
Abstract
Background The aim of this study was to explore the experiences of dental associates and how these relate to their working environment.
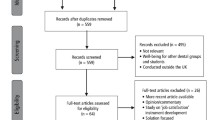
Methods Qualitative methodology was used. Semi-structured interviews were conducted with 11 associates in the UK in early 2018. Participants were asked about their working experiences, professional autonomy and the improvements they thought could be made to their working environment. Interview transcripts were analysed using deductive thematic analysis.
Results Three key themes were identified: 1) 'conditions', how associates view their working environment; 2) 'drivers', what associates believe drives their working conditions; 3) 'effects', how associates are affected by their working environment. There were differences between the working environments of associates working in corporate practice and those in independent practice. They relate primarily to decision-making and finances. While most associates enjoyed their job, a common factor that negatively affected associates was governance including the current NHS contract and actions of the General Dental Council.
Discussion The results of this study indicate that associates and the profession face a variety of issues today. The effects this has on associates could contribute to the changes that are being seen in the profession and are explored using social psychology theories.
Conclusion The findings of the study complement work demonstrating corporate associates to have lower levels of autonomy than their non-corporate peers and highlights that drivers vary between sectors. Social psychology theories indicate that the working environment could be affecting change in the profession.
Similar content being viewed by others


Key points
-
Demonstrates that associates believe different aspects drive the working environment dependent on sector.
-
Illustrates how associates, irrespective of sector, can be affected by the same factors.
-
Describes how the working environment could influence changes to the dental landscape.
Introduction
General practice-based dental care in the UK, both private and NHS, is largely provided by independent practitioners. In August 2018, 10,509 locations were registered with the Care Quality Commission (CQC) as primary dental care providers.1 While it has been some time since the restrictions on dental corporates were lifted, little is known about the influence corporates have had on associates, as this area is under researched. A clearer understanding of the working experiences of dental associates and how they are affected by the expansion of corporates would allow associates to be better supported and ultimately improve working conditions. This study aimed to address the lack of understanding by exploring the working experiences, and opinions, of dental associates and how these relate to their working environment.
Legislation aimed at opening the dental market to competition and increasing options for raising funds for dental practices has led to an increase in the number and size of dental multiples. NHS dental contracts in England are awarded through procurement processes, with NHS England local teams commissioning for the services they require. Government tendering in the UK has been under the spotlight due to failures such as the collapse of Carillion, which received £1,719 million in revenue from the UK government in 2016.2 Their collapse launched a Public Administration and Constitutional Affairs Committee inquiry into how the government and public sector manages the risks of outsourcing the delivery of public services.3 The inquiry will look at how the government and public sector make decisions about sourcing the delivery of public services, including the risks of concentrating a large number of contracts with a single company. Despite corporate entry into health care being controoversial,4 and the current uncertain financial and political landscape, the dental market in the UK continues to consolidate. For example, a pan European dental body corporate (DBC) moving into the NHS, with practices in Norway, Sweden, Finland, Denmark, Germany, Switzerland, Italy and the UK.
Dentistry is not the only profession in the UK to be facing challenges due to a relaxation of regulation. An insidious culture has developed in pharmacy, a field that was opened to competition in 2005, with reports of the sector becoming more business focused and target driven,5,6,7 pharmacists being put under commercial pressures by their employers,8 working in a more stressful environment,6,7 increasing role conflict,9 autonomy preclusion,10,11,12 and potential deprofessionalisation.11,13,14,15 Work with dental associates has shown similar effects. While some aspects are constant between the independent and corporate dental sectors, others differ. Overall, associates working in a corporate environment expressed significantly lower levels of morale, decision-making capabilities and autonomy.16
This study works to provide a deeper insight of the earlier results to aid understanding of the working environment of associates. Associates from the UK were interviewed and the resulting data analysis is described and summarised. Attempts are made to theorise its significance and implications in relation to the available literature and current dental landscape.
Methods
Study design
Semi-structured interviews analysed thematically.
Selection of participants
Participants were recruited via British Dental Association (BDA) publications, social media and professional networks, with participation not limited to association members. Interested parties were asked to contact us and were subsequently contacted by email or telephone to arrange a convenient time for interview. Selection criteria were intentionally left broad with the only restriction being that participants had to have experience of working as an associate in the UK. Participants were informed that the study was being conducted to gain further understanding of associates' working experiences and how these relate to their working environment.
