
Abstract
Objective
This study was conducted to explore the expression of transforming growth factor-beta 1 (TGF-β1) and its correlation with autophagy markers in the bladder of rats with neurogenic lower urinary tract dysfunction (NLUTD) post spinal cord injury (SCI).
Study design
A total of 36 male Wistar rats were randomly divided into the SCI group and control group. Rats in the SCI group were subjected to T10–T11 spinal cord transection. At day 1, 4, and 7, 6 rats were euthanized daily and the Basso, Beattie and Bresnahan score (BBB score), post-void residual (PVR), urinary bladder function score (UBFS) and bladder weight were assessed. The expression TGF-β1 and autophagy markers were evaluated by immunofluorescence staining, Western bolt, and qRT-PCR.
Setting
A total of 36 male Wistar rats were randomly divided into the SCI group and control group, with three time points in each group.
Participants
Not applicable.
Results
SCI modeling impaired the motor function of the hind limbs and the bladder function of rats. NLUTD muscle exhibited a punctated immunostaining pattern for LC3, suggesting the accumulation of autophagosomes. Our results further indicated that compared with the control group, the expression levels of TGF-β1 and LC3 were increased, while the level of P62 was decreased after SCI modeling.
Conclusion
TGF-β1 was significantly increased in SCI rats with NLUTD and was correlated with autophagy markers LC3 and p62.
Similar content being viewed by others

Introduction
Spinal cord injury (SCI) is a serious central system injury, which causes a great economic burden on the society. It leads to motor and sensory dysfunction and a range of autonomous deficits [1]. Neurogenic lower urinary tract dysfunction (NLUTD) is one of the most serious complications of SCI. More than 80% of patients with spinal cord injury exhibit some degree of bladder dysfunction [2]. NLUTD caused by SCI might lead to decrease of bladder capacity and increase of detrusor pressure, which often leads to urinary incontinence, urinary tract infection, vesicoureteral reflux, and renal impairment [2]. NLUTD has a huge impact on the quality of patients’ lives [3]. However, no effective etiological treatment has been developed for SCI patients with NLUTD. Therefore, it is necessary to find the pathological mechanism of NLUTD after SCI.
Autophagy is an important cellular pathway involved in the degradation of proteins and organelle, which also maintains cell homeostasis [4]. It plays a cytoprotective role in response to most forms of cellular stress [5]. LC3 is a key autophagic marker, as it is post-translationally modified from its inactive form (LC3-I) to its active form (LC3-II) – an autophagosome component [6]. Another widely used marker for autophagic flux is the autophagy receptor sequestosome 1 (SQSTM1, p62), which physically links autophagic cargo to the autophagic membrane and is itself degraded by autophagy [7, 8]. Changes of autophagic markers were detected in the spinal cord after SCI [9]. Our previous studies have found that autophagy was activated during the recovery of the bladder after SCI [10]. However, the mechanism is not fully understood.
Transforming growth factor-beta 1 (TGF-β1) is a potential growth regulatory protein, which is involved in a variety of pathophysiological processes in vivo. It regulates cell differentiation, survival and proliferation and also promotes tissue repair following injury [11]. TGF-β1 also plays an important role in the regulation and signal transmission to the process of nervous system injury, degeneration, repair and regeneration [12]. Previous work showed that TGF-β1 injection into the subarachnoid space of rats with SCI induced partial restorations in hindlimb motor function [13], suggesting that TGF-β1 might be involved in neuroplasticity following SCI. It has also been reported that TGF-β1 was released to stimulate elastin and collagen for bladder wall remodeling in NLUTD post SCI [14]. Previous studies have shown that TGF-β1 induces autophagy in several other cellular systems. One major study found that TGF-β1 actives autophagy in denervated skeletal muscle, as manifested by an increase in LC3 and a decrease in P62 [15].
The detrusor loses central nervous system innervation in individuals with SCI. Therefore, there may be a correlation between TGF-β1 and detrusor autophagy in NLUTD patients. Up to now, there is no study on the association between TGF-β1 and autophagy in detrusor of NLUTD after SCI. In this study, we established a NLUTD model after SCI and observed the expression of TGF-β1 and autophagy in different process of NLUTD after spinal cord injury.
