
Richard Holliday interviews research dental nurse Kimberley Pickering and Fiona Ellwood about their contributions to dental research during the COVID-19 pandemic.

©Malte Mueller/Getty Images Plus
Introduction
2020 will be a memorable year for all of us. The COVID-19 pandemic has had huge impacts on our personal and social lives but as dental professionals we have also seen substantial changes to our working lives. Dental nurses in both NHS and private settings have contributed to the pandemic response in many ways including, but not limited to, being redeployed to other NHS services, working in Urgent Dental Care Centres, and getting dental practices reorganised and ready to restart non-urgent care. The importance of good quality dental research has been highlighted by the pandemic and this article interviews two dental nurses contributing to different parts of the research pathway during the pandemic.
Kimberley, what COVID-19 research have you been involved with?
As a dental care professional my involvement has been working in collaboration with a large research group at the School of Dental Sciences, Newcastle University, comprising of clinicians, academics and basic scientists eg microbiologists. As a collective, our overall aim is to improve understanding of dental aerosols and splatter to allow the safest practice of dentistry. At the start of the pandemic our work focused on updating old research methodologies (mainly used in the 1980s and 1990s) by adding in modern techniques and research methods. The methods used a tracer dye (fluorescein) and two techniques for measuring it. Next, we tested a range of procedures and checked the effect of suction and opening the windows. We looked at contamination close by and also over an open plan clinic such as here in the dental hospital. Figures 1 and 2 illustrate the experimental set up.

Kimberley working with an orthodontist to evaluate the potential contamination produced from an orthodontic debonding procedure

This image shows the dental mannequin after one of our pilot experiments. This highlights the local contamination when no mitigation procedures are used!
Kimberley, what have the main findings of your research been so far?
We found that:
-
'Water spray' from dental instruments can travel large distances and distribution of contamination (shown by fluorescein) varied widely across our experimental area (Fig. 3)
Fig. 3 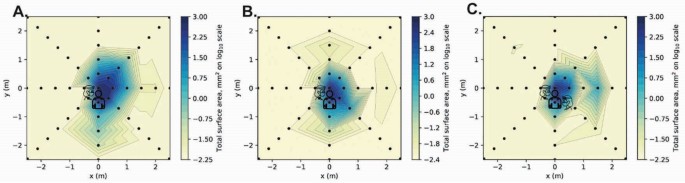
These series of heatmaps show contamination from using a high-speed drill to complete a crown preparation on an upper right central incisor. A was conducted without suctionB was completed with the operator holding their own suctionC was conducted with an assistant operating the dental suction. The darker blue areas represent the areas of higher contaminationthe light bluegreen represent areas of moderate contaminationthe yellow represents areas of no or little contamination. This image has been reproduced from Allison et al. 20201
-
Across all our experiments we found that the areas which received the most contamination ('hot spots') were down the length of the patient (toward the feet) and opposite the operator (the operator was right handed). This highlights the importance of good quality patient coverings (aprons) and PPE of the dental assistant
-
As a dental nurse it was reassuring to find that dental suction (with a wide aspirator tip) substantially reduces contamination. Also, the levels of contamination were much lower on the assistant compared to the operator - the highest sites were on my left arm and chest (I was holding the suction with this hand)
-
We were able to compare different procedures and found that using a high-speed drill or an ultrasonic scaler produced the most splatter and aerosol. Using a slow hand piece (without irrigation) during an orthodontic debonding procedure produced very low levels of contamination and was a low risk procedure for aerosol generation
-
We have also conducted a study in an open plan clinic, such as those you might find in a dental hospital. The findings of this study have helped establish safe working practices in these clinics, including data on fallow times.

