
Abstract
Study design
Experimental study.
Objectives
To compare lipid profiles during moderate-intensity exercise between persons with cervical spinal cord injuries (SCIC) and able-bodied controls (AB).
Setting
Wakayama Medical University, Japan.
Methods
Six participants with SCIC and six AB performed 30-min arm-crank exercise at 50% VO2peak. Blood samples were collected before (PRE), immediately (POST), and 60 min after exercise (REC). Concentrations of serum free fatty acids ([FFA]s), total ketone bodies ([tKB]s), acetoacetic acid ([AcAc]s), insulin ([Ins]s), and plasma catecholamines and glucose ([Glc]p) were assessed.
Results
Catecholamine concentrations in SCIC were lower than AB throughout the experiment (P < 0.001) and remained unchanged, while increased at POST in AB (P < 0.01). [FFA]s remained unchanged in both groups with no differences between groups. [tKB]s in SCIC tended to increase at REC from PRE (P = 0.043), while remaining unchanged in AB (P > 0.42). [AcAc]s in SCIC increased at REC from PRE and POST (P < 0.01) while remaining unchanged in AB (interactions of Group × Time P = 0.014). [Glc]p and [Ins]s were comparable between the groups throughout the study.
Conclusion
Serum ketone bodies in SCIC increased after exercise while remaining unchanged in AB, suggesting that suppressed uptakes of serum ketone bodies from blood to the muscles in SCIC would partially contribute the increased serum ketones.
Similar content being viewed by others


Introduction
Daily physical activity in persons with spinal cord injuries (SCI) tends to be restricted due to locomotor deficits, likely increasing the prevalence of diabetes mellitus, dyslipidemia, and metabolic syndrome more than in the able-bodied (AB) population [1]. As reported from Sasakawa Peace Foundation, participation in sport and recreation should be encouraged and promoted, but rates of activity participation in individuals with impairments was still less than 20% in Japan [2]. Accordingly, the identification and development of ideal physical environments to encourage physical activity participation safely in persons with impairments are strongly desired.
Persons with cervical spinal cord injuries (SCIC) face multiple challenges to exercise performance due to both somatic and autonomic dysfunction associated with higher-level SCI [3]. Working muscles are smaller in SCIC athletes and skeletal muscle glycogen stores are likely depleted faster during exercise [4]. In addition, after SCI, there is a shift to type II muscle fibers while the existing type I fibers selectively atrophy [5], further contributing to altered exercise metabolism in this population. Because lipid profiles in persons with SCI are characterized primarily by lower high-density lipoprotein cholesterol (HDL-C) and higher triglyceride/HDL-C ratio than those in AB [6], lipid metabolism is possibly different from AB controls during prolonged exercise. However, there is limited information about fat metabolism that would inform nutritional guidance for exercise performance in SCI.
Free fatty acid (FFA) usage can exceed that of glucose during mild to moderate exercise, leading to increase production of ketone bodies in the liver. Ketone bodies are crucial to metabolic pathways such as β-oxidation, the tricarboxylic acid (TCA) cycle, gluconeogenesis, and lipogenesis [7]. Serum concentrations of ketone bodies are determined by the difference between production in the liver and uptake in peripheral tissues such as skeletal muscles and brain. Sympathetic dysfunction possibly attenuates the production and release of ketone bodies in SCIC, while the smaller muscle mass and decreased oxidative capacity in SCIC can reduce the removal of ketone bodies from the bloodstream [7]. The assessment of serum concentrations of FFA ([FFA]s), respiratory exchange ratio (RER), and serum ketone bodies would deepen our understanding of lipid metabolism in persons with SCIC.
The purpose of our study was to examine serum ketone bodies and [FFA]s before, during, and after exercise in SCIC and compare the responses to normative changes in AB persons. The hypothesis was that serum ketone bodies would be elevated more in SCIC than in AB after exercise.
Methods
Participants
Participants were recruited from the community surrounding Wakayama Medical University. Six males with SCIC volunteered for the study and six AB males were recruited as sex-matched controls. Participants were excluded if they had comorbid other neurological/medical conditions or were taking medications that primarily affected cardiac function. Participants were provided the details of the study protocol and possible risks, and they provided informed written consent form before voluntary participation in this study. The procedures in this study conformed to the guidelines in the Declaration of Helsinki and were approved by the Review Board on Human Experiments, Wakayama Medical University (#2076).
