
Abstract
Cancer-related fatigue is an extremely common and debilitating psychiatric symptom that affects up to 80% of cancer patients. Despite its negative impact on the patient’s quality of life, there is no well-established biomarker or mechanisms associated with this debilitating condition. The functional brain-derived neurotrophic factor (BDNF) Val66Met single nucleotide polymorphism (SNP) has been associated with a variety of psychiatric illnesses. We hypothesized that Val66Met may influence the risk for developing cancer-related fatigue. BDNF Val66Met was analyzed by polymerase chain reaction in 180 patients with confirmed cancer diagnoses. Fatigue was measured using the Functional Assessment of Cancer Therapy-Fatigue (FACIT-Fatigue) questionnaire. Depression was measured using the Hamilton Depression Scale (HAM-D). Data were transformed when necessary and regression models were constructed to access the association between genotype and symptom severity. Participants carrying the Met allele reported significantly less fatigue compared to the Val/Val genotype group. The presence of the Met allele did not influence depression levels. The results suggest that the BDNF Val66Met polymorphism confers protective advantage against cancer-related fatigue; whereas having the Val/Val genotype may be a genetic risk factor. Findings from this study not only provide clues to the neural basis of cancer-related fatigue, but also allow for symptom severity prediction and patient education with the goal to improve symptom management.
Similar content being viewed by others
Introduction
Oncology patients often experience psychiatric symptoms such as cancer-related fatigue, which differs from the normal sense of “tiredness” as it cannot be resolved by rest and severely impacts their daily functioning1. Of all cancer-related symptoms, fatigue is often the most distressing and prevalent symptom reported by up to 80% of oncology patients1,2. Currently, the diagnosis of cancer-related fatigue relies entirely on self-reports with no well-established biomarkers3. In addition, little is known about its underlying mechanisms and no FDA-approved therapeutic interventions are available1. As a result, the National Cancer Institute has identified cancer-related fatigue as a first-tier, high-priority research area4,5.
The unrelenting sense of tiredness can be both persistent and severe, directly affecting the patient’s ability to perform daily tasks, resulting in helplessness and despair6. While there is a scarcity of empirical evidence for effective management strategies, recognition of the symptom by healthcare providers and patient education may alleviate the emotional burden associated with cancer-related fatigue6. While cancer-related fatigue is often reported by patients as a multidimensional symptom, the overall sense of tiredness notably exhibits a cognitive component7,8. Interestingly, not all patients with cancer or those receiving cancer treatments experience profound fatigue, and it is conceivable that genetic vulnerabilities may alter the threshold of symptom presentation in response to inflammation induced by cancer or its treatments9.
Brain-derived neurotrophic factor (BDNF) is a key neurotrophin expressed ubiquitously throughout the brain and plays a central role in almost all facets of brain function such as neuroplasticity, developmental processes, synaptogenesis, and maintenance of functional neuronal networks10. BDNF is produced in the neuronal cell body and transported in secretory vesicles into somatodendritic compartments where they are released upon electric stimulation11. BDNF is first synthesized as the precursor proBDNF (~32 kDa) and cleaved into mature BDNF (~13 kDa)12. Pro-BDNF and mature BDNF (mBDNF) are thought to have opposing effects mediated by specific neurotrophin/receptor interactions: (1) mBDNF dimerizes and binds to tropomyosin-related kinase B (TrkB) receptor and promotes long-term potentiation, neurite outgrowth, and cell survival; (2) proBDNF, on the other hand, promotes long-term depression, growth cone retraction, and neuronal cell death by interacting with pan-neurotrophin receptor 75 (p75NTR) and a co-receptor, sortilin13.
A particular single nucleotide polymorphism (SNP) that has garnered increasing interest is the BDNF Val66Met (rs6265), a single nucleotide substitution (G196A) causing an amino acid change at codon 66 from the canonical valine (Val) to methionine (Met) in the pro-region of the BDNF11. The Met66 allele occurs in 50% of Asians, 30% of Caucasians, and 5% of African Americans14. Functionally, Val66Met has been shown to reduce activity-dependent release, but not constitutive release, of BDNF11. Even though the Val→Met substitution at codon 66 does not alter the structural or functional properties of mBDNF, Val66Met markedly reduces the association of BDNF with secretory vesicle markers, suggesting that the decrease in activity-dependent release is a result of altered secretion instead of production11. The consequences of having the Met allele (Val/Met, Met/Met) have been associated with a plethora of detrimental effects including decreased hippocampal volume, memory deficits, increased anxiety behavior, and increased risk for depression both in animal models and human studies15,16,17. However, the high natural occurrence of Val66Met suggests that the Met allele may confer selective advantage. In fact, the Met allele appears to be protective in older adults: compared to Val/Val individuals, Met allele carriers have demonstrated higher cortical thickness, better episodic memory performance, slower cognitive decline, and decreased risk for Alzheimer’s disease in old age, but not early in adult life18,19. In addition, the effect of Val66Met differs based on gender and alters the risk for depression in a gender-specific manner20. Val66Met also influences disease outcome in a time-dependent fashion: for example, Met allele carriers exhibited greater acute deficits, but enhanced recovery, after ischemic stroke21.