Materials and methods
Experimental animals and grouping
A total of 36 adult male Wistar rats (6–7 weeks old, weighing 240–260 g) were purchased from Jinan Pengyue Experimental Animal Breeding Co., Ltd. (Jinan, China) and were housed on a 24 h day-night cycle. They were randomly divided into two equal groups: SCI group (n = 18) and the control (sham surgery) group (n = 18). Kinematic scores were performed on day 1, 2, 3, 4, 5, 6 and 7 after surgery in both groups. On the 1st, 4th, and 7th days after spinal cord injury, 6 rats were sacrificed in the control group and the SCI group, respectively. Among these rats, their bladder tissues from five rats were equally divided into two parts, half for western blotting and the other half for PCR. The bladder tissue from the remaining sacrificed rat in each group was used for immunohistochemistry. In order to avoid the influence of different parts of the material on the results, we took the whole bladder as the research material. The bladder smooth muscle was collected for immunohistochemical staining, and the bladder dome area was selected for observation. All the experimental procedures were in accordance with the guidelines for animal scientific procedures provided by Shandong University Ethics Committee.
Establishion of the SCI model
After 1 week of adaptive feeding, rats were anesthetized with 10% chloral hydrate (3 ml/kg) administered by intraperitoneal injection. The modified Hassan Shaker’s spinal cord transection method was used to establish the SCI model. After successful anesthetization, the lower back region of the rats was shaved and they were placed in a prone position on the operating table. Rats were fixed on the experimental platform in the prone position, and then skin preparation, disinfection and aseptic operation hole towels were routinely prepared. T10 was taken as the center. A 2.0 cm incision was taken along the spinal direction to cut open the skin and muscles to expose the spinous process and fully expose the vertebral body. The T10–T11 lamina with rongeur was carefully removed avoiding injury to the spinal cord and dura mater as much as possible. The T10–T11 segments of spinal cord were fully exposed. The spinal cord was transectioned completely at the level of T10 with a surgical blade [16]. During this process, the rat’s hind limbs and tails showed spastic convulsions continuing for a few seconds. After the operation, the muscles, subcutaneous tissue and skin were sutured layer by layer.
The control group only underwent laminectomy at T10–T11 level without SCI.
The rats were intraperitoneally injected with penicillin immediately after operation to prevent infection and for 3 consecutive days (Benzylpenicillin Sodium from Shandong Lukang Pharmaceutical Company Ltd., Shandong Jining, China, 80000 units/days/per animal).
Behavioral analysis
Functional analysis was first assessed using the Basso, Beattie, and Bresnahan (BBB) locomotor scale according to previously established behavior tests [17]. BBB scores were measured on a smooth and wide ground at 1, 2, 3, 4, 5, 6 and 7 days. It was done by two observers who were familiar with the BBB score but did not know the experimental grouping. The measurement time was at least 4 minutes.
Evaluation of bladder function
We used two noninvasive methods to evaluate the bladder function: the post-void residual (PVR) and the urinary bladder function score (UBFS).
(1) PVR. The bladder volume of the rats was evaluated manually and residual urine were recorded twice a day. Immediately after we observed the rat urinating, the bladder was emptied by applying pressure with the index finger and middle finger to the most central part of the abdomen. The urine excreted by the rats was collected in a graduated glass tube and recorded [10].
(2) UBFS. The four-point UBFS was evaluated twice a day after surgery according to a previous study [10, 18]. We mainly assessed the bladder function of rats in UBFS by the frequency of artificially assisted urination and hematuria. Our researchers performed daily squeezing of the rat’s bladder according to the extent of the rat’s urine retention. Our researchers first observed the urination habits of the rats. After feeding, the rats were induced to urinate by tapping the bladder area, and the bladder filling in the lower abdomen was touched after urination. If the bladder of the rat was relatively distended, it indicated that the residual urine volume was large, and the rat was manually massaged to urinate. After the urine was collected, we also performed a routine urine test to observe whether there were red blood cells in the urine. 0 = complete loss of function (manual expression of bladder 3×/day, the urine contains blood), 1 = partial recovery of UBF (manual expression 2×/day, urine may contain blood), 2 = partial recovery of UBF (partial/ complete release of sphincter spasm, manual expression 1×/day, still blood in urine), 3 = advanced recovery (manual expression 1×/day, no blood in urine), 4 = physiological UBF. In the control group of rats, residual urine was indeed not able to be manually squeezed out of the rat after urination. Therefore, the rats in the control group did not need artificial urination and were scored 4 points.