Procedures
Interviews were conducted by telephone and digitally recorded, with all participants assigned a pseudonym. The interview schedule was developed based on previous work, existing literature and discussion. Questions within the schedule were open-ended, with prompts provided to encourage participants. Interviews lasted between 19 and 76 minutes. The interviews consisted of four main sections: clinical autonomy, role conflict, working life/experiences, and how working life could be improved. Each interview included the question 'Could you describe your working life?' This purposely broad question allowed participants to raise aspects most relevant to their experiences without being steered in a particular direction. Follow-up questions were asked for clarification or to address aspects of interest. For this study, a dental corporate was classed as a sole trader/partnership or incorporated company operating three or more dental practices.
Data analysis
Thematic analysis, as defined by Braun and Clarke, was employed with their six-step process being followed.17 Theoretical thematic analysis was carried out, driven by earlier work and a desire to further explore previously identified areas. Theoretical analysis allows data to be mapped to specific questions, with these questions evolving during the coding process. Themes were primarily identified on a sematic level with the researchers subsequently looking beyond participants' responses.
As we aimed to understand the themes that emerged from associates relating to their working environments, we have not given, nor did we quantitatively analyse, the number of participants within each theme. In places we have used terms such as 'commonly' or 'majority', to indicate more than 50% of participants, and 'few' to indicate less than 20% of participants.18 This allows for some meaning to be derived from the data and for information to be documented, interpretations or conclusions to be tested, and participant experiences to be represented.
Results
Characteristics of study subjects
Eleven associates agreed to be interviewed, with Table 1 summarising participant demographics. Interviewed associates had experience in sectors including the armed forces and maxillofacial surgery, some had previously owned practices while others had EEA qualifications and been recruited from abroad. Some worked within more than one craft, for example, general practice and the community dental service, while others had experience in more than one corporate (Table 2). NHS caseload varied among participants from 0% to 100%. The reasons for participating in the study for corporate and non-corporate associates were similar. They wanted their voices to be heard and felt their experiences could help improve working conditions for associates.
Outlook
Despite the role being described as stressful, unpredictable, frustrating and a challenge, the majority of associates enjoyed their job and felt dentistry in the UK was a good profession. Two sub-themes were identified when exploring associates' enjoyment of their job: personal and professional factors. Personal factors included job security, financial issues and job satisfaction while the one professional factor was identified as patient-related aspects. 'I've built up a good rapport with those patients; some of them I would call friends now as well and it's nice to treat those patients and see how their lives are going.' Loki L on their patients.
Identified themes
Three themes were identified relating to the working environment of associates these were:
Conditions: how associates view their working environment
Drivers: what associates believe drives their working conditions
Effect: how associates are affected by their working environment.
Conditions
Expectations
While the majority of associates enjoyed their job, they felt their expectations had not always been met. The main theme was career progression, with associates, irrespective of sector, feeling their careers had stagnated with no reward for enhancing their skills or room for progression in general practice. There was a disparity between the expectations of non-corporate associates and non-UK graduates recruited from abroad into the corporate sector. One sub-theme was identified relating to the expectations of this group and this was dishonesty, with associates feeling exploited and lied to. Working conditions were worse than expected for those in this group while non-corporate associates recognised the risk. 'I would say that there's a huge risk with that, you're taking effectively lambs and slaughtering them'. Charles X, on overseas dentists being directly recruited into corporate practice.
Erosion
Associates commonly highlighted an erosion, or decline, in relation to their remuneration as well as culture, standards, autonomy and investment into practice estate. Longer serving associates described a general erosion of the profession in terms of their working experience, with long-serving corporate associates chronicling, for example, an accumulation of disrepair due to lack of investment in maintenance of practice real estate and a fall in the level of experience of dental nurses. Respect for associates had declined over time, with this being linked by some to the oversupply of associates in some areas.
'When we sold the practice in 2002… I think things were a little bit different then, to how they are now and the climate has changed so much and we did have a fair bit of autonomy then. It was still not as much as we had when it was our own practice'. Clark K, on erosion.
'There's a general slide to devalue but I think it has a knock-on effect because then you stop meeting as equals and you don't have the same relationship with the practice as perhaps you did, yeah'. Jessica J, on erosion.
Support and persecution
Divergence was seen between associates in relation to how supported they felt and what they felt persecuted by. Aspects such as feelings of persecution by the GDC were shared by the majority of associates in both sectors, but corporate associates cited their agreements as a further cause and felt less supported than their non-corporate colleagues. Public perception of the profession was also mentioned, with associates not believing the profession to have a good public face. Defensive dentistry which was practised due to fear of litigation, was also referenced. Bureaucracy and micromanagement was a further sub-theme.
