
Abstract
Study design
Retrospective chart review.
Objectives
Sepsis is a leading preventable cause of death in patients with chronic spinal cord injury (SCI). Individuals with tetraplegia may exhibit different signs and symptoms of infection compared to those with paraplegia. In this study, we examine differences in vital signs (VS) and mental status between septic patients with tetraplegia and paraplegia with the goal of improving early identification of sepsis in this population.
Setting
Veterans hospital in Washington, USA.
Methods
Participants consisted of 19 patients with tetraplegia and 16 with paraplegia who were transferred from an SCI Service to a higher level of care with sepsis between June 1, 2010 and June 1, 2018 (n = 35). We compared VS between patients with tetraplegia and paraplegia at baseline and during sepsis including temperature, heart rate (HR), and blood pressure as well as presence/absence of altered mental status (AMS).
Results
While there were no significant VS differences between groups at baseline, septic patients with tetraplegia had lower maximum temperature (38.2 °C versus 39.2 °C, p = 0.003), lower maximum HR (106 versus 124 beats/minute, p = 0.004), and more frequent AMS compared to septic patients with paraplegia (79% versus 31%, p = 0.007).
Conclusion
Patients with tetraplegia may not be able to mount fever and tachycardia to the same degree as patients with paraplegia and may be more prone to developing AMS during sepsis. These findings suggest that changes to VS parameter cut-offs may improve sensitivity and be useful in identifying sepsis earlier in the tetraplegic population.
Similar content being viewed by others

Introduction
Sepsis is a leading preventable cause of death in patients with chronic spinal cord injury (SCI) [1]. Patients with SCI have increased susceptibility to infections due to several factors including a compromised respiratory system, neurogenic bladder requiring urinary catheters, and impaired sensation leading to pressure injuries [2]. Furthermore, the standardized mortality ratio (SMR), which quantifies the change in mortality of a cohort with respect to the general population, for sepsis among patients with SCI is extremely elevated at 172.3 [1]. One possible contributing factor is atypical signs and symptoms of infection in the SCI population, leading to delays or errors in diagnosis and management [3].
Sepsis is currently defined as infection with organ dysfunction, which can be represented by a Sequential [Sepsis-associated] Organ Failure Assessment (SOFA) score of two points or more [4]. Multiple studies have shown that early administration of antimicrobials improves clinical outcomes [5,6,7]. In the SCI population, a delay in empirical antibiotic treatment is common [8], with atypical clinical presentations possibly contributing to this delay [3].
Considering the effect of SCI on the autonomic nervous system (ANS), it is unsurprising that patients with SCI may have different signs and symptoms of infection compared to the general population. In addition to playing a critical role in maintaining physiologic homeostasis and responding to stressors, the ANS mediates interactions between the nervous and immune systems [9]. Spinal cord injury affects the ANS to varying degrees depending on the level and completeness of injury, suggesting that patients with tetraplegia may exhibit different signs and symptoms of infection compared to individuals with paraplegia. A Pubmed search on April 14, 2022 using keywords “spinal cord injury”, “sepsis”, and “vital signs” did not yield any studies examining vital sign (VS) differences between patients with tetraplegia and paraplegia during sepsis. As timely treatment of sepsis translates to improved clinical outcomes, it is important to characterize any differences in how these two groups respond to sepsis.
In this study, we examine differences in VS and mental status between septic patients with tetraplegia and paraplegia with the goal of improving early identification of sepsis in this population.
Methods
Study design
We conducted a retrospective chart review of all patients with SCI who were transferred from the Veterans Affairs Puget Sound Health Care System SCI Service to a higher level of care with a diagnosis of sepsis between June 1, 2010 and June 1, 2018. Collection of data from the electronic medical record for research purposes was approved by the institutional review board.
