gingival hyperplasia: a clinical and in vitro study. J Periodontol 1991; 62: 30-35.
Heasman P A, Hughes F J. Drugs, medications and periodontal disease. Br Dent J 2014; 217: 411-419.
Butterworth C J, Chapple I L C. Drug-induced gingival overgrowth: a case of auto-correction of incisor drifting. Dent Update 2001; 28: 411-416.
Ilgenli T, Atilla G, Baylas H. Effectiveness of peri-odontal therapy in patients with drug-induced gingival overgrowth. Long-term results. J Periodontol 1999; 70: 967-972.
Jepsen S, Caton J G, Albandar J M et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol 2018; 45(S20): S219-S229.
Hughes F J. Clinical problem solving in periodontology and implantology. 1st ed. Churchill Livingstone Elsevier, 2013.
Magnusson I, Lindhe J, Yoneyama T, Liljenberg B. Recolonization of a subgingival microbiota following scaling in deep pockets. J Clin Periodontol 1984; 11: 193-207.
Timmerman M F, van der Weijden G A, van Steenbergen T J, Mantel M S, de Graaff J, van der Velden U. Evaluation of the long-term efficacy and safety of locally-applied minocycline in adult periodontitis patients. J Clin Periodontol 1996; 23: 707-716.
Garrett S, Adams DF, Bogle G et al. The effect of locally delivered controlled-release doxycycline or scaling and root planing on periodontal maintenance patients over 9 months. J Periodontol 2000; 71: 22-30.
Herrera D, Sanz M, Jepsen S, Needleman I, Roldán S. A systematic review on the effect of systemic antimicrobials as an adjunct to scaling and root planing in periodontitis patients. J Clin Periodontol 2002; 29(S3): 136-159.
Haffajee A D, Socransky S S, Gunsolley J C. Systemic anti-infective periodontal therapy. A systematic review. Ann Periodontol 2003; 8: 115-181.
Pjetursson B E, Helbling C, Weber H P et al. Peri-implantitis susceptibility as it relates to periodontal therapy and supportive care. Clin Oral Implants Res 2012; 23: 888-894.
Sgolastra F, Petrucci A, Severino M, Gatto R, Monaco A. Periodontitis, implant loss and peri-implantitis. A meta-analysis. Clin Oral Implants Res 2015; 26: e8-e16.
Koldsland O C, Scheie A A, Aass A M. Prevalence of implant loss and the influence of associated factors. J Periodontol 2009; 80: 1069-1075.
Matarasso S, Rasperini G, Iorio Siciliano V, Salvi G E, Lang NP, Aglietta M. A 10-year retrospective analysis of radiographic bone-level changes of implants supporting single-unit crowns in periodontally compromised vs. periodontally healthy patients. Clin Oral Implants Res 2010; 21: 898-903.
Linkevicius T, Vindasiute E, Puisys A, Linkeviciene L, Maslova N, Puriene A. The influence of the cementation margin position on the amount of undetected cement. A prospective clinical study. Clin Oral Implants Res 2013; 24: 71-76.
Roccuzzo M, Bonino L, Dalmasso P, Aglietta M. Long-term results of a three arms prospective cohort study on implants in periodontally compromised patients: 10-year data around sandblasted and acid-etched (SLA) surface. Clin Oral Implants Res 2014; 25: 1105-1112.
Levin L, Halperin-Sternfeld M. Tooth preservation or implant placement: a systematic review of long-term tooth and implant survival rates. J Am Dent Assoc 2013; 144: 1119-1133.
Schwendicke F, Stolpe M, Müller F. Professional oral health care for preventing nursing home-acquired pneumonia: A cost-effectiveness and value of information analysis. J Clin Periodontol 2017; 44: 1236-1244.
Chapple L, Chapple I. Risk assessment in periodontal disease. Dent Update 2018; 45: 920-926.
Genco R J, Borgnakke W. Risk factors for periodontal disease. Periodontol 2000 2013; 62: 59-94.
Lang N P, Tonetti M S. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev Dent 2003; 1: 7-16.
Page R C, Martin J, Krall E A, Mancl L, Garcia R. Longitudinal validation of a risk calculator for periodontal disease. J Clin Periodontol 2003; 30: 819-827.
Matuliene G, Studer R, Lang N P et al. Significance of periodontal risk assessment in the recurrence of periodontitis and tooth loss. J Clin Periodontol 2010; 37: 191-199.
Asimakopoulou K, Newton J T, Daly B, Kutzer Y, Ide M. The effects of providing periodontal disease risk information on psychological outcomes - a randomized controlled trial. J Clin Periodontol 2015; 42: 350-355.
Sharma P, Busby M, Chapple L, Matthews R, Chapple I. The relationship between general health and lifestyle factors and oral health outcomes. Br Dent J 2016; 221: 65-69.
Asimakopoulou K, Nolan M, McCarthy C, Newton J T. The effect of risk communication on periodontal treatment outcomes: A randomised controlled trial. J Periodontol 2019; 90: 948-956.
Axelsson P, Lindhe J. The significance of maintenance care in the treatment of periodontal disease. J Clin Periodontol 1981; 8: 281-294.
Ramfjord S P, Morrison E C, Burgett F G et al. Oral hygiene and maintenance of periodontal support. J Periodontol 1982; 53: 26-30.
Axelsson P, Nyström B, Lindhe J. The long-term effect of a plaque control programme on tooth mortality, caries and periodontal disease in adults. Results after 30 years of maintenance. J Clin Periodontol 2004; 31: 749-757.
Nyman S, Lindhe J. A longitudinal study of combined periodontal and prosthetic treatment of patients with advanced periodontal disease. J Periodontol 1979; 50: 163-169.
Rosling B, Serino G, Hellström M K, Socransky S S, Lindhe J. Longitudinal periodontal tissue alterations during supportive therapy. J Clin Periodontol 2001; 28: 241-249.
Ramseier C A, Nydegger M, Walter C et al. Time between recall visits and residual probing depths predict long-term stability in patients enrolled in supportive periodontal therapy. J Clin Periodontol 2019; 46: 218-230.
British Society of Periodontology. Referral policy and parameters of care. Available online at https://www.bsperio.org.uk/publications/downloads/28_143801_parameters_of_care.pdf (accessed 4 April 2019).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Prof Chapple acts as an adviser to Oral Health Innovations, who license PreViser software in the UK and Ireland
Rights and permissions
About this article

Cite this article
Wadia, R., Chapple, I. Periodontal care in general practice: 20 important FAQs - Part two. Br Dent J 227, 875–880 (2019). https://doi.org/10.1038/s41415-019-0944-9
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-019-0944-9