'I think once patients have that trust in us and once patients have that respect essentially for us, I think we, as dentists, would feel less challenged and wouldn't need to do as much what we call "defensive dentistry" and we'll be able to provide a lot more treatment and be able to offer all the range of treatments'. Scott S, on defensive dentistry.
'I think they'd like to micromanage everything, so from rotas to our ordering to our appointment system, I think they like to have a firm control over everything but you can't control everything and the personal aspect is out of the window and I think you lose certain benefits that way, if that makes sense'. Barry A, on being controlled by a corporate provider.
Autonomy
There was clear disparity between those in corporate and non-corporate environments in relation to autonomy. Associates with experience in both sectors acknowledged the non-corporate environment generally offered a greater level of freedom than corporate environments, in relation to the clinical and non-clinical decisions they were able to make. All but one corporate associate was limited by approved lists for the materials and laboratories they were able to use, and in some cases where referrals could be made, while those in non-corporate practice were not. Corporate associate agreements were mentioned and what was seen to be the dishonest promises in relation to clinical decision-making, and in some cases systems pressured associates into making specific decisions. Clauses in corporate agreements included not discussing working conditions and being prohibited from informing patients and staff that you're leaving or the reasons why. 'I don't think they have as much autonomy in terms of the clinical decisions from what I've heard'. Kara Z, on clinical freedoms in corporate practice. 'We're always told in our contract that you'll have full clinical freedom but actually that's not the case anymore. We don't have the same clinical freedom that we used to have'. Charles X, on corporate agreements.
'From a material point of view, we are given, I suppose, the freedom to choose materials but actually there's not really too much freedom, apparent freedom, because there's a certain list we have to choose from and even if the list has lots of items then if we want to choose something we always are restricted by the budgets that are allocated to the practice. So, not good freedom for materials'. Sara L, on professional autonomy in the corporate environment.
Changes
All associates identified changes that they felt would improve their working environment. Common to both sectors was governance. For those who provided NHS treatment this covered changes to the NHS contract and the NHS more generally. NHS, mixed and private associates cited changes to the GDC, who were suggested to be making it harder for dentists to practise and being overzealous in their pursuit of disciplinary issues. Associates would like to see changes in their progression structure to make it easier to progress with their careers. The often negative public perception of the profession was also raised and improving this was seen to be a benefit as was the perception of associates by the profession. One difference between the sectors was corporate associates wished to see a change from profit being the priority. 'They're actually trying to make their [the dentist's] work more difficult than it is.… that includes all sorts of regulators of this category'. Selina K, on the GDC. 'Having more of a set training pathway or training goals as to how we can progress as dentists'. Loki L, on changes to career progression.
'The biggest thing I would like to change, which I think is near enough impossible, is for the patient's or the public's perception of dentistry, because I think they feel it's a necessary evil and what they don't necessarily consider or value is the actual, the quality and the benefit of having good oral health, good teeth and also effectively paying to have treatment that's going to potentially save your teeth and improve your quality of life'. Scott S, on public perceptions.
Associates suggested how they thought the profession might change as time progressed. Some suggested that working environments might improve due to events such as Brexit and a possible fall in the supply of associates, while others suggested deterioration. The current level of clawback indicated that corporates may be changing their business model and led to questions of if the corporate model was shifting from NHS dentistry due to a struggle to make a profit and, if this was the case, what it meant for the sector as a whole.
Advice
There were differences in the advice associates would give to recent graduates or those wishing to enter the profession. Most corporate associates did not recommend working in the corporate environment, though it was acknowledged that the working environment in non-corporate practice was dependent on the practice owner, and non-UK graduates would not advise coming to the UK or working within the NHS. Similarly, there would be advice against joining the profession from some non-corporate associates. Common pieces of advice were to find areas the associate liked or excelled at and to continue with professional training.
'Do your FD training, try and find a practice that's going to be supportive and there are going to be people at the practice who are going to be able to informally mentor you. Start to try and look for your postgraduate training so that you can then at some point perhaps slot into a job that's going to require that. If partnership offers itself, all well and good, you might want to go consider that'. Charles X, on advice to a new UK graduate.
'I'd ask them to just think very carefully about their decision, if they do intend to apply for dentistry and just to make sure they're aware of what they're letting themselves in to. I'd be half in mind to sway them against going into dentistry, unless they were well aware of the climate and the issues that we face'. Scott S, advice for a new dentist.