Previous studies on the role of BDNF in cancer-related fatigue relied on measuring BDNF concentrations in plasma or serum as a proxy22. However, circulating BDNF is largely attributable to platelet precursor cells, megakaryocytes, which synthesize BDNF under the platelet BDNF promoter23. It is not clear whether circulating BDNF measured in blood reflects brain BDNF levels24. Despite the importance of BDNF on brain functions and increasing interest in Val66Met on psychiatric/cognitive symptoms, studies on the effects of Val66Met on cancer-related fatigue are non-existent. One study found a higher rate of suicide in cancer patients carrying the Met allele25. Interestingly, several recent studies provided new evidence to suggest a protective role of Val66Met against chemotherapy-induced cognitive impairment and depression26,27,28. In addition, Val66Met is a particularly interesting candidate SNP to examine for cancer-related fatigue due to the well-established symptomatic and possible mechanistic overlap between fatigue and depression29, and for the profound influence Val66Met has on the risk of depression in otherwise healthy individuals17.
The goal of this study was to determine the role of the BDNF Val66Met genotype on cancer-related fatigue in subjects with confirmed cancer diagnoses. As Val66Met has been shown to increase the risk for depression in healthy individuals29, we also examined whether this SNP influences depression in cancer patients. Here we report that Val66Met confers protective advantage against developing cancer-related fatigue. However, in contrast with healthy individuals, the risk for the development of depression is not altered by Val66Met in subjects with cancer.
Materials and methods
Participants
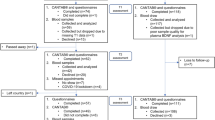
Data were collected from two studies: (1) patients with non-metastatic prostate adenocarcinoma scheduled to receive radiotherapy (NCT00852111); (2) patients with any type of cancer scheduled to receive any type of treatment (NCT01231932). Signed written informed consents were obtained prior to study participation.
NCT00852111 was approved in 2008 by the Institutional Review Board (IRB) of the National Institutes of Health (NIH). All subjects were 18 years of age or older, with confirmed cancer diagnoses, and scheduled to start cancer treatment at the NIH. Prospective participants were excluded if they had an unstable or end-stage disease of any body system, uncorrected hypothyroidism, untreated anemia, any medical history of tuberculosis, any infectious disease such as HIV or hepatitis, a chronic inflammatory disease, or a psychiatric disorder diagnosis within the past 5 years, or a second malignancy. Those receiving chemotherapy or taking medications known to affect cytokine production, such as tranquilizers, steroids, and nonsteroidal anti-inflammatory agents, were also excluded from this study.
Instruments
Fatigue was measured using the Functional Assessment of Chronic Illness Therapy-fatigue (FACIT-Fatigue) scale. The total fatigue scores range from 0–52; lower scores indicate higher fatigue intensity. Subjects with a FACIT-Fatigue score <43 were considered fatigued30,31. A 3-point difference in FACIT-Fatigue scores is considered to be a minimally clinically important difference32,33,34. Depression was measured using the Hamilton Depression Rating Scale (HAM-D). High scores indicate more severe depression: a score of 0–7 indicates no depression, a score of 8–16 indicates mild depression, and a score of ≥17 indicates moderate-to-severe depression35. See supplementary methods for more details.
