
Abstract
Flexible partial removable dental prostheses (PRDP) provide superior aesthetics, durability, improved patient comfort due to softer surface and low elastic modulus, and require less time and expense for fabrication. However, when a flexible PRDP is used to replace several missing teeth, especially when no occlusal rests or vertical stops are present, rotation and sinking of the denture base and resorption of the residual ridge tend to occur. This may result in the concentration of excessive force in the resin clasp, along with clasp deformation or fracture, and compression of the marginal gingiva. In such situations, it is advisable to incorporate a metal framework and occlusal rests in the design of the flexible PRDP to achieve the optimal rigidity and support. This article describes a case restored with such a 'combination' prosthesis.
Similar content being viewed by others


Key points
-
Helps the general dentist understand the indications of flexible partial dentures and combination dentures.
-
Describes the steps of fabrication of the combination prostheses.
-
Highlights how small details, such as addition of clasps for interocclusal records and a wax try-in appointment, are critical and help the practitioner perform the procedures accurately.
Introduction
Partial removable dental prostheses (PRDP), fabricated using thermoplastic resin, are commonly known as flexible dentures, non-clasp dentures, clasp-free dentures, and metal-free dentures.1,2,3 The prosthesis is retained using flexible retentive arms made from thermoplastic denture base resin which has greater elasticity compared to a conventional heat-polymerised denture base resin (PMMA).1
Flexible PRDPs are indicated in the following situations: few missing anterior teeth, few missing posterior teeth with occlusal support, desire for improved aesthetics, large oral defect, bilateral ridge undercuts, bony exostoses, large tuberosities, metal/monomer allergy, tilted teeth, microstomia and/or scleroderma.1,2,4 The resin clasps of flexible PRDPs cover the cervical regions of abutment teeth, the marginal gingiva, and the labial-buccal mucosa.1 Hence, it is critical to ensure that the resin correctly approximates the anatomy and that patients are able and motivated to maintain oral hygiene.1,5,6
Flexible PRDPs provide superior aesthetics,1 durability, improved patient comfort due to softer surface and low elastic modulus,7,8,9,10,11,12 and require less time and expense for fabrication.1 However, they discolour and degrade,13,14,15,16 are difficult to adjust and polish,17 and may increase the risk of exacerbating periodontal conditions due to the wide area of coverage of the resin clasp.1,5,6 When flexible partial dentures are used to replace several missing teeth, especially when no occlusal rests or vertical stops are present, rotation and sinking of the denture base and resorption of the residual ridge tend to occur.1 This may result in the concentration of excessive force in the resin clasp, along with clasp deformation or fracture.1 In addition, sinking of the dentures may result in compression of the marginal gingiva by the resin clasp.1 In such situations, it is advisable to incorporate a metal framework and occlusal rests in the design of the flexible PRDP to achieve the optimal rigidity and support. Such a PRDP may be indicated in almost all types of partially edentulous arches.1,18 This article describes a case restored with such a 'combination' prosthesis.
Case report
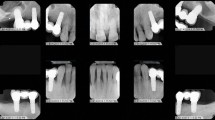
A 77-year-old Indian male reported to the author's clinic with the chief complaint of missing teeth and an inability to function with existing partial removable dental prostheses. The patient had lost his teeth (18, 17, 16, 15, 14, 24, 25, 26, 27, 28, 37, 38, 46, 47, 48) due to caries and periodontal disease (Figs 1, 2, 3). Flexible partial dentures were fabricated, two years previously, to replace the missing teeth but the patient was unable to function with them, owing to poor retention and stability. The existing teeth had mild periodontitis and teeth 23, 34 and 45 had carious lesions. The patient's oral hygiene was fair. The patient reported a history of cardiac disease and two bypass surgeries in the last three years. The patient did not want to undergo any invasive surgery and desired simple, retentive, functional and aesthetic restorations.