Study protocol
Participants were reported to come to the laboratory for two separate visits for a baseline testing session, as well as an acute exercise trial. Prior to each visit, all participants were asked to refrain from alcohol, caffeine and heavy exercise for 24 h preceding the experiments, as well as fast for at least 4 h before measurements. In the first visit, participants performed an arm-crank-graded exercise test to exhaustion for determining their peak rate of oxygen consumption (VO2peak). After arrival at the laboratory, participants emptied their bladders and body mass was taken on a wheelchair scale (PW-630, TANITA corporation, Tokyo); in participants with SCIC, the mass of their wheelchair was subtracted from the total to calculate body mass. Participants then entered an environmental chamber controlled at 25 °C ambient temperature and 50% relative humidity. Participants rested quietly for 30 min prior to measurements while they were outfitted with equipment. After measurements at rest for 3 min, participants started arm-crank exercise at 50 revolutions/min without loading for 3 min. Since the optimal workload increment for eliciting VO2peak of SCIC using an arm-crank ergometer is 2–6 W min−1 [8], the exercise intensity was increased by 5 W every 3 min until it reached 10 W, and above this intensity, 5 W every minute for persons with SCIC and 10 W for AB every minute until they could not maintain the rhythm due to exhaustion [9]. We assessed minute oxygen consumption (VO2), carbon dioxide elimination (VCO2), and ventilation (VE) every 15 s (MetaMax 3B, CORTEX, Leipzig, Germany) and monitored electrocardiogram continuously during the graded exercise. We determined VO2peak by averaging the three largest consecutive values at the end of exercise [10].
At the second visit, participants emptied their bladders, were weighed, entered the same environmental chamber at the same condition as the first visit, and then rested for 60 min on a wheelchair or a chair for SCIC or AB, respectively, while they were outfitted with measurement equipment. Previously, a hand-ergometer exercise at 60% of VO2peak for 20 min was used as the exercise load for trained SCIC [11], but it was difficult for untrained SCIC in present study to do 20-min exercise at the same load as the above. The participants performed the exercise in two separate sessions because total VO2 and energy expenditure during intermittent aerobic exercise are comparable to continuous exercise with the same intensity and total duration and are greater after exercise [12]. After 10-min resting measurements, participants performed 2 sets of arm-crank exercise for 15 min intermediated by 2 min. They were able to exercise for 30 min, the minimum daily exercise time recommended for SCI to improve their cardiometabolic health [13]. Work intensity was set as 50% VO2peak calculated by the Karvonen formula [14] at 50 revolutions/min, 7 (2) [mean (SD)] and 43 (6) W for SCIC and AB, respectively. After exercise, participants rested in a sitting position for 60 min during de-instrumentation and recovery measurements.
Measurements
Heart rate
A single-lead electrocardiogram (BSM-2401; Nihon Koden, Tokyo) was used to measure heart rate (HR) by averaging R-R intervals every minute during rest and throughout exercise.
Blood samples
Eight milliliters of blood was collected from the antecubital vein via a butterfly needle each at rest (PRE), immediately after the exercise (POST), and 60 min after the exercise (REC). One milliliter of blood was put into sodium-fluoride-containing tubes to assess plasma concentration of glucose ([Glc]p). Three milliliters of blood were placed into EDTA-2Na+-containing tubes to assess plasma concentrations of adrenaline ([Ad]p) and noradrenaline ([NA]p). Four milliliters of blood was transferred to serum-separating medium tubes to assess serum concentrations of insulin ([Ins]s), ketone bodies, acetoacetic acid ([AcAc]s), β-hydroxybutyrate ([βOHB]s) and total ketone bodies ([tKB]s), as well as [FFA]s. All tubes, except those containing heparin, were centrifuged at 4 °C at 3000 rpm for 20 min. Following centrifugation, serum or plasma components were transferred into sterilized tubes. These samples were stored in a −80 °C freezer for later analysis.
Blood properties
[Ad]p and [NA]p were measured by HPLC (model HPLC-725CA; Toso, Tokyo). [AcAc]s, [βOHB]s, [tKB]s and [FFA]s were assessed by enzyme method. [Ins]s was determined by chemiluminescent enzyme immunoassay. [Glc]p was measured using an ultraviolet absorption spectrophotometry.
Data analysis
Cardiorespiratory responses
HR was averaged for 5 min at rest, during the 2-min rest interval, and during the first and last 5 min of each exercise bout.
Group characteristics were compared using independent Student’s t-tests. A 2 × 3 (group × time) repeated-measures ANOVA was used to evaluate all outcome responses. Subsequent post hoc evaluations were performed using a Tukey–Kramer test. All values are presented as means (SD), unless otherwise indicated. The null hypothesis was rejected at the level of P < 0.05. The standard least squares method was used to perform regression analyses between a change (Δ) in [Ad]p versus Δlipid profiles from PRE. All statistical evaluations were performed using SPSS 25.0 (IBM, Chicago, IL). Based on the previous data of [tKB]s and [AcAc]s in SCIC and AB during mild cold stress [15] and assumed that alpha error probability and power (1- β err prob) were 0.05 and 0.85, respectively, the effect size were 0.454 and 0.851 and the total sample sizes were 10 and 6, respectively, using “ANOVA Repeated measures, within factors” of statistical test. Sample sizes in SCI interventional studies tend to be small [16] due to their severe disabilities. Type II errors are more likely to occur when sample sizes are too small. However, statistical power (1- β err prob) for [tKB]s and [AcAc]s in the present study calculated by using the same test as above were both >0.999 and the effect sizes were 2.255 and 3.133, respectively, assuming α error probability was 0.05.