Bladder weight
The rats were killed at 1, 4 or 7 days after surgery. Bladders were excised above the bladder neck and harvested. The perivesical fat tissues were removed carefully, and the bladder weights (n = 6 for each group) were measured by an analytical balance (Sartorius, Germany) [19].
Immunofluorescence staining
Immunofluorescence staining was used to confirm the locations of the TGF-β1 and autophagy-associated proteins. The harvested bladders were fixed with 4% paraformaldehyde for 48 h, dehydrated, and paraffin-embedded, and then cross-sectionally cut into 5 μm. After deparaffinating, rehydration and antigen retrieval, the sections were blocked with 5% albumin from goat serum for 1 h at room temperature. Primary antibody incubation was conducted overnight at 4 °C; primary antibodies included: rabbit anti-TGF-β1 (1:100; Sanying, Wuhan, China), rabbit anti-LC3 (1:200; Abcam, USA), rabbit anti-P62 (1:100; Abcam, USA). The sections were then stained for 1 h at room temperature with fluorescent Alexa488 goat anti-rabbit secondary antibody (1:1000, Abcam, USA), followed by a 5 min DAPI (Beyotime, Shanghai, China) staining. The images were captured on NanoZoomer S60 (Hamamatsu, Japan) and analyzed by Image Pro Plus (Media Cybernetics, Inc, Rockville, MD, USA).
Protein extraction and western-blotting analysis
The harvested bladder was homogenized in RIPA lysis buffer with protease and phosphatase inhibitor (Beyotime, Shanghai, China), centrifuged to collect the supernatant. The protein concentration was determined using a bicinchoninic acid (BCA) assay kit (Beyotime, Shanghai, China). Proteins were separated on a 12% SDS-PAGE gel and transferred to a nitrocellulose membrane. Then, the membrane was blocked with 5% freshly prepared nonfat milk-TBST (Tris-buffered saline, 0.1% Tween 20) for 2 h at room temperature, and then incubated with primary rabbit polyclonal antibodies overnight at 4 °C: anti-TGF-β1 (1:100; Abcam, USA), anti-LC3 (1:1000; Abcam, USA), anti-P62 (1:200; Abcam, USA). They were incubated with HRP-conjugated goat anti-rabbit secondary antibody (1:3000, Abcam, USA) for 1 h at room temperature. GAPDH was used as an internal loading control (anti-GAPDH, 1:3000, Sanying, Wuhan, China). ECL detection reagent and X-ray film were used for protein detection. Quantification of band intensity was performed by Image J (National Institutes of Health, Bethesda, MD, USA).
RNA extraction and quantitative real-time PCR
The total RNA was extracted from fresh detrusor samples using TRIzol (Takara, Shiga, Japan) according to the manufacturer’s protocol. RNA concentration was estimated using the Biowave DNA UV–Vis spectrophotometer (Biochrom, Cambridge, UK). cDNA was synthesized using the ReverTra Ace q-PCR RT Kit (TOYOBO, Japan). Quantitative real-time PCR (q-PCR) was performed for target RNAs with SYBR Green q-PCR kits (Accurate Biology, China). q-PCR of the same sample was performed for β-actin expression as internal control. The primers were synthesized by BioSune Biotechnology (Shanghai) Co., Ltd. The primers used were as follows:
TGF-β1:
forward: 5′-TGACATGAACCGACCCTTCC-3′;
reverse: 5′-TGTGGAGCTGAAGCAGTAGT-3′.
LC3:
forward: 5′-TTGGTCAAGATCATCCGGCG-3′;
reverse:5′-GTCAGCGATGGGTGTGGATA-3′.
P62:
forward: 5′-CTGTGGTGGGAACTCGCTAT-3′;
reverse: 5′-GCCAAAGGGGTTGGGAAA-3′.
β-actin:
forward: 5′-CTCTGTGTGGATTGGTGGCT-3′;
reverse: 5′- CGCAGCTCAGTAACAGTCCG-3′.
Statistical analysis
Three independent experiments were done in each group. Results are shown as mean ± standard deviation (SD). The GraphPad Prism 6 software (GraphPad Software, USA) was used for analyses. The normality of the datasets obtained were assessed with the K-S test first, and the comparison was determined by Student’s t test between two groups and by one-way ANOVA with Bonferroni post-tests among multiple groups. A p < 0.05 was considered statistically significant.