'I think it's a good career. It's a very secure career because we're very short of dentists. I think for the right sort of person who takes satisfaction out of doing the job, it has a lot to offer. For somebody who just wants to get rich, I think they'd find it quite challenging. It had a reputation of being a way to get rich quickly and as various new techniques have come in that was the way to make money. I think it still has a lot to offer as a career but it is a challenge. My daughter did her work experience with us and she said at the end of the week "well yes, I think I could do that, but I don't want to have to work that hard"'. Steve R, advice for a new dentist.
These conditions are presented in Figure 1.

How associates view their working environment (conditions)
Drivers
Associates identified a number of drivers that they believed dictated their working environment. All of which can be related to the ethos or philosophy of those in control, with the importance of each factor varying by sector. For corporate associates the dominant driver was finance, followed by corporate reputation and for non-corporate associates the personality of the practice owner. Associates in non-corporate practices, while recognising their freedoms were dependent on the practice owner, felt aspects such as practice goodwill and relationships were driving forces. Finances were a driver in the non-corporate setting but this focused on investment into the practice rather than profit, with some of this thought to be due to practice owners working in the practice and therefore having a more personal stake. 'Without doubt it's the bottom line, the financial bottom line'. Charles X, on what drives decision-making in a corporate practice.
'I think he sets the example and then he obviously lets that example be a way for other people to aspire to and therefore I think in order to do that, he's well aware if he was in [name redacted] shoes, he would want that same level of autonomy, so it's also the level of respect, professional respect to the colleagues that he delivers'. Scott S, on why he has the freedoms he has. 'It's about your relationship with your principal, isn't it?'. Kara Z, on what drives clinical freedom
Associates with freedom had the trust of their practice owner and owners were felt to invest in, and value, relationships with their staff, patients and community. Additionally, setting an example for their associates and having an understanding of how things work. While the bottom line was important in both sectors, the relevance of success verses profit varied.
'If you own your own practice and the goodwill of that practice, because it's a practice in a local community, means a lot to you, you want people who generate goodwill and you want, overall you want that practice to keep that goodwill turning over, keep patients happy, keep patients coming, keep the reputation of the practice good, those things are things that are important to practice principals because it's their business, it's their patients and they need that practice to be successful'. Jessica J, on investment by the principal.
The level of control held by corporate associates appeared to be partially driven by the level of power, or position, the associate held in the practice. Previous practice owners who had sold their practice to a corporate provider and subsequently worked as an associate in that practice described greater levels of freedom, as did those who were the sole clinician, and possibly the main income generator, at a site.
These drivers are presented in Figure 2.

What associates believe drives their working conditions (drivers)
Effect
Associates in both sectors realised and acknowledged, they, in essence, worked for a higher power, with some describing how their environment affected them. Some corporate associates felt they were part of a collective rather than an individual practice. Some raised the issue of what effect their working environment and curtailed decision-making had on their working experience, with two having gone as far as resigning from a post. This sentiment was expressed by others as being the intended course of action should the situation ever arise. Associates felt devalued and in some cases suffered ill effects, including stress and anxiety, with some seeking therapy due to the effect their work had on them.
'When they recruit you, they present you with a dream career job and when you come here it's absolutely totally different… I underwent psychotherapy and I am having psychotherapy every week to deal with my life, to learn certain ways of seeing things'. Sara L, on being recruited from abroad.
The effects on the profession of associates not being permitted to make decisions were covered, with the possible impact on self-employed status being raised. The loss of professional expertise was highlighted with the knowledge of associates being lost. This was not only thought to be the case for long experienced associates and previous practice owners, but also for more recently graduated clinicians who had benefited from training in things that older associates hadn't such as practice management. Having clinical freedom was also seen as a benefit for patients and the experience of an associate as a patient in the corporate sector supported this, with the associate who had been treated in corporate practice feeling lied to and not valued. 'Having your own autonomy, you feel you can give the best service to the patients'. Loki L, on the benefits of autonomy for patients.
Internal conflict
All associates felt internal conflict, with a common sub-theme in NHS and mixed associates being governance. This covers the current NHS contract and the pressure to balance patient need and the units of dental activity (UDA) system. This professional versus business conflict showed divergence with corporate associates and their responsibility to the corporate, causing associates to be asked to upsell or push treatments they felt were inappropriate. Self-preservation was identified as one reason why associates did not raise issues when they felt there could be a problem. This was accompanied, for corporate associates, by the remote nature of the management structure, resulting in it being difficult to raise issues and also the suggestion that issues when raised were lost or ignored. For non-corporate associates, the relationship between associate and practice owner were important factors for raising issues.
