
Abstract
Background Since its discovery in 1862, the Gaillardot Phoenician gold wire dental bridge (Louvre artefact no. 5,777) has been the subject of conflicting interpretations as to its correct situation in the jaws, the origin of replaced teeth, and the possibility of teeth having been rearranged within the appliance.
Methods This paper offers an analysis based on examination and digital macrophotography of the appliance at the Louvre. Resultant images aided never-before considered points of evidence such as aspects of individual tooth anatomy, occlusion, and the need of the fabricating artisan to allow for crowding of the original dentition.
Results Pontic and abutment teeth bear a labial horizontal developmental groove and are the same colour. Canines and incisors conform to mandibular teeth anatomy and canines are in their correct positions. Canine incisal cusp wear and a flat labial arch indicates the dentition had been an Angle Class III anterior relationship. The incisor pontic teeth had originally been crowded out of the arch and were trimmed to reduce their width to fit the bridge within the arch.
Conclusions This extra evidence confirms the interpretation of a mandibular setting and correct positioning of teeth within the appliance. To create a favourable dental arrangement to address bridge stability and longevity, the fabricating artisan had to modify the dentition.
Similar content being viewed by others


Key points
-
Suggests a possible reinterpretation of the Gaillardot Phoenician appliance.
-
Highllights canine tooth anatomy.
-
Discusses mandibular masticatory movement.
Introduction
The Gaillardot dental appliance, found at Sidon, Phoenicia (Fig. 1) in 1862, was made to replace two anterior teeth presumably lost to periodontal disease. Renan's 1864 description claimed it was attached to a remnant of female maxilla.1 However, as the artefact is now presented, any such bone has been lost (not depicted in Renan's drawing in Figure 2) and at some time it appears to have been made rigid by application of a glue (visible in Figures 3 and 4). The dental appliance is a six-unit fixed anterior bridge with two pontics (Fig. 3).

Phoenicia. A geographical name of Greek origin corresponding to modern coastal Lebanon and northern Israel. The historical Phoenicians were traders who flourished c.1500-332 BCE). Reproduced with permission from Bible History

a) Renan drawing, 1864; b) Guerini drawing, 1909. Note both depict a maxillary setting and the claimed bone fragment is missing as early as Renan's drawing. Renan's drawing conforms somewhat to the existing state of the artefact with eroded root ends and worn incisal edges and canine cusps whereas Guerini's rendition is idealised

Gaillardot appliance: a) labial view; b) lingual view; c) incisal view. Note characteristic features of mandibular incisors: lateral incisors wider than centrals (right central has been purposefully reduced in width), flat incisal edges and interproximal contact points at the incisal corners. Note also characteristic features of mandibular canines: the labial surface in a) is divided into a mesio-labial surface of smaller width compared to a wider disto-labial surface by a labial ridge offset to the mesial

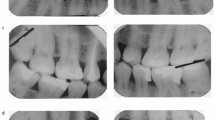
Mandibular canine anatomy: a) Gaillaedot appliance left canine (33) lingual view; b) Gaillardot appliance right canine (43) incisal view; c) left canine (33) schematic lingual view (grid = 1 sq mm); d) left canine (33) schematic view (grid = 1 sq mm). Images c) and d) reproduced with permission from Nelson S J, Wheeler's Dental Anatomy, Physiology, and Occlusion. 9th edition, 2010, Elsevier
When viewed as a mandibular artefact (Fig. 3), the pontics are the right central and lateral incisor crowns. To aid reattachment these are each perforated by two bucco-lingual holes, one at the tooth neck and one mid crown. Four abutments support the pontics: on the right side the canine, and on the left the central and lateral incisors, and the canine. In contrast to the Etruscan use of cold welded gold bands and riveted pontic2,3 teeth, the Phoenician artefact made use of the Egyptian technique of gold wire splinting.4,5,6 A gold wire encircles all teeth three times. It also passes interproximally and through the pontic holes at the necks, connecting abutments and pontics firmly together. A separate wire connector, laced two times through the mid-crown holes, binds the pontics together.
Since its discovery, the appliance has been subject to conflicting interpretations. This resulted from early misleading drawings (Fig. 1) and later, poor-quality black and white photographs, often flipped and flopped in publications. This was compounded by, with the exception of Filderman,7 a lack of physical examination of the appliance by later researchers. Consequently, there are three lingering questions surrounding the interpretation of the Gaillardot appliance:1,3,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28
- 1.