Participants
Our SCI Unit contains 38 beds with an average daily census of 24.1 patients, with both acute and chronic SCI, during the study period. Unexpected transfers off the SCI Service had been previously identified for quality assurance purposes. Patients who were identified as having sepsis by the accepting team were included in our study. For patients with multiple transfers due to sepsis, we only included data from the first episode to simplify subsequent statistical analyses. We also excluded one patient from the heart rate (HR) analyses who had a cardiac pacemaker. Demographic data were collected including age, sex, duration of injury, length of stay (LOS), neurologic level of injury, and American Spinal Injury Association Impairment Scale (AIS). We reviewed medical records to determine which patients had ever experienced autonomic dysreflexia (AD) as an indicator of degree of autonomic dysfunction. Outcomes were then compared between patients with tetraplegia (n = 19) and paraplegia (n = 16).
Outcome Measures
We extracted baseline, asymptomatic VS including temperature (Tb), heart rate (HRb), systolic blood pressure (SBPb), and diastolic blood pressure (DBPb). These were calculated by averaging five sets of VS using one of three methods. Preferably, we averaged the last five VS measurements that were obtained prior to hospital discharge. If this was unobtainable (e.g., patient died during admission), we averaged five consecutive VS measurements from prior to transfer, at least 48 h prior to symptom development. Finally, if this was not possible (e.g., patient was symptomatic upon admission), we averaged the five most recent sets of outpatient VS. To obtain VS during sepsis, we extracted the highest temperature (Tmax), highest heart rate (HRmax), lowest systolic blood pressure (SBPmin), and lowest diastolic blood pressure (DBPmin) as well as laboratory values (if performed) in the 24 h prior to transfer off the SCI Service. Collected laboratory values included white blood cell count, lactate, platelets, prothrombin time (PT), international normalized ratio (INR), total bilirubin, and creatinine. We also recorded the presence/absence of altered mental status (AMS) in the 24 h prior to transfer by reviewing progress notes from nursing and physician staff. To determine if there was a significant difference in VS changes from baseline to sepsis, we compared these differences between patients with tetraplegia and paraplegia.
Statistical analysis
Data are expressed as mean ± standard deviation. Two-tailed unpaired t-test and Fisher’s exact test were used to compare demographic data between patients with tetraplegia and paraplegia. The two-tailed Mann–Whitney U test was used to compare VS and laboratory data between patients with tetraplegia and paraplegia. Two-tailed Fisher’s exact test was used to compare the percentage of patient with AMS between those with tetraplegia and paraplegia. All statistical analyses were performed with SPSS 19 for Windows. Statistical significance was set at p < 0.05 for all tests.
Results
During the study period, there were 151 unexpected transfer events that occurred in 90 patients and 36% (n = 54) were due to sepsis. Multiple patients were transferred more than once, but only the initial episode was considered in the current study (n = 35). Patient characteristics are shown in Table 1. Age, years since initial SCI, proportion of patients with injuries less than six months duration, LOS, and distribution of AIS classification did not significantly differ between the two groups. As expected, patients with tetraplegia were significantly more likely to have had a previous episode of AD compared to patients with paraplegia (68% versus 19%, p = 0.006). In addition to being diagnosed with sepsis by the accepting team, all patients met at least two out of four systemic inflammatory response syndrome (SIRS) criteria (temperature > 38.0 °C or <36.0 °C, tachycardia > 90 beats/minute, tachypnea >20 breaths/minute, and WBC > 12 × 109 or <4 × 109) in the 24 h prior to transfer and had at least one suspected source of infection.
While there were no significant differences in VS between patients with tetraplegia and paraplegia at baseline, there were significant VS differences between the two groups during sepsis (Table 2). The Tmax among patients with tetraplegia was 38.2 °C compared to 39.2 °C in patients with paraplegia (p = 0.003). In addition, HRmax was significantly lower among patients with tetraplegia compared to paraplegia (106 versus 124 bpm, p = 0.004). There was no significant difference in SBPmin or DBPmin between patients with tetraplegia and paraplegia. Comparing the degree of change in VS from baseline to sepsis, the rise in temperature and HR from baseline to sepsis was significantly lower in patients with tetraplegia compared to patients with paraplegia, while SBP and DBP both fell to a similar degree in both groups. Finally, the prevalence of AMS among septic patients with tetraplegia was significantly higher compared to patients with paraplegia (79% versus 31%, p = 0.007) (Table 3).
There were no significant differences in any laboratory value between septic patients with tetraplegia and paraplegia (Table 4).