'Like any other associate you have in the back of your mind your UDAs and you need to achieve your target, so that's the thing that sometimes influences your decision but it shouldn't influence it that much because that's not very ethical'. Jean G, on the UDA system. 'So, you have to pick and choose some of your battles about what you, what you decide to really fight against'. Scott S, on raising issues. 'Let's say I raise an issue, the issue just gets lost on the way or it's even covered up, like maybe from the practice manager or from another manager that's on top of them, that they don't want problems on top'. Selina K, on raising issues in corporate practice.
Perceptions
Associates who had non-corporate experience only were reluctant to work in the corporate sector, with corporates being known through reputation and peers. Non-corporate associates perceived the corporate sector to be self-serving and corporate associates to have a comparatively lower level of job satisfaction and a lack of autonomy. 'These corporate organisations that don't seem to care about us as dentists or us as people; all they're concerned about is getting UDAs done at the lowest rate possible and then it's, I think job satisfaction is poor'. Loki L, on corporate practice.
Discussion
As far as the authors are aware, this is the first study to explore dental associates' perceptions of their working environment in relation to the sector of general practice in which they work. Our study confirmed previous results of associates working in corporate environments feeling less autonomous than those in independent practice,16 and determines the factors they believe influence their ability to make decisions, undertake their work, and how this could impact on the profession.
Working environments
The differences expressed by associates in this study reflected previous work that quantified the relative loss of autonomy and decision-making abilities of corporate associates in comparison to those working in independent practice. This expanded to include aspects such as corporate reluctance to maintain practice premises and professional equipment that impacts on the day-to-day functioning of the clinic and associates' working life. The main driver, as seen by corporate associates, was finance, with all decision-making seen to be based on profit. While associates in this sample overwhelmingly expressed their dislike for corporate dentistry, similar sentiments were expressed by some associates for the independent sector. Though this was the exception, it is apparent that some practice owners do limit the autonomy and freedoms of associates, but understandably, to a lesser extent. A common opinion from current non-corporate associates was that they would not work for a dental corporate based on the reputation for curbing associate freedoms and being driven by profit.
Loss of autonomy in a corporate environment is not unexpected. Processes are employed to allow the corporate to operate in a profitable manner and, as the business expands, the amount of bureaucracy necessary to organise the workplace and maximise profits increases.11,19 Taking the UK pharmacy sector, which has seen corporate investment in a more open market since 2005, as a comparator, corporate investment could be described as being detrimental to the profession. As well as formally documented changes,5,6,7,8,9,10,11,12 reported effects on the workforce are similar to that of associate dentists, with pharmacists working in a leading UK corporate chain reporting a relentless drive for profit at their expense.20
How the working environment affects associates
Social psychology is called on to offer a novel way to describe the effects of associates' working experiences and environments. The profession is changing, and these changes could be described as being affected by factors such as cognitive dissonance, social contract negation and driven by governance aspects, as well as corporate pressures.
Conflict of interest and cognitive dissonance
The system associates work in has an inherent conflict of interest (COI), as is the case for other healthcare systems.21,22 Associates are faced with decisions that could challenge their altruism, as personal values are pitted against the values of the system. Associates with NHS experience recognise that the current contract may compromise practice and this could be compounded by corporate involvement, because, in addition to meeting a UDA target, there could be added corporate pressures. While COI creates a risk of bias that can affect judgement and, at its worst, lead to dishonesty, problems only arise when clinicians allow personal interest to bias their judgement and affect their patient.22,23
The current contract could potentially undermine associates' moral identity as altruistic practitioners and introduce discomfort. Should this arise, they should be motivated to resolve this dissonance. Originally, cognitive dissonance theory suggested that when people are faced with discomfort due to conflicting cogitations, that is behaviours, attitudes or emotions, they are motivated to decrease the discomfort, or tension, the conflict causes.24 To resolve the discomfort people have been suggested to do one of three things:
Changing behaviour to tie in with their beliefs/values; for example, an associate leaving their job
Justifying the behaviour; for example, an associate accepting their job has problems but saying this is fine as I am helping people
Changing belief(s); for example, an associate believing profits should be placed over patients.25
Should associates choose to change their behaviour to tie in with their beliefs/values there could be sizable consequences both for associates and patients. On a personal level, associates need to work and if they choose not to work for corporate providers they could find it difficult to practise due to issues such as associate oversupply in certain areas. An exodus of associates from corporate practice would cause a problem in providing dental services, but as IDH alone, for example, held 643 UK practices,26 it would be unlikely for a large enough number of associates to simultaneously leave their practice due to workplace conditions.