Are the pontic incisors foreign to the dentition? Renan (1864) identified the pontics as foreign, an opinion repeated by Van Marter (1886) and Lufkin (1948). Weinberger (1940, 1946) initially agreed but based on new Louvre photographs of 1947 in 1948 he limited 'foreignness' to only what he then identified as a maxillary lateral incisor. Ring thought both pontics were bone
- 2.
Have teeth been rearranged within the supporting gold wire framework? Weinberger claimed the four abutment teeth were removed at some time from the wire and incorrectly reinserted. He believed the narrow right central incisor was transposed with the lateral. Also, the canines had changed places, as revealed by distal incisal corners now on the mesial
- 3.
Is the appliance maxillary or mandibular? Beginning in 1864, many have argued for a maxillary setting: Renan (1864), Van Marter (1886), Farrar (1888), Guerini (1894, 1909), Deneffe (1899), Lemerle (1900), Godon (1901), Weinberger (1948), Hoffmann-Axthelm (1976). Similarly, a mandibular setting has had its advocates: Kirk (1909), Sudhoff (1926), Weinberger (1926, 1946), Filderman (1931), Brown (1934), Clawson (1934), Iskander (1979), Becker (1997), Schneider (2000), Blomstedt (2013). Weinberger, in 1940, managed to illustrate both settings in a single article.
Materials and methods
The new assessment of the Phoenician appliance is based on physical examination of the appliance at the Louvre, digital photography using a Canon 700D with a Canon 100 mm macro lens and ring flash, as well as texts of dental anatomy, occlusion and dental wear.
Results and discussion
Filderman believed the pontic teeth were foreign to the dentition because 'Leur teinte est bleutee, alors que les autres sont plutot jaunes.' and 'Elles ne presentment pas de stries horizontals';7 that is, they bore a blue hue in contrast to the yellow of the other teeth, and they lacked horizontal streaks. However, any perceived colour difference apparent in our macrophotography could be considered significant, and all teeth, including pontics, bear a common horizontal developmental groove (Fig. 3a). Use of autogenous teeth as pontics in Etruscan dental bridges was identified by Becker.5 In doing so, Becker anticipated our argument by stating: 'teeth, presumably loosened by periodontal problems or deliberately removed, could have been used. Such recycling of one's own teeth might also guarantee a correct colour and size match in the appliance'.5
All teeth are mandibular in form, confirmed by comparison with dental anatomy illustrated in Nelson (2010).29 Note in each of the Figure 4 images, characteristic features of mandibular canines contrast with those of maxillary canines and are also evidence that the canines are on their correct sides in the appliance. The lingual surface is smooth, lacking pronounced mesial and distal ridges as well as cinguli. In contrast to maxillary canines, the mandibular canines also lack a definite lingual ridge and so mesial and distal fossae, clearly apparent in Figure 4b. The mesial surface outline of the crown and root are nearly continuously straight, while the distal crown outline is longer than the mesial. The distal crown outline is convex in contrast to the straighter mesial outline. This contrasts with the maxillary canine, where both mesial and distal outlines are more convex. Although mesial and distal incisal cusp inclines have been lost through cusp wear, the red arrows in Figure 4b highlight the offset labial ridge and the relative proportions of the mesio-labial and disto-labial surfaces, as considered in Figure 3. In Figure 4c, the red arrows highlight the case of a pristine cusp whose incline lengths conform to the ratio of mesial one third to distal two thirds. The close adaptation of the bridge-encircling gold wire to the canines is seen in Figure 4b with the only gaps on the mesio-buccal and mesio-lingual aspects, as could be expected in such a technique.
Left central and lateral incisors have flat incisal edges with contact points at the incisal corners, and the lateral incisor is wider than the central incisor (Fig. 3a). The mandibular nature of the canine anatomy and correct right and left positioning of canines in the bridge is apparent in Figure 4. In the lingual view, the distal marginal ridge is longer than the mesial. Distal crown outlines are rounded, in contrast to the mesial outlines, while the mesial crown and root surfaces conform to a more continuous straight line. Also apparent is a flatter, smoother lingual surface lacking the cinguli and more pronounced mesial and distal marginal ridges of maxillary canines. The lingual ridge and accompanying mesial and distal fossae are also missing. Although the canine cusps have been lost through wear, the original proportions of a shorter mesial-incisal cusp incline relative to the distal can be appreciated (Fig. 4b). The unworn, anatomically ideal, mandibular incisal cusp incline ratios of mesial one third and distal two thirds are seen in Figure 4d.