Discussion
Our findings suggest that patients with tetraplegia may have a different physiologic response to sepsis compared to patients with paraplegia, manifest in clinical parameters assessed on clinical sepsis screening tools. Specifically, patients with tetraplegia are not able to mount as high of a temperature or HR in response to systemic infection. In addition, AMS is much more common during sepsis among patients with tetraplegia compared to patients with paraplegia. These findings are unlikely to be due to differences in sepsis severity, as there were no significant differences in blood pressure or laboratory values between the two groups.
Impaired thermoregulation
In able-bodied individuals, fever is the result of an increase in the hypothalamic set point, which is triggered by endogenous and/or exogenous pyrogenic substances. These pyrogenic substances induce the release of endogenous pyrogenic cytokines, triggering a cascade resulting in disinhibition of thermogenic neurons in the anterior hypothalamus, thus establishing a new higher hypothalamic set point. Mechanisms mediated by the sympathetic nervous system, including shivering and vasoconstriction, then raise the body temperature to match the new set point [10].
In tetraplegia, heat conservation and thermogenesis may be inhibited to a greater degree compared to paraplegia. Following SCI, individuals experience a loss of vasomotor control below the level of injury [11]. Thus, individuals with tetraplegia have a greater degree of vasomotor impairment compared to individuals with paraplegia, resulting in more profound thermoregulatory impairment. Guttman et al. showed that individuals with tetraplegia have lower core temperatures compared to able-bodied individuals in the setting of colder ambient temperatures (18–20 °C) [12]. In addition, in this temperature range, the skin temperature of patients with tetraplegia was significantly higher compared to able-bodied individuals, demonstrating an impaired ability to vasoconstrict peripheral vasculature to conserve heat.
Furthermore, patients with tetraplegia have impaired shivering, which represents the body’s most potent method of increasing metabolism and heat production [13]. Downey et al. demonstrated that individuals with SCI are only able to shiver in muscles with intact innervation [14]. As a result, patients with tetraplegia were only able to increase their metabolism by 100% in cold temperatures, compared to 200% in patients with paraplegia. Therefore, septic patients with tetraplegia may be unable to match their body temperature to the higher hypothalamic set point due to impaired shivering and vasoconstriction. In our study, septic patients with tetraplegia had a Tmax that was 1.0 °C lower than patients with paraplegia, supporting this hypothesis.
Previous research investigating fever in response to infection among patients with SCI is mixed. Earlier studies suggested that individuals with tetraplegia are able to mount fevers of a similar magnitude as able-bodied individuals in response to infection [15], while a more recent study showed an impaired ability to mount temperature >38 oC in response to infection/inflammation in patients with tetraplegia and paraplegia [16]. An important distinction between the previous studies and our study is that our cohort only included patients diagnosed with sepsis, while the previous studies included patients with infections/inflammation of unclear severity, possibly accounting for the different findings.
Cardiovascular dysfunction
Heart rate
In addition to elevated temperature, sepsis is also characterized by cardiovascular dysfunction. The onset of sepsis is often accompanied by hypovolemia due to vasodilation and leakage of plasma into the extravascular space. The resulting hypotension is sensed by baroreceptors in the carotid sinus and aortic arch, triggering increased sympathetic outflow to the heart and vasculature in an effort to maintain cardiac output [17, 18]. Following tetraplegia, supraspinal control of preganglionic sympathetic neurons in the thoracolumbar spinal cord is impaired. In our study, patients with tetraplegia had significantly lower HR during sepsis compared to patients with paraplegia, suggesting that sympathetically mediated tachycardia in the setting of hypotension is blunted in this population.
Though no previous literature has compared HRmax during sepsis in patients with tetraplegia compared to paraplegia, several studies examining the cardiovascular response to exercise in the SCI population provide support for impaired sympathetically mediated tachycardia in this population. During exercise, early increases in HR are thought to be dependent upon supraspinal regulation of the sympathetic nervous system [19]. Previous studies have shown that tetraplegia impairs the capacity to increase HR immediately after onset of exercise compared to able-bodied controls [19, 20]. In addition, HR immediately after onset of exercise is lower in individuals with tetraplegia compared to those with paraplegia, in whom supraspinal control of the sympathetic outflow to the heart is relatively less impaired [19]. These findings support our hypothesis that impaired supraspinal control of sympathetic outflow to the heart in patients with tetraplegia blunts sepsis-induced tachycardia.