BDNF rs6265 profiling
Whole blood samples were collected in ethylene-diamine-tetra-acetic acid tubes (BD Biosciences, Franklin Lakes, NJ, USA) and extracted using PureLink™ Pro 96 Genomic DNA Purification Kit (Invitrogen, Carlsbad, CA, USA). The region containing the BDNF Val66Met SNP (GenBank dbSNP: rs6265) was profiled using polymerase chain reaction (PCR) using the following primers: forward 5′–AGAAGAGGAGGCTCCAAAGG–3′ and reverse 5′–ACAAGGTGGCTTGGCCTAC–3′. After enzymatic purification, sequencing was performed by using BigDye™ Terminator Cycle Sequencing Kit (ThermoFisher Scientific, Waltham, MA, USA). Data analysis was performed using the DNASTAR Lasergene12® software (DNASTAR, Inc, Madison, WI, USA). The threshold for SNP detection was set to 10%. Mutations from the reference sequence were called when possible sequence quality and coverage allowed.
Statistics
Demographic and clinical characteristics were summarized by standard descriptive statistics. Values are expressed as Mean ± Standard Deviation (SD). For comparisons of clinical characteristics between groups, Student’s two-sample t test, Dunnett’s test, and the Wilcoxon Rank Sum test were used when appropriate and a chi-squared test was employed to examine differences in proportions. Using power analysis with an alpha of 0.05 and power of 80%, the projected sample size needed is ~41 subjects per group and a total of 82 subjects.
The first measurement of interest was the FACIT-Fatigue score and the chief predictor was genotype. The FACIT-Fatigue score was bounded at the upper limit by a maximum score of 52, inducing an asymmetrical distribution pattern that is left-skewed. To accommodate this feature, each score was divided by the maximum score, and then transformed with a logistic transformation36. The resultant transformed data had reduced skewness, affording the use of traditional statistical methods. The transformed FACIT-Fatigue score was first modeled as a function of genotype, and then modeled as a function of genotype, patient age, and a corresponding interaction (joint) effect of both within a generalized linear model assuming a normal distribution for the transformed outcome and an identity link.
As a larger proportion of total HAM-D scores equaled to zero (no depression) than would be predicted by standard probability models, the fit of zero-inflated models was explored. The total score could be viewed as a count; thus, zero-inflated Poisson37 and zero-inflated negative binomial38 models were employed to compare the scores between the two genotypes. A bootstrapped 95% confidence interval was estimated for the difference in the scores between the two genotypes. Model assessment was performed by comparing the outcome value frequencies against their corresponding observed frequencies. If the observed fit was similar between the zero-inflated Poisson and the negative binomial models, the probability model with the fewest parameters was selected. As was the case with the FACIT-Fatigue score, a second model was fit with terms for genotype, age, and their joint (interaction) effect.
Mean HAM-D and FACIT-Fatigue scores for those patients with T stage T1 were compared with all other stages by Dunnett’s test. The application of Dunnett’s test afforded protection against an inflation of the experiment-wise error rate for these two families of comparisons. All statistical tests were two-sided and conducted at the 0.05 level of statistical significance. Statistical analyses were performed using JMP 15.0.0 (SAS Institute, Cary, NC, USA) and SAS Version 9.4 (TS1M6, SAS Institute).
Results
Clinical characteristics
A total of 180 cancer patients were recruited for the study. To eliminate the potential confound introduced by the interaction between Val66Met and gender, we only included male subjects in the current study. The sample cohort were older men with a mean age of 65.3 ± 8.1 years (Table 1). Participants were predominantly Caucasian (73.3%). Prostate adenocarcinoma accounted for 95.5% of the cancer types (Table 1). Cancer T stages ranged from T1 to T4 (Table 1). Subjects with T0 or Tx at the time of the study were only included in the study if additional confirmatory cancer diagnostic evidence was obtained.
The BDNF Val66Met SNP genotype frequencies of the entire cohort were in Hardy–Weinberg Equilibrium (χ2 = 0.45, p = 0.504). The common homozygous Val/Val accounted for 66.11% of the total sample. Val/Met heterozygous and Met/Met homozygous represented 29.44% and 4.44% of the total sample, respectively (Table 2).
Val66Met alters risk for fatigue but not depression in cancer patients
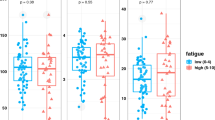
Met carriers (Met/Met and Val/Met) reported significantly higher FACIT-Fatigue scores indicating lower fatigue levels (47.1 ± 4.9) compared to Val/Val homozygous (43.4 ± 8.7) (Fig. 1a; F1178 = 9.70, p = 0.002). On the other hand, HAM-D scores were not significantly different between genotypes (Fig. 1b; Met carrier: 1.492 ± 2.171 vs. Val/Val: 1.508 ± 2.087; F1177 = 0.00, p = 0.961).