Evidence of correct positioning of the canine teeth within the bridge is also seen in the close adaptation of the wire framework to the necks of the teeth, visible in incisal views (Figs 3c and 4b). The only gaps between canines and supporting wire are on the mesio-buccal and mesio-lingual aspects, where the wire loops encircling all teeth as one unit are not pulled fully in by the interproximal loops (see, for example, Figure 4b). In the authors' opinion, three encircling strands of wire would resist the close accommodation of transposed canines resulting in poorly seated teeth revealed by multiple gaps.
Mesial-distal measurements of the canines were recorded at the Louvre with a digital vernier caliper; 7.57 mm for both teeth, contrasting with Filderman's 1931 measurement of 8 mm. However, it was found in our examination that the teeth have at some time been painted with glue (visible in the macro images) which has imparted a rigidity to the appliance, apparent in handling. If Filderman removed the canines to take measurements, his recordings are likely more accurate than ours. We were aware of possible parallax error in viewing the teeth against the vernier, which could not be placed ideally against the interproximal surfaces. Measurements can be compared to Dewey's published averages for maxillary canines of 7.6 mm and 6.9 mm, and largest measurement of 9.5 mm, for mandibular canines.30
The degree of incisal cusp wear of the mandibular canines would have depended on the functioning lifetime of the teeth, ingestion of abrasives, food toughness, bruxing and parafunction. The angle of wear, however, is due to the mechanics of their occlusion with opposing maxillary teeth. Wear reduced the mesial height of the crown more rapidly than the distal. The angle of slope of the resulting incisal facet is the reverse of that seen in mandibular canine wear in Angle Class I occlusions.31 In our view, the dentition was most likely in an anterior Class III relationship whereby the mesio-incisal facet of the mandibular canine contacted the disto-incisal edge of the maxillary lateral incisor during mandibular movement. It must be noted that, throughout the process of canine wear, although the incisal cusp is lost the original ratio of a smaller mesio-incisal incline length to longer disto-labial length is reflected in the mesio-labial to disto-labial widths of the labial surface, as seen in the incisal view.
Mandibular masticatory movement in a fully protected occlusion can be conceptualised as traversing a path about 45° downward and laterally. In this cycle of movement, protection of the occlusion is imparted by a protective canine rise; this has been termed a vertico-lateral mandibular protective movement.31 With functional wear of the canines and loss of protective canine rise, the angulation changes visibly with age from 45° to a 'bovine' 0°, because of wear also on the distal ridges.31 In the authors' opinion, the amount of wear of the Phoenician canines indicates a mandibular path of movement midway through the lifecycle of a deteriorating occlusion.
Ancient and modern evidence from the Middle East suggests that an Angle Class III dentition and pronounced canine wear would not be an unexpected arrangement in the Phoenician dentition. Leek found that 'Class III cases and double proclinations are relatively common in Egyptian skulls… today it is an accepted clinical fact that Class III dentitions suffer severe attritions even though modern soft food is consumed'.32 In the ancient Middle East dentitions had to cope with diets higher in abrasives introduced by food preparation techniques,32,33,34,35,36 and with potentially tougher foods. For example, food hardness potentiates tooth wear through masticatory exertion. Muscular activity and masticatory movements can vary with food resistance whereby tough foods induce an increase in muscle activity and lateral jaw movements.37,38 Even in the absence of tough foods, Angle Class III occlusions routinely function with a pronounced lateral component of mastication.37 Background environment can also be a source of ingested abrasives. For example, Johansson found the content of airborne dust exacerbates the bruxing wear in modern Saudi youth; significantly, the bruxism loss is mostly confined to the canines and incisors.39
The fabricating artisan faced the problem of stabilising reinserted right central and lateral incisor teeth in a presumed crowded dentition. Presumption of such crowding in the Phoenician case is reasonable in the light of research showing dental crowding is most common in the mandibular anterior region, worsening with age.40,41 A classic Angle Class III skeletal arrangement often results in an anterior flat arch curve. Natural anterior crowding in this Phoenician case would have been accentuated by drifting of teeth associated with periodontal disease, a common condition in ancient dentitions.42 To maximise stability, rather than attempt to reproduce the original crowded arch, the artisan chose to narrow the pontic teeth. This facilitated flattening of the arch of the bridge, in keeping with the presumed occlusion of the upper arch.