Blood pressure
Our finding that baseline blood pressure was not significantly different in patients with predominantly chronic tetraplegia compared to patients with paraplegia is at odds with several previous publications [21,22,23,24]. Our study may have been underpowered to detect a small blood pressure difference between the two groups. A study by Zhu et al. supports this possibility, as it showed that mean baseline SBP over a five-year period among individuals with tetraplegia was only 5 mmHg and 10 mmHg lower compared to individuals with high and low paraplegia, respectively [25].
To our knowledge, there is no literature examining differences in blood pressure in septic patients with tetraplegia versus paraplegia. In our study, there was no difference in blood pressure nadir during sepsis between the two groups, consistent with the hypothesis that sepsis-induced hypotension is largely independent of the ANS. Though cardiac dysfunction and hypovolemia contribute to septic shock, peripheral vasodilation represents the major mechanism [26]. Vasodilation in septic shock is mediated by increased nitric oxide and prostacyclin synthesis, triggered by endotoxin [27, 28]. In addition, vasodilation occurs in the setting of dramatically increased peripheral levels of catecholamines [29], suggesting that vasodilation in septic shock is independent of the sympathetic nervous system. Therefore, it is plausible that sepsis may affect the blood vessels of patients with tetraplegia and paraplegia to the same degree, regardless of the integrity of the sympathetic nervous system.
Altered mental status
Alteration in mental status is a common early finding in severe sepsis, with prevalence ranging from 9–71% [30,31,32,33,34,35]. Sepsis-associated encephalopathy (SAE) describes the diffuse cerebral dysfunction that accompanies sepsis in the absence of direct central nervous system infection, structural abnormality, or other types of encephalopathy such as hepatic or renal encephalopathy.
Evidence that impaired cerebral autoregulation may contribute to SAE comes from Bowton et al., who showed that cerebral blood flow (CBF) was significantly lower in nine encephalopathic septic patients compared to normal age-matched values [36]. In addition, this depression did not correlate with changes in mean arterial pressure. It is possible that reduced CBF results in ischemia and contributes to AMS.
Though there was no significant blood pressure difference between septic patients with tetraplegia and paraplegia in our study, and blood pressure dropped to a similar degree compared to baseline, the prevalence of AMS in patients with tetraplegia was significantly higher compared to patients with paraplegia. Given the absence of significant blood pressure differences between the two groups, cerebral perfusion pressure could not have accounted for the observed difference in AMS. However, impaired cerebral autoregulation and/or cerebrovascular reactivity leading to diminished CBF among patients with tetraplegia is a possible explanation for this difference. Using a clinically relevant model of transient hypertension in rats, Phillips et al. showed that chronic repetitive cerebral hyperperfusion such as seen with AD, resulted in impaired cerebrovascular endothelial function and profibrotic cerebrovascular stiffening characterized by reduced distensibility [37]. As patients with tetraplegia are more likely to experience repetitive transient hypertension due to AD compared to patients with paraplegia, this group is more likely to have the impaired cerebrovascular endothelial function and cerebrovascular stiffening described above. In our study, 68% of patients with tetraplegia experienced AD, compared to only 19% of patients with paraplegia. Furthermore, the majority of patients with tetraplegia in our study were injured for >6 months, a duration that would allow the above-mentioned vascular changes to occur in response to recurrent AD episodes. Thus, given the importance of intact endothelial function and cerebrovascular distensibility to the regulation of the cerebrovasculature [38,39,40,41,42], it is plausible that patients with tetraplegia, but not paraplegia, have impaired cerebrovascular regulation during sepsis leading to reduced CBF and subsequent AMS.
Clinical implications
Recognition that patients with tetraplegia may not mount fever or tachycardia to the same degree as patients with paraplegia has important implications regarding sepsis screening. The Surviving Sepsis Campaign recommends that hospitals have a performance improvement program for sepsis, including sepsis screening, which is associated with decreased mortality in several studies [43, 44]. A prior study of patients with recent-onset SCI determined that a screening tool for earlier clinical deterioration should use a lower SBP cut-off for patients with neurological levels T6 or rostral to avoid false-positive screens, but the study did not assess patients with sepsis [24]. Currently, there is no sepsis screening tool that has been validated in the SCI population.