a Scatter plot of FACIT-Fatigue scores grouped by genotype. FACIT-Fatigue scores of subjects that carried the Met allele (47.089 ± 4.944) compared to subjects with Val/Val (43.357 ± 8.654) were significantly higher (F1178 = 9.70, p = 0.002). b Scatter plot of HAM-D scores grouped by genotype. There was no difference (F1177 = 0.00, p = 0.961) between subjects that carried the Met allele (1.508 ± 2.087) compared to subjects with Val/Val (1.492 ± 2.171). c Confidence Interval (CI) plot demonstrating that the difference between genotypes (Met carrier vs. Val/Val) was only significant in FACIT-Fatigue scores (p = 0.026) but not in HAM-D scores (p = 0.965). d The percentage of fatigued subjects (FACIT-Fatigue score <43), in the Val/Val group was significantly higher (33.61%) than the Met carrier group (18.03%) (p = 0.008, Wilcoxon Rank-Sums test). The rate of depression (HAM-D score ≥8) was not significant between the two genotypes (1.64 vs. 2.54%; p = 0.882).
A regression model was constructed to analyze FACIT-Fatigue scores as a function of genotype, and the adequacy of the fit of the model was shown in supplementary Fig. 1. The distribution of the model’s studentized deviance residuals were symmetrical and could be approximated by a standard Gaussian curve; thus allowing for the construction of a generalized linear model assuming a normal distribution for the transformed outcome (supplementary Fig. 1A). The symmetry and homoscedasticity of the model were further demonstrated by the agreement between the percentiles of a standard Gaussian distribution and the cumulative distribution of the Studentized deviance residuals (supplementary Fig. 1B). Carrying the Met allele significantly predicted lowered risk for fatigue at a 95% confidence interval (Table 3; 95% CI [0.0769, 1.2117], p = 0.026).
As most of the study participants were not depressed, a larger proportion of “0” HAM-D scores were reported than would be predicted by standard probability models. Zero-inflated Poisson and zero-inflated negative binomial models were thus constructed to compare the difference between genotypes in HAM-D scores (Supplementary fig. 2). The model predicted “0” values almost perfectly and positive values by <8% points of deviation (Supplementary Fig. 2A). The deviations of zero-inflated Poisson predicted values from observed HAM-D values by only 0.5–8% points indicating a sound fit of the model (Supplementary Fig. 2B). Carrying the Met allele did not predict the risk for depression (Table 4; 95% CI [−0.2726, 0.2852], p = 0.965).
The difference between Met carriers and Val/Val subjects in FACIT-Fatigue scores was statistically significant (Fig. 1c; 95% CI [1.37, 6.10], p = 0.026). In contrast, the corresponding 95% CI for the difference in mean HAM-D scores between the two cohorts [−0.84, 0.74] was not statistically significant (p = 0.965). We observed a significantly higher percentage of fatigued subjects (FACIT-Fatigue score <43) in the Val/Val group (33.6%), whereas only 18.0% of Met carriers were fatigued (p = 0.008). The rate of depression was low in both groups (Val/Val: 1.64% vs. Met carrier: 2.54%) and the difference between genotypes was not significant (Fig. 1d; p = 0.882).
Regardless of the cancer type, participants carrying the Met allele generally fell within the top quartile of the FACIT-Fatigue distribution, whereas participants with two copies of Val fell within the bottom quartile (Supplementary Fig. 3). Dunnett’s test was conducted to compare FACIT-Fatigue and HAM-D scores among T stages; no significant difference was detected at a 0.05 nominal level of statistical significance (Supplementary Fig. 4).
Participants carrying the Met allele exhibited lower body mass index (BMI) compared to the Val/Val group (Supplementary Fig. 5A; F1153 = 6.02, p = 0.016). BMI weakly correlated with actigraphy daily activity count (adjusted R2 = 0.05, p = 0.006). However, we did not observe any difference in daily activity count between genotypes (F1156 = 0.01, p = 0.910). Furthermore, daily activity count in the current study did not correlate with FACIT-Fatigue scores (Supplementary Fig. 5A; adjusted R2 = 0.0002, p = 0.311).