The design embodied aspects of Etruscan and Egyptian dental techniques.12 This is very likely deliberate and a reflection of the cultural contacts and borrowings among these various peoples. Etruria very likely was the origin of the feasibility of replacing lost teeth. However, lacking the Etruscan technology of cold welding gold plate, the Phoenicians adapted what they had very likely already learnt from the Egyptians, the use of gold wire for splinting loose teeth.4,25
Conclusion
The Gaillardot dental appliance was fabricated to retain the reinserted mandibular right central and lateral incisor teeth that had probably succumbed to periodontal disease. The fabricating artisan reused the original teeth and, by reducing the width of the reinserted teeth, maximised bridge stability by eliminating the perceived crowding. A straightened, more mutually supporting tooth arrangement, would have lessened the load on supporting abutments, also most likely loosened by periodontal disease. The technique consequently produced the most stable result possible for both replaced teeth and abutments. If, as claimed, the abutment teeth had at some stage been removed from the appliance, they were returned to their correct positions, as indicated by the pronounced mesial-incisal wear of the canines; the reverse of that seen in the Angle Class I tooth arrangement due to the Class III nature of the Phoenician's occlusion. The precise adaptation of the encircling gold wire is also evidence of the correct positioning of the canine teeth. While aesthetics had been the primary function of Etruscan dental appliances,2,3 the Phoenician design produced the most effective dental appliance for mastication recovered to date from antiquity.
References
Renan E. Mission de Phénicie. [French] Paris: Imprimerie Imperiale, 1864.
Becker M J. Etruscan female tooth evulsion: gold dental appliances as ornaments. In Baker P A, Carr G (eds) Practitioners, Practices and Patients: New Approaches to Medical Archaeology and Anthropology. pp 238-259. Oxford: Oxbow Books, 2002.
Becker M J, Turfa J M. The Etruscans and the History of Dentistry: The Golden Smile through the Ages. London: Routledge, 2017.
Becker M J. Early dental appliances in the Eastern Mediterranean. Berytus 1997; 42: 71-102.
Becker M J. The Valsiarosa Gold Dental Appliance: Etruscan Origins for Dental Prostheses. Journal of the Etruscan Foundation 1999; 6: 43-73.
Becker M J. Etruscan Gold Dental Appliances Evidence for Early "Parting" of Gold in Italy Through the Study of Ancient Pontics. In Tsoucaris G, Lipkowski J (eds) Molecular and Structural Archaeology: Cosmetic and Therapeutic Chemicals. pp 11-27. Dordrecht: Springer Netherlands, 2003.
Filderman J. Notice sur une prothèse fixe, datant d'avant J-C. La Revue Odontologique 1931; 52: 335-343.
Van Marter J G. Further evidences of prehistoric dentistry. Independent Practitioner 1886; 7: 57-61.
Lufkin A W, Castro F M, Archer W H. A History of Dentistry. 2nd ed. Philadelphia, PA: Lea & Febiger, 1948.
Weinberger B W. Did dentistry evolve from the barbers, blacksmiths or from medicine? Bull Hist Med 1940; 8: 965-1011.
Weinberger B W. Further evidence that dentistry was practiced in ancient Egypt, Phoenicia and Greece. Bull Hist Med 1946; 20: 188-195.
Weinberger B W. An Introduction to the History of Dentistry. St. Louis, MO: The C V Mosby Company, 1948.
Ring M E. Dentistry: An Illustrated History. New York: Harry N. Abrams, 1992.
Farrar J N. Treatise on the Irregularities of the Teeth and Their Correction I. London: The International News Company, 1888.
Guerini V. L'Odontologic. In Asbell M B Specimens of the Dental Art in Ancient Phoenicia (5th-4th Century B.C. Bull History of Medicine 1948; 22: 812-821, 815.
Guerini V. A History of Dentistry: From The Most Ancient Times Until The End Of The Eighteenth Century. Philadelphia: Lea & Febiger, 1909.
Deneffe V. La prosthése dentaire dans l'antiquité. [French] Anvers: H. Caals, 1899.