Results
Assessment of motor functions, bladder function and the bladder weight
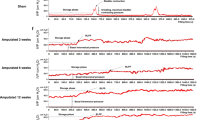
BBB rating scale was used to evaluate the motor function of both hindlimbs of rats. After surgery, the motor function of both hindlimbs of SCI rats was lost and paralyzed (Fig. 1A). The locomotor functions of the rats started to recovery at day 6. The rats in the control group behaved normal and the scores were 21 points at each time point. BBB scores of SCI rats in each day were significantly decreased compared with that in control group (p < 0.01). In the first day after operation, dysuria was seen in some rats, accompanied by hematuria. The PVR of rats in SCI group were significantly increased (p < 0.01) compared with that in control group, and decreased gradually from day 1 to day 7 after SCI modeling (Fig. 1B). The UBFS scores of SCI group were significantly decreased after SCI modeling, and gradually recovered from day 1 to day 7 (Fig. 1C). On the 6th day after the rat spinal cord injury, the rat’s urine could not be squeezed out by artificial urination. Hematuria was not observed in some rats. Therefore, the bladder function scores of the rats were improved compared with that of day 1. In addition, the bladder weight in SCI groups were significantly increased (p < 0.01) compared with that in control group (Fig. 1D). The weight of bladder increased gradually, and reached the highest at day 7 (0.585 ± 0.026 g).

A The BBB scores were assessed at each time point. B The PVR were measured at each time point. C The UBFS were measured at each time point. D Weights of the bladders were measured at day 1, 4, and 7 after SCI modeling. Data presented as mean ± SD; *p < 0.01.
Identification of activation of autophagy
Next, we detected the expression pattern of TGF-β1 and autophagy markers including LC3 and P62 in bladder tissues from control and SCI rats by immunofluorescence staining. The results showed that TGF-β1 was located in extracellular matrix (Fig. 2A), while LC3 and P62 were located in the cytoplasm (Fig. 2B, C).

A TGF-β1 was located in extracellular matrix. B Punctate LC3 dot-like staining and C punctate P62 dot-like staining were located in the cytoplasm. Red arrow indicated the upregulation of proteins while blue arrow indicated the downregulation of the protein. Scale bar = 50 μM.
TGF-β1 and LC3 and P62 mRNA and protein expression
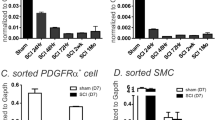
Next, we detected the expression levels of TGF-β1 and autophagy markers including LC3 and P62 in bladder tissues from control and SCI rats by western bolt (Fig. 3A) and qRT-PCR. The corresponding quantitative data of western bolt was shown in Fig. 3B–D. Our results indicated that the protein levels of TGF-β1 and LC3 were increased, while the level of P62 was decreased at day 1, 4 and 7 after SCI modeling. However, the mRNA levels of TGF-β1 were higher in the SCI group than that in the control group at day 1 (p < 0.01) and day 4 (p < 0.05), but there was no statistical difference at day 7 (p > 0.05, Fig. 3E). The mRNA levels of LC3 were increased (Fig. 3F), while the level of P62 was decreased at day 1, 4 and 7 after SCI modeling (Fig. 3G).

A Western blot analysis of TGF-β1, LC3-II and P62 protein expression in the bladder detrusor at day 1, 4, and 7 after SCI modeling in different groups. B–D The corresponding quantitative data of western bolt analysis. E–G qRT-PCR analysis of TGF-β1, LC3-II and P62 protein expression in the bladder detrusor at day 1, 4, and 7 after SCI modeling in different groups. *p < 0.05; **p < 0.01.
Discussion
NLUTD is bladder and urethral disorders caused by damage to the central nervous system that controls voiding function [20]. SCI is the leading cause of neurogenic bladder and urethral disorders [21]. Injury above the conus medullaris and the integrity of the spinal reflex arc of the bladder leads to overactivity of the detrusor and loss of coordinated movement of the detrusor and sphincter, resulting in a spastic bladder [22]. As a result, the patient’s bladder storage and voiding function will be impaired. Injury to the conus or sub-conus causes the loss of integrity of the spinal reflex arc of the bladder and a flaccid bladder [23]. Thus, the patient is able to store urine but cannot voluntarily urinate. The recovery of neurogenic bladder function after SCI is inseparable from long-term and systematic bladder management [24]. Reconstruction of bladder function and improvement of urinary continence are important guarantees for prolonging the life expectancy and improving the quality of life of SCI patients. However, our current understanding of the pathogenesis of LUTD is still very limited, and the molecular regulatory network in the occurrence and development of NLUTD remains unclear.