Less drastic changes in behaviour, such as rationalising or changing beliefs, could be more damaging to associates as well as the profession. Associates in this study do not feel respected or valued, and corporate associates disempowered. Looking at this, in conjunction with social contract theory, associates could believe they are no longer being offered the terms of their social contract by society, or the profession, and may change their behaviour to compensate, leading to changes within the profession.27 A social contract is a philosophical term used to explain certain structures in society by analogy to legal contracts between individuals. For dentists, this denotes an agreement between the profession and the public with the basic premise that in exchange for the ability to alleviate suffering related to oral disease, society bestows certain benefits such as a higher than average income, respect and status with professional autonomy described as an important element.27
When dentistry was established as a profession in the early 20th century, professionalism had been suggested to be what some have termed 'nostalgic', with dentists placing the highest values on aspects such as altruism and personal morality.27,28 With recent changes such as an increasing focus on aesthetics and the growth of corporates, nostalgic professionalism has been suggested to be being replaced by other forms, including entrepreneurial professionalism, that place higher value on factors such as commercialism and less of an emphasis on altruism.27,28 This suggestion is not limited to dentistry, with physicians suggested to be dissatisfied with how society is reneging its side of their social contract and also bemoaning a loss of autonomy and respect.27
Cognitive dissonance was evident in this study; all associates reported enjoying their job but described their working environment/lives in negative terms, with the majority working in environments that negatively influenced the way they are able to work. This fits with literature exploring workplace environments that indicates, despite high levels of workplace stress, social workers, for example, experience relatively high levels of job satisfaction.29 This study did not explore dissonance nor its resolution but associates were mindful of conflict and detailed how they managed it. Everyone experiences cognitive dissonance but there is the suggestion that those in certain professions experience the phenomenon more frequently and with deeper ramifications.25
Improvements
All associates suggested ways in which they felt their working environments could improve. Those who worked in, or had experience of, the NHS, felt the system was not fit for purpose and, irrespective of work sector, saw NHS contract reform in England to be a positive move. The current NHS contract was seen as an impediment to good practice. The associates with experience of working under the pilot and prototype 'blend A' contracts provided additional insight into this and while they were positive towards the pilot contract and the emphasis it allowed to be placed on prevention, they expressed dismay and concerns over the time available to treat patients and associates payment relating to the prototypes. This is not an isolated view, with discussions on the issue highlighting that while pilots were seen as promising, as they placed emphasis on prevention and did not use UDAs, the introduction of the prototypes was disappointingly placing associates under increased pressure. Furthermore, the reintroduction of activity led to a feeling of being back on the treadmill and the prevention message being diminished.30
Moving forward
Whichever way associates choose to manage the tension their working environment induces, cognitive dissonance is recognised as being a powerful motivator for change31 and is suggested to be a contributor to the acceptance of suboptimal care.32 Looking at the working environment, the way in which it has and continues to change, as well as how it affects associates, could indicate that corporatisation is one of the main drivers changing the profession. Under current economic constraints, and with continuing market consolidation, it seems probable that the working environment of all associates will erode. It is important that this is recognised by both commissioners and providers, and that subsequent strategies take into account a healthy and safe working environment for staff.33
This paper explores the experiences of dental associates and how these relate to their working environment. The number of associates being interviewed was small, and while the study only touches the surface of a problem within the profession there were clear themes emerging from the interview process. Those interviewed were derived from a purposive sample, with the study aiming to capture the experiences, beliefs and opinions instead of providing a quantitative summary of findings.
Limitations
There is a degree of subjectivity involved in this study, which may be complicated further by the interviews being conducted and coded by a sole researcher and, consequently, from a single perspective. Using a single researcher to conduct and code all interviews could be advantageous, and in some cases is preferred, as the researcher will be fully immersed in the data and have a unique relationship with participants.34 As some recommend that coding involves more than one researcher,34 and for rigour and validity,35 initial codes were cross-checked by VC in discussion with EO and subsequent themes developed. With limited research in the area of dental associates' working environments, and VC's limited prior experience within this area, VC was able to approach the data with an open and relatively unbiased perspective. Efforts were also made to compare findings with existing research results in related, similar settings, such as pharmacy, both in the UK and internationally.