Lemerle L. Notice sur l'historie de l'art dentaire, depuis les temps les plus recutés jusqu'à nos jours suirie du catalogue de l'exposition rétrospective de l'art dentaire organisée par l'école dentaire de Paris à l'exposition universelle de 1900. [French] Paris: Paris Bureau De L'Odontologie, 1900.
Godon C. L'évolution de l'art dentaire. L'Ecole dentaire, son histories son action, son avenir. [French] Paris: Librarie J-B Bailliére et fils, 1901.
Hoffmann-Axthelm W. Zahnprothetik im Ägypten: ein archäologische Tatsache? Quintessenz [German] 1976; 27: 155-163.
Kirk E C. An added footnote to Guerini 1909:30, in Weinberger B W. 1948: 102
Sudhoff K. Geschichte der Zahnheilkunde. [German] Leipzig: J A Barth, 1926.
Weinberger B W. Orthodontics. An Historical Review of Its Origins and Evolution. St. Louis, MO: C V Mosby Company, 1926.
Brown L P. The Antiquities of Dental Prosthesis (Part 1) To the Close of the Fifteenth Century, A. D. Dental Cosmos 1934; 76: 828-836.
Clawson D. Phoenician Dentistry. Beirut: The Museum of Archaeology of the American University of Beirut, 1934.
Iskander Z, Harris J, Farid S. Further evidence of dental prosthesis in ancient Egypt. Ann Serv Antiq Egypte 1979; 63: 103-113.
Schneider H. La prosthèse dentaire dans l'Antiquité. [French] Paris: Universite Rene Descartes, 2000. Available at http://www.biusante.parisdescartes.fr/ressources/pdf/histmed-asclepiades-pdf-schneider.pdf (accessed May 2019).
Blomstedt P. Dental surgery in ancient Egypt. J Hist Dent 2013; 61: 129-141.
Nelson S J. Wheeler's Dental Anatomy, Physiology, and Occlusion. 9th ed. Philadelphia, PA: Elsevier Health Sciences, 2010.
Dewey M. Dental Anatomy. St. Louis, MO: C V Mosby Company, 1917.
Darveniza M. Full occlusal protection - theory and practice of occlusal therapy. Aust Dent J 2001; 46: 70-79.
Leek F F. Bite, Attrition and Associated Oral Conditions as Seen in Ancient Egyptian Skulls. J Hum Evol 1972; 1: 289-295.
Murray M A. Cereal production and processing. In Nicholson P T, Shaw I (eds) Ancient Egyptian Materials and Technology. pp 505-536. Cambridge: Cambridge University Press, 2000.
Pain S. Why the pharaohs never smiled. New Scientist (London) 2005 June 29. Available at https://www.newscientist.com/article/mg18625061-900-why-the-pharaohs-never-smiled/ (accessed May 2019).
Fields M. Book review: An appraisal of the skulls and dentition of ancient Egyptians, highlighting the pathology and speculating on the influence of diet and environment, J. Miller, ISBN 9781407302829. Int J Osteoarchaeol 2009; 19: 443-445.
Forshaw R J. Dental health and disease in ancient Egypt. Br Dent J 2009; 206: 421-424.
Pröschel P, Hofmann M. Frontal chewing patterns of the incisor point and their dependence on resistance of food and type of occlusion. J Prosthet Dent 1988; 59: 617-624.
Komino M, Shiga H. Changes in mandibular movement during chewing of different hardness foods. Odontology 2017; 105: 418-425.
Johansson A, Fareed K, Omar R. Analysis of possible factors influencing the occurrence of occlusal tooth wear in a young Saudi population. Acta Odontol Scand 1991; 49: 139-145.
Shigenobu N, Hisano M, Shima S, Matsubara N, Soma K. Patterns of dental crowding in the lower arch and contributing factors. Angle Orthod 2007; 77: 303-310.
Little R M, Wallen T R, Riedel R A. Stability and replapse of mandibular anterior alignment first premolar extraction cases treated by traditional edgewise orthodontics. Am J Orthod 1981; 80: 349-365.
Forshaw R J. The practice of dentistry in ancient Egypt. Br Dent J 2009; 206: 481-486.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Maccheroni, M., Darveniza, M. Reinterpretation of a Phoenician dental appliance. Br Dent J 226, 985–988 (2019). https://doi.org/10.1038/s41415-019-0413-5
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-019-0413-5