Discussion
Multiple lines of evidence suggest that cancer-related fatigue may be a result of unresolved inflammation stemming from a combination of genetic risk factors and inflammatory triggers including cancer9,39. Even though cancer-related fatigue represents a general sense of tiredness, emerging evidence points toward a cognitive component that involves a potential alteration in brain connectivity8,40. The Val66Met polymorphism within the pro-domain of BDNF has been associated with a variety of psychiatric disorders including depression, a symptom that is often co-morbid with cancer-related fatigue17,29. To our knowledge, this is the first study to demonstrate a novel genetic association between BDNF Val66Met polymorphism and lowered risk for developing cancer-related fatigue. Interestingly, although Val66Met has been shown to greatly increase the risk for depression in healthy individuals29, carrying the Met allele did not affect depression levels in patients with cancer. These findings are clinically significant as Val66Met may serve as a novel genetic marker that specifically predicts the risk for cancer-related fatigue, but not the often-comorbid depressive symptoms. In addition, our study offers a first glimpse into the neural basis of cancer-related fatigue and provides clues to developing future therapeutic interventions.
A growing body of literature suggests a causal role of peripheral inflammation in cancer-related fatigue pathogenesis as a result of either cancer or cancer treatment9,39. Although the exact mechanisms whereby peripheral inflammation results in fatigue symptoms is unknown; immune-chemosensory signaling via the afferent vagus nerve is thought to transduce peripheral inflammation signals to the central nervous system41. In fact, vagus nerve transection in an animal model of inflammation attenuated sickness behavior, which includes fatigue42. Interestingly, healthy adults with the Met/Met genotype exhibit reduced vagal activity as well as reduced cortisol response to acute stress43,44. It is possible that the Met allele confers advantage by dampening the hyperactivation of the vagus nerve immune sensory signaling pathway and decreases the risk for the consequent cancer-related fatigue.
Another possible explanation for the protective advantage of the Met allele may be related to the upregulation of proBDNF under pathological conditions45 combined with downregulated TrkB transcription and unchanged p75NTR in old age46,47. This suggests a shift in balance between the two forms of BDNF toward a more proapoptotic effect mediated by proBDNF, which may be particularly detrimental to patients with advanced age like those in the current patient cohort. Since the Val66Met genotype is associated with reduced activity-dependent secretion of both pro- and mature BDNF, it is conceivable that carrying the Met allele affords protection against cancer-related fatigue by reducing the proapoptotic effects of proBDNF48. It is worth noting that the protective advantage of Val66Met is likely to be genetic rather than a result of altered physical activity, as we did not observe any difference in daily activity between genotypes (Supplementary Fig. 5).
This study has several limitations. First, our study included subjects with multiple types of cancer with various levels of severity. Our decision not to exclude cancer types with small sample sizes was because patients will likely seek care because of the negative impact of fatigue on daily living regardless of the type of cancer. Interestingly, neither the cancer type nor the disease severity altered our findings. It is conceivable that Val66Met could be used as a general predictor for lowered risk of cancer-related fatigue, regardless of the cancer type or severity. We are actively recruiting patients with various types of cancer to test this hypothesis. Secondly, previous studies have shown that cancer and cancer treatment may lead to fatigue via different mechanisms39,49,50. We only included participants that had confirmed cancer diagnoses before the start of treatment in order to focus on fatigue related to cancer itself instead of cancer treatment. Future work will explore the effect of Val66Met on longitudinal changes in fatigue symptoms before and after cancer treatment. Thirdly, all participants included in this study were male to avoid the confound of gender-specific effects of BDNF51. Current efforts are being made to recruit female participants to further examine whether this polymorphism affects cancer-related fatigue and depression differently in different genders. In addition, future studies with a larger sample size will explore whether sex hormones influence the effect of Val66Met on fatigue. It is worth noting that BMI, which has been shown to increase the risk for psychiatric conditions such as depression and anxiety52, did not significantly correlate with fatigue or depression levels in our study. It is possible that there exists a ceiling effect where neuroinflammation related to cancer is already at a level whereby any additional contribution by BMI was not detected. Future studies that include non-cancer patients will help elucidate this point. Finally, the rationale for grouping Met heterozygous and homozygous individuals as Met carriers was based on in vitro evidence demonstrating the similarity in secreted BDNF between these genotypes53. While the sample size in the current study did not allow for comparisons among Val/Val, Val/Met, and Met/Met, future studies will investigate whether differences in protection against fatigue exist between Met heterozygous and homozygous individuals.