In addition to differences in VS, we observed that septic patients with tetraplegia may be more likely to experience AMS compared to patients with paraplegia, suggesting that this population may benefit from interventions aimed specifically at SAE [45,46,47,48,49].
Limitations
There are several limitations to our study. Given a relatively small sample size of 35, the likelihood of a Type II error is increased in our study. In addition, all our study participants were male, limiting the generalizability of the results. For septic VS data, we collected the most extreme values for temperature, HR, and blood pressure, which occasionally occurred at different time points, not reflecting how VS would be interpreted from a sepsis screening standpoint. Analysis of respiratory rate, which is a component of both SIRS criteria and qSOFA, would have been useful, but we chose to exclude this measure due to accuracy concerns. We did not have a measure of autonomic completeness such as the International Standards to document remaining Autonomic Function after SCI (ISAFSCI) [50], though we did quantify the number of patients in each group who experienced AD, providing some information regarding each patient’s propensity to episodes of transient hypertension. Finally, an objective measure of AMS such as the Glascow Coma Scale would have provided useful detail but was not available in our data set.
Conclusion
Our study, the first to our knowledge to examine differences in how individuals with tetraplegia and paraplegia respond to sepsis, shows that patients with tetraplegia may not be able to mount fever and tachycardia to the same degree as patients with paraplegia. In addition, AMS was significantly more prevalent in the tetraplegic group, possibly secondary to impaired cerebral autoregulation and/or cerebrovascular reactivity. These findings suggest that changes to VS parameter cut-offs may improve sensitivity and be useful in identifying sepsis earlier in the tetraplegic population. Furthermore, particular importance should be placed on identifying AMS in patients with tetraplegia, as this may be an early and frequent sign of sepsis in this population.
Data availability
Data are available from the corresponding author on reasonable request.
References
Soden RJ, Walsh J, Middleton JW, Craven ML, Rutkowski SB, Yeo JD, et al. Causes of death after spinal cord injury. Spinal Cord. 2000;38:604–10.
Brommer B, Engel O, Kopp MA, Watzlawick R, Muller S, Pruss H, et al. Spinal cord injury-induced immune deficiency syndrome enhances infection susceptibility dependent on lesion level. Brain. 2016;139(Pt 3):692–707.
Ditunno JF Jr, Formal CS. Chronic spinal cord injury. N Engl J Med. 1994;330:550–556.
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315:801–10.
Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer P, et al. Surviving Sepsis Campaign: International guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43:304–77.
Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34:1589–96.
Ferrer R, Martin-Loeches I, Phillips G, Osborn TM, Townsend S, Dellinger RP, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42:1749–55.
Evans CT, Burns SP, Chin A, Weaver FM, Hershow RC. Predictors and outcomes of antibiotic adequacy for bloodstream infections in veterans with spinal cord injury. Arch Phys Med Rehabil. 2009;90:1364–70.
Kenney MJ, Ganta CK. Autonomic nervous system and immune system interactions. Compr Physiol. 2014;4:1177–200.
Schortgen F. Fever in sepsis. Minerva Anestesiol. 2012;78:1254–64.
Normell LA. Distribution of impaired cutaneous vasomotor and sudomotor function in paraplegic man. Scand J Clin Lab Investig Suppl. 1974;138:25–41.
Guttmann L, Silver J, Wyndham CH. Thermoregulation in spinal man. J Physiol. 1958;142:406–19.
Jacobs I, Martineau L, Vallerand AL. Thermoregulatory thermogenesis in humans during cold stress. Exerc Sport Sci Rev. 1994;22:221–50.
Downey JA, Miller JM, Darling RC. Thermoregulatory responses to deep and superficial cooling in spinal man. J Appl Physiol. 1969;27:209–12.
Schmidt KD, Chan CW. Thermoregulation and fever in normal persons and in those with spinal cord injuries. Mayo Clin Proc. 1992;67:469–75.