Panoramic radiograph of the patient

Maxillary arch with several missing teeth

Mandibular arch
Periodontal and restorative therapy were performed and the patient was given detailed instructions and cleaning aids to maintain his oral hygiene. Flexible partial dentures were fabricated by the previous dentist to prevent display of metal retainers when the patient smiled. However, the patient had several teeth missing in the maxillary arch and Kennedy class I space configurations, contraindicating the use of flexible partial dentures. To circumvent the problems associated with flexible partial dentures but retain their aesthetic advantage, a cast metal framework with flexible denture bases and direct retainers was planned for both the maxillary and the mandibular arch. A polyamide denture base resin (Sunflex) was proposed due to its inherent advantages including: stain resistance, superior aesthetics, ease of repair and reline procedures.19
Fabrication of the definitive restorations
Following improvement in periodontal health, the procedures for fabrication of the definitive prostheses were initiated. Most of the steps were similar to ones used for fabricating conventional cast partial dentures. The few differences included incorporation of a flexible resin direct retainer as opposed to cast metal direct retainers, use of flexible thermoplastic resin as opposed to acrylic resin for denture base fabrication, and creation of diatorics in the prosthetic teeth to aid in the retention of the prosthetic teeth to the denture base. The clinical and laboratory steps are outlined below:
-
1.
Diagnostic impressions were made with alginate (alginate impression material) and poured with type III dental stone (Microstone)
-
2.
Interocclusal records were made and the casts were mounted on a type III semi-adjustable articulator (WhipMix 2240)
-
3.
The casts were surveyed and flexible PRDPs with cast metal major connector, minor connector, indirect retainers and flexible direct retainers and denture bases were designed
-
4.
The mouth preparation was limited to preparation of rest seats for support and indirect retention
-
5.
Master impressions were made with alginate (alginate impression material) and poured immediately using a type III dental stone (Microstone). The definitive casts and the design casts were sent to the laboratory, along with detailed instructions for framework fabrication. The laboratory was instructed to initially incorporate metal clasps in the framework (for retention) to facilitate the framework try-in, interocclusal registrations and the wax trial denture try-in procedures
-
6.
The framework was tried in the mouth using a disclosing medium (disclosing wax) and adjusted as needed
-
7.
An altered cast impression was deemed unnecessary as the denture bearing mucosa was firm and healthy and it was accurately recorded on the master cast
-
8.
Wax rims were attached to the frameworks, interocculsal records were made and shade selection accomplished
-
9.
The definitive casts were mounted on a semi-adjustable articulator using the interocclusal records. Prosthetic teeth were selected based on the occlusal anatomy, the size of the existing natural teeth and shade determined. Diatorics were created in the prosthetic teeth (to aid in mechanical retention) and they were waxed to the framework
-
10.
The wax trial dentures were tried in the mouth to evaluate the aesthetics and occlusion. The clinically approved wax trial dentures with the definitive casts were sent to the laboratory for denture processing. The laboratory was instructed to eliminate the metal clasps and incorporate flexible thermoplastic resin clasps, as indicated in the PRDP design. Since deep alveolar undercuts were present cervical to all the abutment teeth, the laboratory was instructed to extend the resin clasp to the tooth adjacent to the abutment teeth, to provide the desired rigidity and strength to the clasps
-
11.
The combination partial denture was tried in using a disclosing medium (Disclosing wax) and adjusted accordingly. Following adjustments, the combination partial denture was finished, polished and placed in the patient's mouth.
Step 10 is shown in Figures 4, 5 and 6. Step 11 is shown in Figures 7 and 8.

Metal clasps eliminated and wax trial denture waxed to final contour

Maxillary definitive prosthesis

Mandibular definitive prosthesis

a) Maxillary prosthesis placed in the patient's oral cavity b) Mandibular prosthesis placed in the patient's oral cavity

Resin clasps do not hamper patient aesthetics and blend with the oral cavity
The patient was very pleased with the prostheses (Fig. 9). Detailed home care instructions were provided, and the patient was asked to return in a week for a recall appointment. In addition, the patient was informed that over a period of time, the partial denture may require refinements and adjustments including the replacement of worn acrylic teeth and relining procedures, due to changes in the denture bearing tissues. The patient was also recalled periodically for periodontal maintenance.