The findings of our research have now been published in a series of papers.1,2,3
Kimberley, how did you find working on the project?
Firstly, I am very delighted to have been given the opportunity to work alongside the team. No matter what level of expertise you bring, I felt a massive involvement and my work contribution was valued. I enjoyed the entire journey of the study, from problem solving in the development phase, to learning new skills in the laboratory. You may think this is silly, but the most challenging part for me was my introduction to a pipette and trying not to drop the sample plate before it went into the plater reader for analysis. I particularly enjoyed the leadership role experience I gained in this project - I was in charge of running some of the experiments on the clinic once I had mastered the process.
You may think this is silly, but the most challenging part for me was my introduction to a pipette and trying not to drop the sample plate before it went into the plater reader for analysis.
Fiona, can you tell us more about the Scottish Dental Clinical Effectiveness Programme (SDCEP) AGP report you were involved with and what your role was?
Dental services have been seriously reduced during the pandemic and there has been an urgent need to look to the safe remobilisation against the backdrop of uncertainty and uniqueness of the virus. The implications and risk factors surrounding the use of aerosol generated procedures (AGPs) and the transmission of SARS-CoV-2 therefore became a priority of much needed research.
With this in mind, the SDCEP recently undertook a 'Rapid Review' of evidence relating to the generation and mitigation of aerosols in dental practice.4 The aims of the review were to:
-
Determine which dental procedures constitute AGPs
-
Determine measures likely to mitigate the risk of transmission of SARS-CoV-2 via dental AGPs
-
Inform procedures for environmental cleaning between patients following a dental AGP.
It was a privilege to be invited to contribute to this work as part of the working group. My role as part of the working group was to represent the views of a wider group; apply professional knowledge, experience and expertise; to consider summarised evidence and to contribute to considered judgement outcomes; and to provide feedback on any drafts of the review. This was a fast pace review with huge support from the methodology team and multiple virtual meetings.
Fiona, this is a large document (36 pages). Can you summarise the main findings, particularly those most relevant to the dental nurse?
Dental nurses are key members of the dental team and quite often are responsible for infection prevention and control and as such, are well placed to not only inform and implement new ways of working but to help in the training of others. Nevertheless, the pandemic has taken the profession into new territory and unique times and everyone has had to adapt and respond to the rapidly evolving and urgent situation that we have found ourselves in. Everything happened very quickly in March 2020 and urgent safety measures had to be implemented in order that patients and the team were kept safe. What the dental teams looked for was guidance - this after all is what has always happened - but this time it was different. Dental nurses were not unique in not knowing what to do at the time, but they were certainly at the forefront when it came to adapting to new ways of working and volunteering to work in emergency and medical settings. This review has given long awaited clarity to some of the more complex matters and allowed all members of the dental team including dental nurses to make sensible and safe judgement calls.
In summary this review has considered evidence relating to the generation of AGPs and the potential mitigation of aerosols, as well as the risk factors of the transmission of SARS-CoV-2. The considered judgements were based on the balance of benefits and harm, acceptability and feasibility. Its whole purpose was to inform policy makers and those developing clinical guidance for the dental team. Whilst this appears to be a rather large document, given the enormity of the task and the extent of the comprehensive literature considered, the industry is incredibly lucky that it is just 36 pages long. The research group were acutely aware that the dental industry was eagerly awaiting the publication of the Rapid Review and relying on it to an extent, to potentially play a part in the reduction in fallow times and therefore a change in the current level of services that they could offer.
The Review was undertaken as a response to the evolving pandemic and was compiled with contributors from the four nations and from a multidisciplinary working group; focus groups also played a part in this work. In short, the review determines what is meant by aerosol generating procedures (AGPs), it determines which procedures produce bioaerosols and the associated level of risks to the procedures. This then allowed for the categorisation of dental procedures into three groups and a broader picture formed of how air changes could be influential in determining 'down time'. Figure 4 is a flow chart presenting recommended fallow times in different conditions.