TGF-β1 is a multifunctional cytokine that regulates cell growth, differentiation, apoptosis and autophagy in various cell types. TGF-β1 protein and activity levels are enhanced acutely during wound healing and chronically in fibrosis to trigger and orchestrate tissue repair processes. It has been reported in the literature that bladder smooth muscle cells release various growth factors in response to mechanical stimulation, such as TGF-β1 and IGF-1 [25]. Previous study has found that TGF-β1 can modulate bladder smooth muscle cell function and may be a crucial regulator of bladder smooth muscle cell phenotype in pathological bladder conditions and also increase the compliance of the bladder [26]. In vitro experiment confirmed that TGF-β1 improve the compliance of bladder smooth muscle cell by increasing soluble collagen production [27]. Some studies have confirmed that TGF-β1 induces autophagy of vascular smooth muscle cells [28].
Autophagy is a highly conservative degradation pathway in eukaryotic organisms, in which cellular proteins, organelles and invading microbes are engulfed by double-membraned autophagosomes and are degraded in the lysosomes [5]. It has great significance in maintaining the stability of the intracellular environment and promoting cell metabolism. Autophagy plays a vital role in the maintenance of homeostasis in bladder smooth muscle cells. Autophagy serves dual roles dependent on the conditions, promoting survival or promoting cell death [5]. Emerging data has suggested that the restoration and/or augmentation of proper autophagy function, for example by inducing lysosomal biogenesis, may be a potential therapeutic target for traumatic brain injury and SCI. In this study, we demonstrated that the bladder muscle of NLUTD rats exhibited a punctated immunostaining pattern for LC3, suggesting the accumulation of autophagosomes. Therefore, anti-autophagy therapy may be a feasible therapeutic strategy for SCI-induced NLUTD. Accumulating evidence has demonstrated that antimalarial drugs, including chloroquine and hydroxychloroquine, are among the very few that inhibit autophagy [29]. Chloroquine and hydroxychloroquine have been widely reported to inhibit autophagy in tumor cells and increase their sensitivity to chemical drugs and radiation [30]. We plan to further examine the therapeutic effect of these antimalarial drugs on NLUTD in our future studies.
In order to explore the roles of TGF-β1 and autophagy in NLUTD, we established a model of NLUTD that was proved to be successful by the results of the BBB score, the PVR and the UBFS. There were differences in BBB score, PVR, UBFS and bladder weight between the SCI group and the control group. The result of the BBB score showed that the motor function of the hindlimb was lost after spinal cord transection injury, and did not recover until the 6th day. The results of the PVR and the UBFS showed that bladder function was impaired after spinal cord transection injury. Then, the decreasing PVR and increasing UBFS indicate that the bladder function was gradually recovering with time. Both the results showed that the recovery of bladder function was prior to the recovery of motor function. We believe that this may be due to the fact that motor regulation relies on a more complex neural network than the voiding reflex.
The results of western blot showed that the SCI rats started to express TGF-β1 and LC3-II at 1 day after SCI, and LC3-II reached a peak at 7 days. The qRT-PCR results showed that the TGF-β1 and LC3-II mRNA level increased as compared to the control group, and reached a peak at 1 day after SCI, at the beginning of the recovery of bladder function. In addition, the expression and mRNA level of P62 was decreased that was consistent with the activation of autophagy in the bladder of SCI rats. These results suggest that the dynamic changes of LC3-II and P62 represent the autophagy activation of NLUTD after SCI. The dynamic change of TGF-β1 is consistent with the trend of autophagy activation in the detrusor of the bladder of SCI rats.
In the acute stage of SCI, the bladder is mostly in the stage of urinary retention. The detrusor is subjected to excessive mechanical traction and release various factors. The results of the present study provide the evidence that as early as 1 day after SCI a number of gene transcripts in the detrusor are significantly altered. In this study, we also found that the bladder weights were increased, which might be a sign of bladder fibrosis. In fact, we expected fibrosis of the bladder wall significantly later than the experimental results (7 days). We believe our findings illustrate the possible role of TGF-β1 in SCI-induced NLUTD. As a well-known biochemical regulator of tissue fibrosis and remodeling, TGF- β1 may also promote the remodeling of bladder wall, suggesting that it has various effects on NLUTD.