Trbovich M, Li C, Lee S. Does the CDC definition of fever accurately predict inflammation and infection in persons with SCI? Top Spinal Cord Inj Rehabil. 2016;22:260–8.
Groves AC, Griffiths J, Leung F, Meek RN. Plasma catecholamines in patients with serious postoperative infection. Ann Surg. 1973;178:102–7.
Leinhardt DJ, Arnold J, Shipley KA, Mughal MM, Little RA, Irving MH, et al. Plasma norephinephrine concentrations do not accurately reflect sympathetic nervous system activity in human sepsis. Am J Physiol. 1993;265(2 Pt 1):E284–8.
Dela F, Mohr T, Jensen CM, Haahr HL, Secher NH, Biering-Sorensen F, et al. Cardiovascular control during exercise: insights from spinal cord-injured humans. Circulation. 2003;107:2127–33.
Takahashi M, Sakaguchi A, Matsukawa K, Komine H, Kawaguchi K, Onari K, et al. Cardiovascular control during voluntary static exercise in humans with tetraplegia. J Appl Physiol. 2004;97:2077–82.
Katzelnick CG, Weir JP, Jones A, Galea M, Dyson-Hudson TA, Kirshblum SC, et al. Blood pressure instability in persons with spinal cord injury: evidence from a 30-day home monitoring observation. Am J Hypertens. 2019;32:938–44.
Goh MY, Millard MS, Wong EC, Berlowitz DJ, Graco M, Schembri RM, et al. Comparison of diurnal blood pressure and urine production between people with and without chronic spinal cord injury. Spinal Cord. 2018;56:847–55.
West CR, Mills P, Krassioukov AV. Influence of the neurological level of spinal cord injury on cardiovascular outcomes in humans: a meta-analysis. Spinal Cord. 2012;50:484–92.
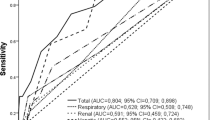
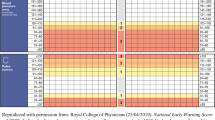
Ahmed WA, Rouse A, Griggs KE, Collett J, Dawes H. Poor specificity of National Early Warning Score (NEWS) in spinal cord injuries (SCI) population: a retrospective cohort study. Spinal Cord. 2020;58:165–173.
Zhu C, Galea M, Livote E, Signor D, Wecht J. A retrospective chart review of heart rate and blood pressure abnormalities in veterans with spinal cord injury. J Spinal Cord Med. 2013;36:463–475.
Angus DC, van der Poll T. Severe sepsis and septic shock. N Engl J Med. 2013;369:840–51.
Cobb JP, Danner RL. Nitric oxide and septic shock. JAMA. 1996;275:1192–6.
Zardi EM, Zardi DM, Dobrina A, Afeltra A. Prostacyclin in sepsis: a systematic review. Prostaglandins Other Lipid Mediat. 2007;83:1–24.
Benedict CR, Rose JA. Arterial norepinephrine changes in patients with septic shock. Circ Shock. 1992;38:165–72.
Maher J, Young GB. Septic encephalopathy. J Intensive Care Med. 1993;8:177–87.
Eidelman LA, Putterman D, Putterman C, Sprung CL. The spectrum of septic encephalopathy. Definitions, etiologies, and mortalities. JAMA. 1996;275:470–3.
Bolton CF, Young GB. Sepsis and septic shock: central and peripheral nervous systems. In: Sibbald WJ, Sprung CL, editors. New horizons: perspectives on sepsis and septic shock. Fullerton: Society of Critical Care Medicine; 1986. p 157–71.
Pine RW, Wertz MJ, Lennard ES, Carrico CJ, Minshew BH. Determinants of organ malfunction or death in patients with intra-abdominal sepsis. A discriminant analysis. Arch Surg. 1983;118:242–9.
Sprung CL, Peduzzi PN, Shatney CH, Schein RM, Wilson MF, Sheagren JN, et al. Impact of encephalopathy on mortality in the sepsis syndrome. The Veterans Administration systemic sepsis cooperative study. Crit Care Med. 1990;18:801–6.