Clinical application of Val66Met SNP as a prognostic/predictive marker for assessing the risk of developing cancer-related fatigue has several advantages: (1) SNP detection can be easily performed requiring only a small sample of blood; (2) genotypic marker detection is affordable, reliable, and yields reproducible results; (3) using the functional Val66Met polymorphism provides a more accurate assessment for brain BDNF and bypasses the aforementioned disadvantage of measuring serum/plasma BDNF concentrations, which is largely attributable to platelet-derived BDNF. Furthermore, the knowledge of a patient’s Val66Met genotype could thus result in a more precise treatment recommendation for that patient, given his or her disease circumstances. For example, lower levels of daytime activity has been associated with worse cancer-related symptoms including depression and fatigue54. Exercise is often recommended for patients suffering from cancer-related fatigue, and exercise has been shown to increase both proBDNF and mBDNF55,56,57. It is conceivable that exercise should be prescribed to fatigued patients differently based on the Val66Met genotype, particularly if abnormalities in proBDNF production or signaling may play a role in the pathogenic process of the symptom.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Berger, A. M. et al. Cancer-related fatigue, version 2.2015. J. Natl Compr. Cancer Netw. 13, 1012–1039 (2015).
Cleeland, C. S. et al. The symptom burden of cancer: evidence for a core set of cancer-related and treatment-related symptoms from the Eastern Cooperative Oncology Group Symptom Outcomes and Practice Patterns study. Cancer 119, 4333–4340 (2013).
Campos, M. P. O., Hassan, B. J., Riechelmann, R. & Del Giglio, A. Cancer-related fatigue: a practical review. Ann. Oncol. 22, 1273–1279 (2011).
Panel NIoHS-o-t-S. National institutes of health state-of-the-science conference statement: symptom management in cancer: pain, depression, and fatigue, July 15–17, 2002. JNCI Monogr. 2004, 9–16 (2004).
Symptom management and quality of life steering committee. National Cancer Institute. 2015 strategic priorities: symptom management and quality of life steering committee. (2015). https://www.cancer.gov/about-nci/organization/ccct/steering-committees/2015-SxQoLSCStrategicPriorities.
Kirshbaum, M. Cancer-related fatigue: a review of nursing interventions. Br. J. Community Nurs. 15, 214–216 (2010). 218-219.
Feng, L. R., Espina, A. & Saligan, L. N. Association of fatigue intensification with cognitive impairment during radiation therapy for prostate cancer. Oncology 94, 363–372 (2018).
Feng, L. R. et al. Cognitive and motor aspects of cancer-related fatigue. Cancer Med. 8, 5840–5849 (2019).
Feng, L. R. et al. mGluR5 mediates post-radiotherapy fatigue development in cancer patients. Transl. Psychiatry 8, 110 (2018).
Kowiański, P. et al. BDNF: a key factor with multipotent impact on brain signaling and synaptic plasticity. Cell. Mol. Neurobiol. 38, 579–593 (2018).
Egan, M. F. et al. The BDNF val66met polymorphism affects activity-dependent secretion of BDNF and human memory and hippocampal function. Cell 112, 257–269 (2003).
Lu, B., Pang, P. T. & Woo, N. H. The yin and yang of neurotrophin action. Nat. Rev. Neurosci. 6, 603–614 (2005).
Sandhya, V. K. et al. A network map of BDNF/TRKB and BDNF/p75NTR signaling system. J. Cell Commun. Signal 7, 301–307 (2013).
Petryshen, T. L. et al. Population genetic study of the brain-derived neurotrophic factor (BDNF) gene. Mol. Psychiatry 15, 810–815 (2010).
Notaras, M., Hill, R. & van den Buuse, M. The BDNF gene Val66Met polymorphism as a modifier of psychiatric disorder susceptibility: progress and controversy. Mol. Psychiatry 20, 916–930 (2015).
Chen, Z.-Y. et al. Genetic variant BDNF (Val66Met) polymorphism alters anxiety-related behavior. Science 314, 140–143 (2006).
Youssef, M. M. et al. Association of BDNF Val66Met polymorphism and brain BDNF levels with major depression and suicide. Int. J. Neuropsychopharmacol. 21, 528–538 (2018).
Voineskos, A. N. et al. The brain-derived neurotrophic factor Val66Met polymorphism and prediction of neural risk for alzheimer disease. Arch. Gen. Psychiatry 68, 198–206 (2011).
Kailainathan, S. et al. Activation of a synapse weakening pathway by human Val66 but not Met66 pro-brain-derived neurotrophic factor (proBDNF). Pharmacol. Res. 104, 97–107 (2016).