Determining fallow times for Group A dental procedures. Image taken with permission from SDCEP Mitigation of aerosol generating procedures in dentistry4
The review discusses the various mitigations ie 'Procedural and Environmental' and the recommendations are noted below.
Procedural mitigations
-
High volume suction - recommended for universal adoption
-
Rubber Dam - recommended for universal adoption
-
Pre-procedural mouth rinses - not recommended for universal adoption
-
Antimicrobial coolants - not recommended for universal adoption.
Environmental mitigations
-
Fallow time - recommended for universal adoption
-
Air cleaners - not recommended universal adoption.
These of course are conditional statements, and some practitioners may choose to use them after considering all of the factors. This is based on current available evidence and new evidence will continue to inform this work.
Fiona, how did you find the experience of working on this project?
It was an incredible privilege to be involved in this work; it has provided great insight into the mechanisms of conducting a Rapid Review at pace, but also in the unique situation of a pandemic. The whole group considered and listened to the points of view aired and it was fabulous to be able to work collaboratively with such esteemed members of the dental world and beyond, and then have a part to play ensuring colleagues understood the contents and the relevance and application to practice. Following the constant ream of papers and observing the appraisal and synthesis of relevant evidence and the analysis of the findings was incredible. The group used anonymous virtual polling to form consensus on the issues. Although we had regular weekly scheduled meetings there was a need, as we approached the deadline, to conduct additional evening meetings and every time we logged on, the minutes and updates were in front of us. We had presentations of ongoing and recently published research by research groups such as the team at Newcastle University, which Kimberley is a member of, which were really insightful. We knew that this review was going out on 25 September 2020 and that a first and potential second iteration would have to appear prior to this and whilst that added an element of pressure, it also helped to keep us on track. This brought a whole new dimension to my research experience and has certainly broadened my outlook on what is possible in emergency/urgent and evolving situations when applying and considering a methodology and methodological approach to research. I know it would not have been for everyone but I truly embraced the work in hand and look forward to the future workstreams.
I want to reassure any dental nurse/dental care professional who is interested in research that such a career pathway does exist and provides exciting challenges and opportunities.
Kimberley, there are not many research dental nurses around the country. Can you tell us a little bit about how you got into this role and your journey so far?
Well, I was born and brought up in Fiji. However, after finishing school I served in the British Army, achieving the rank of sergeant. After eight years of military service, I gained British citizenship and settled in England, retraining as a dental nurse and qualifying in 2012. I still currently serve in the Army Medical Services Reserves, 201 Field Hospital Unit, with the Royal Army Dental Corps. In 2013, after a year working in a dental practice, I progressed my career by joining the Dental Clinical Research Facility (Dental CRF) at the Newcastle upon Tyne Dental Hospital. The post was for a research dental nurse with my primary role being to support a wide range of NIHR portfolio research studies. I also have additional responsibilities as the nominated link person for the Oral and Dental Patient, Carer and Public Involvement (PCPI) group, and have recently been promoted to senior research dental nurse. I have assisted with over 20 different research studies (quantitative/qualitative) and am joint co-author on several research project publications (British Medical Journal, Journal of Dentistry).In 2016 I decided to consolidate my professional research experiences with academic study to develop further my knowledge of research methods, research approvals, and ethics and governance when conducting research trials and interpreting data. To achieve this, I enrolled in an MSc clinical research programme, part-time, completing with Merit in 2019. My MSc project was funded via a Dental Care Professional research award (October 2018) and this has recently been published in BDJ Open (my first lead author paper!).5
And so here I am today, a dental nurse, with the current research involvement in light of the issues surrounding COVID-19 pandemic and the implications it has on dentistry. Throughout my journey I have been warmly supported and encouraged by my colleagues to expand my involvement in the research programme. I urge others who wish to learn new skills and tackle new and interesting problems to think about a career in research. Research qualifications and extended duties are not normally presented, or in some cases structured, as an alternative career route for dental nurses. However, I want to reassure any dental nurse/dental care professional who is interested in research that such a career pathway does exist and provides exciting challenges and opportunities.
Editor's note
A special issue of BDJ Team focused on DCP research will be published later on in 2021. To propose or submit an article or for more information, please contact the Editor on k.quinlan@nature.com.
References
Allison J R, Currie C, Edwards D C et al. Evaluating aerosol and splatter following dental procedures: addressing new challenges for oral healthcare and rehabilitation. J Oral Rehabil 2020; doi:10.1111/joor.13098.
Holliday R, Allison J R, Currie C et al. Evaluating dental aerosol and splatter in an open plan clinic environment: implications for the Covid-19 pandemic. J Dent 2021; doi: 10.1016/j.jdent.2020.103565.
Llandro H, Allison J R, Currie C et al. Evaluating aerosol and splatter during orthodontic debonding: implications for the COVID-19 pandemic. Br Dent J 2021; doi: 10.1038/s41415-020-2503-9.
Scottish Dental Clinical Effectiveness Programme. Mitigation of aerosol generating procedures in dentistry. A rapid review. 25 September 2020. Available at: https://www.sdcep.org.uk/published-guidance/covid-19-practice-recovery/rapid-review-of-agps/ (accessed December 2020).
Pickering K, Bissett S M, Holliday R, Vernazza C, Preshaw P M. Exploring the use of mouth guards in Muay Thai: a questionnaire survey. BDJ Open 2020; 6: 20.
Author information
Authors and Affiliations
Rights and permissions
About this article

Cite this article
Holliday, R., Pickering, K. & Ellwood, F. COVID-19 and dental nursing. BDJ Team 8, 10–13 (2021). https://doi.org/10.1038/s41407-021-0497-z
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41407-021-0497-z
This article is cited by
-
The role of the dental team during the COVID-19 pandemic
BDJ Team (2022)