Young GB, Bolton CF, Archibald TM, Austin TW, Wells GA. The electroencephalogram in sepsis-associated encephalopathy. J Clin Neurophysiol. 1992;9:145–52.
Bowton DL, Bertels NH, Prough DS, Stump DA. Cerebral blood flow is reduced in patients with sepsis syndrome. Crit Care Med. 1989;17:399–403.
Phillips AA, Matin N, Jia M, Squair JW, Monga A, Zheng MMZ, et al. Transient hypertension after spinal cord injury leads to cerebrovascular endothelial dysfunction and fibrosis. J Neurotrauma. 2018;35:573–81.
Phillips AA, Krassioukov AV, Ainslie PN, Warburton DE. Perturbed and spontaneous regional cerebral blood flow responses to changes in blood pressure after high level spinal cord injury: the effect of midodrine. J Appl Physiol. 2014;116:645–53.
Phillips AA, Warburton DE, Ainslie PN, Krassioukov AV. Regional neurovascular coupling and cognitive performance in those with low blood pressure secondary to high-level spinal cord injury: improved by alpha-1 agonist midodrine hydrochloride. J Cereb Blood Flow Metab. 2014;34:794–801.
Phillips AA, Ainslie PN, Krassioukov AV, Warburton DE. Regulation of cerebral blood flow after spinal cord injury. J Neurotrama. 2013;30:1551–63.
Phillips AA, Chan FH, Zheng MM, Krassioukov AV. Neurovascular coupling in humans: physiology, methodological advances and clinical implications. J Cereb Blood Flow Metab. 2016;36:647–64.
Willie CK, Tzeng YC, Fisher JA, Ainslie PN. Integrative regulation of human brain blood flow. J Physiol. 2014;592:841–59.
Levy MM, Dellinger RP, Townsend SR, Linde-Zwirble WT, Marshall JC, Biron J, et al. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Crit Care Med. 2010;38:367–74.
Jones SL, Ashton CM, Kiehne L, Gigliotti E, Bell-Gordon C, Disbot M, et al. Reductions in sepsis mortality and costs after design and implementation of a nurse-based early recognition and response program. Jt Comm J Qual Patient Saf. 2015;41:483–91.
Freund HR, Ryan JA Jr, Fischer JE. Amino acid derangements in patients with sepsis: treatment with branched chain amino acid rich infusions. Ann Surg. 1978;188:423–30.
Toklu HZ, Uysal MK, Kabasakal L, Sirvanci S, Ercan F, Kaya M, et al. The effects of riluzole on neurological, brain biochemical, and histological changes in early and late term sepsis in rats. J Surg Res. 2009;152:238–48.
Wilson JX. Mechanism of action of vitamin C in sepsis: ascorbate modulates redox signaling in endothelium. Biofactors. 2009;35:5–13.
Busund R, Koukline V, Utrobin U, Nedashkovsky E. Plasmapheresis in severe sepsis and septic shock: a prospective, randomized, controlled trial. Intensive Care Med. 2002;28:1434–9.
Moss RF, Parmar NK, Tighe D, Davies DC. Adrenergic agents modify cerebral edema and microvessel ultrastructure in porcine sepsis. Crit Care Med. 2004;32:1916–21.
Krassioukov A, Biering-Sorensen F, Donovan W, Kennelly M, Kirshblum S, Krogh K, et al. International standards to document remaining autonomic function after spinal cord injury. J Spinal Cord Med. 2012;35:201–10.
Funding
No financial assistance was received in support of the study. This material is the result of work supported by Veterans Affairs Puget Sound Health Care System. The contents of this work do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Author information
Authors and Affiliations
Contributions
SHS was responsible for designing the study, extracting and analyzing data, interpreting results, writing the manuscript, and creating the tables. KMS contributed to extracting data, interpreting results, writing and editing the manuscript. SPB contributed to analyzing the data, interpreting results, and editing the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was approved by the Veterans Affairs Puget Sound Institutional Review Board (MIRB# 01692).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Song, S.H., Sankary, K.M. & Burns, S.P. Vital sign differences between septic patients with tetraplegia and paraplegia. Spinal Cord Ser Cases 8, 87 (2022). https://doi.org/10.1038/s41394-022-00553-3
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41394-022-00553-3