Patient's smile
The patient complained of soreness during the first two recall visits. He was asked to massage his tissues twice a day and keep the prostheses out of the mouth for six to seven hours each day, as mentioned in the home care instructions. The patient was comfortable with his prostheses on the following visit. He has been followed-up for the last two years and has been comfortable functioning with the prostheses.
Summary
Flexible PRDPs are contraindicated when multiple teeth are missing with no vertical stops.18 However, the combination partial denture is indicated in all such situations and provides the desired retention, stability and support, while improving patient aesthetics. The acrylic prosthetic teeth are mechanically bonded to the thermoplastic resin. Hence, there is a slight possibility that the prosthetic teeth may come out of the prosthesis, however, this was not observed in the case described in this article.
References
Fueki K, Ohkubo C, Yatabe M et al. Clinical application of removable partial dentures using thermoplastic resin-part I: definition and indication of non-metal clasp dentures. J Prosthodont Res 2014; 58: 3-10.
Lowe L G. Flexible denture flanges for patients exhibiting undercut tuberosities and reduced width of the buccal vestibule: a clinical report. J Prosthet Dent 2004; 92: 128-131.
Meijer G J, Wolgen P J. Provisional flexible denture to assist in undisturbed healing of the reconstructed maxilla.J Prosthet Dent 2007; 98: 327-328.
Samet N, Tau S, Findler M, Susarla S M, Findler M. Flexible, removable partial denture for a patient with systemic sclerosis (scleroderma) and microstomia: a clinical report and a three-year follow-up.Gen Dent 2007; 55: 548-551.
Zlatarić D K, Celebić A, Valentić-Peruzović M. The effect of removable partial dentures on periodontal health of abutment and non-abutment teeth.J Periodontol 2002; 73: 137-144.
Hosoi T. Non-clasp denture. DE 2009; 168: 1-4.
Sano M, lto K, Nomura A, Kohno S. [Properties of thermoplastic polymers used for non-clasp dentures.]J Jpn Soc Dent Products (Japanese)2009; 23: 28-34.
Yokoyama N, Machi H, Hayashi K, Uchida T, Ono T, Nokubi T. [Physical properties of polyamide resin (nylon group) as a polymeric material for dentures: Part 2. Surface hardness and tensile strength.] J Nippon Acad Dent Technol (Japanese) 2004; 25: 87-92.
Kawara M, Suzuki H, Ishikawa S. [Progress of EstheShot1 for esthetic denture - report of abrasion losses. Ann.]Jpn Prosthodont Soc (Japanese)2011; 3: E89.
Ucar Y, Akova T, Aysan I. Mechanical properties of polyamide versus different PMMA denture base materials. J Prosthodont 2012; 21: 173-176.
Hayashi K, Yokoyama N, Machi H, Uchida T, Ono T, Nokubi T. [Physical properties of polyamide resin (nylon group) as a polymeric material for dentures: Part 1. Characteristics of absorbent and dimensional change.]J Nippon Acad Dent Technol (Japanese)2004; 25: 80-86.
Hishimoto M, Katou Y, Akita Y, Murakami Y, Iida S. [Physical properties of polyester copolymer for denture materials.]J Nippon Acad Dent Technol (Japanese)2008; 29 (Spec Iss): 196.
Yatabe M. [How to deal with non-clasp denture? Its advantages and problems.]Quintessence (Japanese)2010; 29: 2083-2090.
Takabayashi Y. Characteristics of denture thermoplastic resins for non-metal clasp dentures. Dent Mater J 2010; 29: 353-361.
Katsumata Y, Hojo S, Ino S et al. [Colour stability of a flexible nylon denture base resin.] J Kanagawa Odont Soc (Japanese)2007; 42: 140-145.
Sepúlveda-Navarro W F, Arana-Correa B E, Borges C P, Jorge J H, Urban V M, Campanha N H. Colour stability of resins and nylon as denture base material in beverages.J Prosthodont 2011; 20: 632-638.
Abuzar M A, Bellur S, Duong Net al. Evaluating surface roughness of a polyamide denture base material in comparison with poly (methyl methacrylate). J Oral Sci 2010; 52: 577-581.
Ito M, Wee A G, Miyamoto T, Kawai Y. The combination of a nylon and traditional partial removable dental prosthesis for improved esthetics: a clinical report.J Prosthet Dent 2013; 109: 5-8.
Thumati P, Padmaja S, Raghavendra Reddy K. Flexible Dentures in Prosthodontics - An overview.Indian J Dent Adv 2013; 5: 1380-1385.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ahuja, S., Jain, V., Wicks, R. et al. Restoration of a partially edentulous patient with combination partial dentures. Br Dent J 226, 407–410 (2019). https://doi.org/10.1038/s41415-019-0095-z
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-019-0095-z