Neurogenic lower urinary tract dysfunction caused by SCI above the parasympathetic spinal canter is usually characterized by detrusor overactivity, low bladder compliance and detrusor-sphincter-dyssynergia [31]. Previous studies have focused on the injured nerves innervating the bladder after SCI, but there are few studies on the pathophysiological mechanism of bladder detrusor. In our study, we found that the expression of TGF-β1 in NLUTD detrusor was significantly increased. In addition, the autophagy was activated in the NLUTD detrusor that was consistent with previous studies [10]. The mechanism of autophagy activated by TGF-β1 is still not clear. Are there other signaling pathways involved in the upregulation of autophagy in detrusor after SCI? It will be the target of future research.
Unfortunately, our research still has some shortcomings. Due to the limitation of experimental conditions, we did not perform urodynamic tests, which can more strongly describe the bladder function of rats. We will continue to focus on these issues in future research.
Conclusion
To summarize, this study demonstrates that TGF-β1 and autophagy-related proteins were expressed in different stages of NLUTD, and they might be involved in the pathological process of NLUTD.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Li HL, Xu H, Li YL, Sun SW, Song WY, Wu Q, et al. Epidemiology of traumatic spinal cord injury in Tianjin, China: An 18-year retrospective study of 735 cases. J Spinal Cord Med. 2019;42:778–85.
Taweel WA, Seyam R. Neurogenic bladder in spinal cord injury patients. Res Rep Urol. 2015;7:85–99.
Hajebrahimi S, Chapple CR, Pashazadeh F, Salehi-Pourmehr H. Management of neurogenic bladder in patients with Parkinson’s disease: a systematic review. Neurourol Urodyn. 2019;38:31–62.
Farre JC, Subramani S. Mechanistic insights into selective autophagy pathways: lessons from yeast. Nat Rev Mol Cell Biol. 2016;17:537–52.
Mizushima N, Levine B, Cuervo AM, Klionsky DJ. Autophagy fights disease through cellular self-digestion. Nature. 2008;451:1069–75.
Komatsu M, Waguri S, Koike M, Sou YS, Ueno T, Hara T, et al. Homeostatic levels of p62 control cytoplasmic inclusion body formation in autophagy-deficient mice. Cell. 2007;131:1149–63.
Pankiv S, Clausen TH, Lamark T, Brech A, Bruun JA, Outzen H, et al. p62/SQSTM1 binds directly to Atg8/LC3 to facilitate degradation of ubiquitinated protein aggregates by autophagy. J Biol Chem. 2007;282:24131–45.
Komatsu M, Kageyama S, Ichimura Y. p62/SQSTM1/A170: physiology and pathology. Pharmacol Res. 2012;66:457–62.
Wu J, Lipinski MM. Autophagy in neurotrauma: good, bad, or dysregulated. Cells. 2019;8:693.
Zeng FS, Zhang L, Cui BJ, Huang LG, Zhang Q, Sun M, et al. Expression of autophagy in different stages of neurogenic bladder after spinal cord injury in rats. Spinal Cord. 2017;55:834–9.
Diniz LP, Matias I, Siqueira M, Stipursky J, Gomes FCA. Astrocytes and the TGF-beta1 pathway in the healthy and diseased brain: a double-edged sword. Mol Neurobiol. 2019;56:4653–79.
McLennan IS, Koishi K. The transforming growth factor-betas: multifaceted regulators of the development and maintenance of skeletal muscles, motoneurons and Schwann cells. Int J Dev Biol. 2002;46:559–67.
Hamada Y, Ikata T, Katoh S, Katoh K, Niwa M, Tsutsumishita Y, et al. Effects of exogenous transforming growth factor-beta 1 on spinal cord injury in rats. Neurosci Lett. 1996;203:97–100.
Liang CC, Shaw SS, Ko YS, Huang YH, Lee TH. Effect of amniotic fluid stem cell transplantation on the recovery of bladder dysfunction in spinal cord-injured rats. Sci Rep. 2020;10:10030.
Yang X, Xue P, Liu X, Xu X, Chen Z. HMGB1/autophagy pathway mediates the atrophic effect of TGF-beta1 in denervated skeletal muscle. Cell Commun Signal. 2018;16:97.
Zhao J, Wu M, Chen S, Ji Z, Zheng X. TGF-beta1 and connexin-43 expression in neurogenic bladder from rats with sacral spinal cord injury. Neurourol Urodyn. 2018;37:2502–9.