Verhagen, M. et al. Meta-analysis of the BDNF Val66Met polymorphism in major depressive disorder: effects of gender and ethnicity. Mol. Psychiatry 15, 260–271 (2010).
Qin, L. et al. An adaptive role for BDNF Val66Met polymorphism in motor recovery in chronic stroke. J. Neurosci. 34, 2493–2502 (2014).
Wolff, B. S., Renner, M. A., Springer, D. A. & Saligan, L. N. A mouse model of fatigue induced by peripheral irradiation. J. Vis. Exp. 121, 55145 (2017).
Chacón-Fernández, P. et al. Brain-derived neurotrophic factor in megakaryocytes. J. Biol. Chem. 291, 9872–9881 (2016).
Gejl, A. K. et al. Associations between serum and plasma brain-derived neurotrophic factor and influence of storage time and centrifugation strategy. Sci. Rep. 9, 9655 (2019).
Park, S. et al. Associations between the brain-derived neurotrophic factor Val66Met polymorphisms and suicide in patients with cancer. Psychiatr. Genet. 28, 71–72 (2018).
Tan, C. J. et al. Replication and meta-analysis of the association between BDNF Val66Met polymorphism and cognitive impairment in patients receiving chemotherapy. Mol. Neurobiol. 56, 4741–4750 (2019).
Ng, T. et al. Brain-derived neurotrophic factor genetic polymorphism (rs6265) is protective against chemotherapy-associated cognitive impairment in patients with early-stage breast cancer. Neuro-Oncol. 18, 244–251 (2015).
Azoulay, D., Giryes, S., Nasser, R., Sharon, R. & Horowitz, N. A. Prediction of chemotherapy-induced peripheral neuropathy in patients with lymphoma and myeloma: the roles of brain-derived neurotropic factor protein levels and a gene polymorphism. J. Clin. Neurol. 15, 511–516 (2019).
Brown, L. F. & Kroenke, K. Cancer-related fatigue and its associations with depression and anxiety: a systematic review. Psychosomatics 50, 440–447 (2009).
Spichiger, E. et al. Prevalence and contributors to fatigue in individuals hospitalized with advanced cancer: a prospective, observational study. Int. J. Nurs. Stud. 49, 1146–1154 (2012).
Cella, D., Lai J-s, Chang, C.-H., Peterman, A. & Slavin, M. Fatigue in cancer patients compared with fatigue in the general United States population. Cancer 94, 528–538 (2002).
Yost, K. J., Eton, D. T., Garcia, S. F. & Cella, D. Minimally important differences were estimated for six Patient-Reported Outcomes Measurement Information System-Cancer scales in advanced-stage cancer patients. J. Clin. Epidemiol. 64, 507–516 (2011).
Cella, D. et al. Validation of the functional assessment of chronic illness therapy fatigue scale relative to other instrumentation in patients with rheumatoid arthritis. J. Rheumatol. 32, 811–819 (2005).
Jaeschke, R., Singer, J. & Guyatt, G. H. Measurement of health status: ascertaining the minimal clinically important difference. Controlled Clin. Trials 10, 407–415 (1989).
Zimmerman, M., Martinez, J. H., Young, D., Chelminski, I. & Dalrymple, K. Severity classification on the Hamilton depression rating scale. J. Affect. Disord. 150, 384–388 (2013).
Lesaffre, E., Rizopoulos, D. & Tsonaka, R. The logistic transform for bounded outcome scores. Biostatistics 8, 72–85 (2006).
Wagh, Y. S. & Kamalja, K. K. Zero-inflated models and estimation in zero-inflated Poisson distribution. Commun. Stat. - Simul. Comput. 47, 2248–2265 (2018).
Lindén, A. & Mäntyniemi, S. Using the negative binomial distribution to model overdispersion in ecological count data. Ecology 92, 1414–1421 (2011).
Feng, L. R., Suy, S., Collins, S. P. & Saligan, L. N. The role of TRAIL in fatigue induced by repeated stress from radiotherapy. J. Psychiatr. Res. 91, 130–138 (2017).
Hampson, J. P., Zick, S. M., Khabir, T., Wright, B. D. & Harris, R. E. Altered resting brain connectivity in persistent cancer related fatigue. NeuroImage: Clin. 8, 305–313 (2015).