Recruited participants reflected a range of demographics, experience and opinion, but the findings may only reflect the views of this specific set of associates. Selection bias may have been introduced through participants self-selecting and while it is possible that the issues identified and opinions shared are particular to this group, this can only be discounted by repeating the study. The depth of data, with the majority of participants reporting similar opinions and experiences, indicate that this, and the small sample size, may not be a concern. While the sample size for this study is small, qualitative work with an identical,36 or smaller,37,38 sample has been published.
Despite these limitations, this study expands the existing literature, providing a novel insight into associates working conditions across sectors, and the findings link to those of others looking at corporate involvement. The findings will help to develop associates working environments and enhance practice, though more research is required to determine the influence that the working environment has on associates and the wider effects.
Conclusion
This research has focused on exploring the experiences of associates and how these relate to their working environment. Corporate and independent dental associates similarly report enjoyment of their job, while experiencing cognitive dissonance but many also feel overloaded, stressed and undervalued by others. The study findings complement earlier quantitative work demonstrating corporate associates to have lower levels of autonomy than their non-corporate peers and highlights that associates in the corporate sector believe profit drives decision-making, with this differing from those in the non-corporate sector. Social theory indicates that the working environment could be affecting change in the profession. NHS contract reform is important for improving the working environment of NHS associates while those in the corporate sector would benefit from a shift from profit being the foremost consideration. Associates would also benefit from positive interaction between the profession and the regulator, the Department of Health, and commissioners. With stress in dentists currently high compared to national averages and teachers, and psychological distress higher in dentists than vets and GMPs,39 all avenues to improve their working conditions should be considered.
References
Care Quality Commission. Using CQC data. 2019. Available at https://www.cqc.org.uk/about-us/transparency/using-cqc-data (accessed April 2019).
Carillion. Making tomorrow a better place: Annual Report and Accounts 2016. Available at https://www.companyreporting.com/sites/default/files/annual-report-index/carillion-annual-report-2016.pdf (accessed April 2019).
Commons Select Committee. The collapse of Carillion inquiry launched. 2018. Available at https://www.parliament.uk/business/committees/committees-a-z/commons-select/public-administration-and-constitutional-affairs-committee/news-parliament-2017/lessons-collapse-carillion-inquiry-launch-17-19/ (accessed April 2019).
Robbins C J, Rudsenske T, Vaughan J S. Private equity investment in health care services. Health Aff (Millwood) 2008; 27: 1389-1398.
McDonald R, Cheraghi-Sohi S, Sanders C, Ashcroft D. Professional status in a changing world: the case of medicines use reviews in English community pharmacy. Soc Sci Med 2010; 71: 451-458.
Jacobs S, Hassell K, Ashcroft D, Johnson S, O'Connor E. Workplace stress in community pharmacies in England: associations with individual, organizational and job characteristics. J Health Serv Res Policy 2014; 19: 27-33.
Jacobs S, Hassell K, Ashcroft D, Johnson S, O'Connor E. Perceived causes and effects of workplace stress in community pharmacy: findings from a postal survey of community pharmacists. Int J Pharm Pract 2011; 19 (Spec Iss): 100-101.
Murphy J A. Employers applying pressure to conduct MURs. 2007. Available at https://www.pharmaceutical-journal.com/opinion/correspondence/employers-applying-pressure-to-conduct-murs/10004867.article (accessed April 2019).
Perepelkin J, Dobson R T. Influence of ownership type on role orientation, role affinity, and role conflict among community pharmacy managers and owners in Canada. Res Social Adm Pharm 2010; 6: 280-292.
Harding H, Taylor K. The McDonaldisation of pharmacy. Pharm J 2000; 265: 602.
Bush J, Langley C A, Wilson K A. The corporatization of community pharmacy: implications for service provision, the public health function, and pharmacy's claims to professional status in the United Kingdom. Res Social Adm Pharm 2009; 5: 305-318.
Dobson R T Perepelkin J. Pharmacy ownership in Canada: implications for the authority and autonomy of community pharmacy managers. Res Social Adm Pharm 2011; 7: 347-358.
Taylor K, Harding G. Corporate pharmacy: implications for the pharmacy profession, researchers and teachers. 2003. Available at http://pharmacyeducation.fip.org/pharmacyeducation/article/view/38 (accessed April 2019).
Sidu A. Glorified shelf stackers? Pharm J 2003; 270: 152.