Lee BB, Cripps RA, Fitzharris M, Wing PC. The global map for traumatic spinal cord injury epidemiology. Spinal Cord. 2014;52:110–6.
Kuricova M, Ledecky V, Liptak T, Madari A, Grulova I LS. Oral administration of inosine promotes recovery after experimental spinal cord injury in rat. Neurol SCI. 2014;35:1785–91.
Gotoh D, Shimizu N, Wada N, Kadekawa K, Saito T, Mizoguchi S, et al. Effects of a new beta3-adrenoceptor agonist, vibegron, on neurogenic bladder dysfunction and remodeling in mice with spinal cord injury. Neurourol Urodyn. 2020;39:2120–7.
Averbeck MA. Editorial comment: systematic literature review and meta-analysis of sacral neuromodulation (SNM) in patients with neurogenic lower urinary tract Dys-function (nLUTD): over 20 years’ experience and fu-ture directions. Int Braz J Urol. 2021;47:1264–5.
Anderson CE, Birkhauser V, Jordan X, Liechti MD, Luca E, Mohr S, et al. Urological management at discharge from acute spinal cord injury rehabilitation: a descriptive analysis from a population-based prospective cohort. Eur Urol Open Sci. 2022;38:1–9.
Dodd W, Motwani K, Small C, Pierre K, Patel D, Malnik S, et al. Spinal cord injury and neurogenic lower urinary tract dysfunction: what do we know and where are we going? J Mens Health. 2022;18:24.
Pannek J, Pannek-Rademacher S. Usefulness of Hydrastis for the prevention of encrustation of long-term indwelling catheters in persons with neurogenic bladder dysfunction: a case series. Spinal Cord Ser Cases. 2021;7:66.
Andretta E, Pagliacci MC, Zuliani C, Filocamo MT, Losavio E, Krassioukov A, et al. A survey of clinical practice concerning long-term follow-up of neurogenic lower urinary tract dysfunction due to spinal cord injury in Italy. J. Spinal Cord Med. 2021:1–9. https://doi.org/10.1080/10790268.2020.1863899.
Nagatomi J, DeMiguel F, Torimoto K, Chancellor MB, Getzenberg RH, Sacks MS, et al. Early molecular-level changes in rat bladder wall tissue following spinal cord injury. Biochem Biophys Res Commun. 2005;334:1159–64.
Parekh A, Long RA, Iannone EC, Chancellor MB, Sacks MS. Assessing the effects of transforming growth factor-beta1 on bladder smooth muscle cell phenotype. I. Modulation of in vitro contractility. J Urol. 2009;182:1210–5.
Heise RL, Parekh A, Joyce EM, Chancellor MB, Sacks MS. Strain history and TGF-beta1 induce urinary bladder wall smooth muscle remodeling and elastogenesis. Biomech Model Mechanobiol. 2012;11:131–45.
Wang W, Chen L, Shang C, Jin Z, Yao F, Bai L, et al. miR-145 inhibits the proliferation and migration of vascular smooth muscle cells by regulating autophagy. J Cell Mol Med. 2020;24:6658–69.
Wang J, Qiu L. Drug-induced self-assembled nanovesicles for doxorubicin resistance reversal via autophagy inhibition and delivery synchronism. Theranostics. 2022;12:3977–94.
De Sanctis JB, Charris J, Blanco Z, Ramirez H, Martinez GP, Mijares MR, et al. Molecular mechanisms of chloroquine and hydroxychloroquine use in cancer therapy. Anticancer Agents Med Chem. 2022. https://doi.org/10.2174/1871520622666220519102948.
Agrawal M, Joshi M. Urodynamic patterns after traumatic spinal cord injury. J Spinal Cord Med. 2015;38:128–33.
Acknowledgements
We would like to thank Professor Huanmin NIU (Department of Rehabilitation Medicine, Second Hospital of Shandong) for providing equipment.
Funding
This work was supported by a grant from the Natural Science Foundation of Shandong Province (ZR2019BH048).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ma, L., Mu, Y., Li, X. et al. Expression of transforming growth factor-β1 and autophagy markers in the bladder of rats with neurogenic lower urinary tract injury. Spinal Cord 61, 154–159 (2023). https://doi.org/10.1038/s41393-022-00866-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-022-00866-y