Pavlov, V. A. & Tracey, K. J. The vagus nerve and the inflammatory reflex—linking immunity and metabolism. Nat. Rev. Endocrinol. 8, 743–754 (2012).
Goehler, L. E. et al. Vagal immune-to-brain communication: a visceral chemosensory pathway. Autonomic Neurosci. 85, 49–59 (2000).
Yang, A. C. et al. BDNF Val66Met polymorphism alters sympathovagal balance in healthy subjects. Am. J. Med. Genet. Part B: Neuropsychiatr. Genet. 153B, 1024–1030 (2010).
Alexander, N. et al. The BDNF Val66Met polymorphism affects HPA-axis reactivity to acute stress. Psychoneuroendocrinology 35, 949–953 (2010).
Krueger, F. et al. The role of the Met66 brain-derived neurotrophic factor allele in the recovery of executive functioning after combat-related traumatic brain injury. J. Neurosci. 31, 598–606 (2011).
Romanczyk, T. B. et al. Alterations in trkB mRNA in the human prefrontal cortex throughout the lifespan. Eur. J. Neurosci. 15, 269–280 (2002).
Al-Shawi, R. et al. Neurotoxic and neurotrophic roles of proNGF and the receptor sortilin in the adult and ageing nervous system. Eur. J. Neurosci. 27, 2103–2114 (2008).
Finan, J. D., Udani, S. V., Patel, V. & Bailes, J. E. The influence of the Val66Met polymorphism of brain-derived neurotrophic factor on neurological function after traumatic brain injury. J. Alzheimers Dis. 65, 1055–1064 (2018).
Feng, L. R. et al. Clinical predictors of fatigue in men with non-metastatic prostate cancer receiving external beam radiation therapy. Clin. J. Oncol. Nurs. 19, 744–750 (2015).
Feng, L. R., Fuss, T., Dickinson, K., Ross, A. & Saligan, L. N. Co-occurring symptoms contribute to persistent fatigue in prostate cancer. Oncology 96, 183–191 (2019).
de Azevedo Cardoso, T. et al. Neurotrophic factors, clinical features and gender differences in depression. Neurochem. Res. 39, 1571–1578 (2014).
Zhao, G. et al. Depression and anxiety among US adults: associations with body mass index. Int. J. Obes. 33, 257–266 (2009).
Chen, Z.-Y. et al. Variant Brain-Derived Neurotrophic Factor (BDNF) (Met66) alters the intracellular trafficking and activity-dependent secretion of wild-type BDNF in neurosecretory cells and cortical neurons. J. Neurosci. 24, 4401–4411 (2004).
Yennurajalingam, S. et al. Association between Daytime Activity, Fatigue, Sleep, Anxiety, Depression, and Symptom Burden in Advanced Cancer Patients: A Preliminary Report. J. Palliat. Med. 19, 849–856 (2016).
Kessels, E., Husson, O. & van der Feltz-Cornelis, C. M. The effect of exercise on cancer-related fatigue in cancer survivors: a systematic review and meta-analysis. Neuropsychiatr. Dis. Treat. 14, 479–494 (2018).
Luo, L. et al. Effect of aerobic exercise on BDNF/proBDNF expression in the ischemic hippocampus and depression recovery of rats after stroke. Behavioural Brain Res. 362, 323–331 (2019).
Quirié, A. et al. Comparative effect of treadmill exercise on mature BDNF production in control versus stroke rats. PLoS ONE 7, e44218 (2012).
Acknowledgements
The authors thank Cindy Clark, MSLS, NIH Library Writing Center, for paper editing. The authors would also like to thank Raisa Ionin, MLS, NIH Library, for her assistance with literature search (research in context). Funding: The present study is fully supported by the Division of Intramural Research of the National Institute of Nursing Research, National Institutes of Health, Bethesda, MD, USA. Grant number: ZIA NR000020-06.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was approved by the Institutional Review Board of the National Institutes of Health.
Informed consent
Written informed consent was obtained prior to study participation.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Feng, L.R., Juneau, P., Regan, J.M. et al. Brain-derived neurotrophic factor polymorphism Val66Met protects against cancer-related fatigue. Transl Psychiatry 10, 302 (2020). https://doi.org/10.1038/s41398-020-00990-4
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41398-020-00990-4
This article is cited by
-
Brain-Derived Neurotrophic Factor rs6265 polymorphism is associated with severe cancer-related fatigue and neuropathic pain in female cancer survivors
Journal of Cancer Survivorship (2023)