Ritzer G. The McDonaldization of Society. 8th ed. Thousand Oaks, CA: SAGE Publications, 2014.
O'Selmo E, Collin V, Whitehead P. Associates and their working environment: a comparison of corporate and non-corporate associates. Br Dent J 2018; 225: 425-430.
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006; 3: 77-101.
Neale J, Miller P, West R. Reporting quantitative information in qualitative research: guidance for authors and reviewers. Addiction 2014; 109: 175-176.
Queen's University Belfast. The dynamics of bureaucracy. Available at https://www.qub.ac.uk/schools/media/Media,291460,en.pdf (accessed April 2019).
Chakrabortty A. How Boots went rogue. The Guardian (London) 2016 April 13.
Larkin I, Loewenstein G. Business Model-Related Conflict of Interests in Medicine: Problems and Potential Solutions. JAMA 2017; 317: 1745-1746.
McCoy M S, Emanuel E J. Why There Are No "Potential" Conflicts of Interest. JAMA 2017; 317: 1721-1722.
Lo B, Ott C. What is the enemy in CME, conflicts of interest or bias? JAMA 2013; 310: 1019-1020.
Festinger L. A Theory of Cognitive Dissonance. Palo Alto, CA: Stanford University Press, 1957.
Burke S, Schmidt G, Wagner S, Hoffman R, Hanlon N. Cognitive Dissonance in Social Work. J Public Child Welf 2017; 11: 299-317.
IDH Finance. Annual report for Bondholders Year ended 31 March 2018. Available at https://www.mydentist.co.uk/docs/default-source/Investors/idh-finance-annual-report-to-bondholders-31-march-18.pdf (accessed April 2019).
Holden A. Dentistry's social contract and the loss of professionalism. Aust Dent J 2017; 62: 79-83.
Hafferty F W, Castellani B. The increasing complexities of professionalism. Acad Med 2010; 85: 288-301.
Collins S. Statutory Social Workers: Stress, Job Satisfaction, Coping, Social Support and Individual Differences. Br J Soc Work 2008; 38: 1173-1193.
LDC Conference. Question time debate: getting prevention back into the dental contract. 2018.
Gruber M. Cognitive dissonance theory and motivation for change: a case study. Gastroenterol Nurs 2003; 26: 242-245.
Price L, Duffy K, McCallum J, Ness V. Are theoretical perspectives useful to explain nurses' tolerance of suboptimal care? J Nurs Manag 2015; 23: 940-944.
Department of Health and Social Care. NHS Constitution for England. 2012. Available at https://www.gov.uk/government/publications/the-nhs-constitution-for-england (accessed April 2019).
Bradley E H, Curry L A, Devers K J. Qualitative data analysis for health services research: developing taxonomy, themes, and theory. Health Serv Res 2007; 42: 1758-1772.
Yardley L. Dilemmas in qualitative health research. Psychol Health 2000; 15: 215-228.
Komatsu H, Yagasaki K, Yamauchi H. Fertility decision-making under certainty and uncertainty in cancer patients. Sex Reprod Healthc 2018; 15: 40-45.
Papakostopoulou M, Hurst D. Disseminating research evidence: what matters to general dental practitioners? Br Dent J 2018; 225: 413-417.
Abarca E, Campos S, Herskovic V, Fuentes C. Perceptions on technology for volunteer respite care for bedridden elders in Chile. Int J Qual Stud Health Well-being 2018; 13: 1422663.
Collin V, Toon M, O'Selmo E, Reynolds L, Whitehead P. A survey of stress, burnout and well-being in UK dentists. Br Dent J 2019; 226: 40-49.
Acknowledgements
EO would like to thank the BDA Trust Fund and the Shirley Glasstone Hughes Trust Fund for funding this project and those who participated.
Author information
Authors and Affiliations
Rights and permissions
About this article

Cite this article
O’Selmo, E., Collin, V. & Whitehead, P. Dental associates' perceptions of their working environment: a qualitative study. Br Dent J 226, 955–962 (2019). https://doi.org/10.1038/s41415-019-0258-y
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-019-0258-y
This article is cited by
-
Psychological distress and the perceived impact of the COVID-19 pandemic on UK dentists during a national lockdown
British Dental Journal (2021)
-
Supporting dentists' health and wellbeing - workforce assets under stress: a qualitative study in England
British Dental Journal (2021)
-
Commissioning in the community dental services: what do dentists think?
British Dental Journal (2020)
-
The community and public dental services: a mixed-method exploration of the workforce
British Dental Journal (2020)