Results
There were no significant differences in any physical characteristics between SCIC and AB, including age [40 (11) vs. 37 (12) years, P = 0.639), self-reported body length [173 (7) vs. 170 (5) cm; P = 0.513) and body mass [58.8 (14.4) vs. 64.8 (12.2) kg; P = 0.459). SCIC participants’ level of injury ranged from C5 to C7, and the duration of injury was 23 (12) years (range 7–39 years). Four SCIC participants were clinically classified as grade A of the American Spinal Injury Association Impairment Scale (AIS A) and the rest were graded as AIS B, all having motor-complete injuries. Maximal power output was 7 (1) W in SCIC, which was lower than that in AB of 43 (3) W (P < 0.0001). Power output during continuous exercise was 7 (2) and 43 (6) W in SCIC and AB, respectively.
Cardiorespiratory responses
HR increased from 61 (8) to 76 (7) bpm in SCIC, and from 69 (7) to 138 (18) in AB (both P < 0.0001; Table 1).
Catecholamines
At all-time points, SCIC had significantly lower [Ad]p and [NA]p than AB (P < 0.007), which remained unchanged during exercise in SCIC (P > 0.6) but was increased at POST in AB compared to PRE (P = 0.037) and REC (P = 0.020; Fig. 1).

Plasma concentrations of adrenaline (A) and noradrenaline (B) before and after exercise in individuals with cervical spinal cord injury and able-bodied. Blood samples were collected before (PRE), immediately after exercise (POST) and 60 min after the cessation of exercise (REC) in 6 individuals with cervical spinal cord injury (●; SCIC) and 6 able-bodied (○; AB). [Ad]p, plasma concentrations of adrenaline; [NA]p, plasma concentrations of noradrenaline. Data are means (SD). *, compared between groups; ‡, from PRE and REC (P < 0.05).
Metabolic markers
Figure 2 shows lipid profiles in both groups. [FFA]s remained unchanged throughout the experiment in both groups (time effect P = 0.212; Fig. 2A) and no significant differences between the groups were observed (group effect P = 0.288). [tKB]s in SCIC tended to increase at REC from PRE (P = 0.082; Fig. 2B), while remaining unchanged in AB (P > 0.42). [AcAc]s in SCIC increased at REC from PRE and POST (P = 0.006 and 0.020, respectively; Fig. 2C), while remaining unchanged in AB (P > 0.42). [βOHB]s remained unchanged in both groups over time (time effect P = 0.083; Fig. 2D) with no differences between groups (P = 0.309) and no Group × Time interaction (P = 0.181).

Serum concentrations of free fatty acids (A), total ketone bodies (B), acetoacetic acid (C) and 3-hydroxybutyric acid (D) before and after exercise in individuals with cervical spinal cord injury and able-bodied. Blood samples were collected before (PRE), immediately after exercise (POST) and 60 min after the cessation of exercise (REC) in 6 individuals with cervical spinal cord injury (●; SCIC) and 6 able-bodied (○; AB). [FFA]s, serum concentrations of free fatty acids; [tKB]s, serum concentrations of total ketone bodies; [AcAc]s, serum concentrations of acetoacetic acid; [βOHB]s, serum concentrations of 3-hydroxybutyric acid. Data are means (SD). †, compared from PRE (P < 0.05).
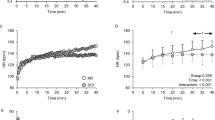
[Glc]p at each time point was similar between the two groups (group effect P = 0.216) and remained unchanged throughout the study in both groups (time effect P = 0.103; Fig. 3A). [Ins]s was comparable between the groups (P = 0.811) and there was no Group × Time interaction (P = 0.839; Fig. 3B), however, it tended to decrease at REC compared with PRE in SCIC (P = 0.068; time effect of ANOVA for P = 0.011), while remaining unchanged in AB (P > 0.170).

Plasma concentrations of glucose (A) and serum concentrations of insulin (B) before and after exercise in individuals with cervical spinal cord injury and able-bodied. Blood samples were collected before (PRE), immediately after exercise (POST) and 60 min after the cessation of exercise (REC) in 6 individuals with cervical spinal cord injury (●; SCIC) and 6 able-bodied (○; AB). [Glc]p, plasma concentrations of glucose; [Ins]s, serum concentrations of insulin. Data are means (SD). †, compared from PRE in AB; ‡, from PRE and POST in SCI (P < 0.05).
Relationships between Δ[Ad]p and lipid profiles
There were no significant correlation between Δ[Ad]p vs. Δ[FFA]s, Δ[AcAc]s, Δ[βOHB]s, and Δ[tKB] (all P > 0.694).
Discussion
The new finding from this study was that serum indicators of lipolysis, [tKB]s and [AcAc]s, tended to be elevated one hour after exercise in SCIC, while [FFA]s and [Glc]p remained unchanged during exercise. The results were not associated with differences in plasma catecholamine concentrations between the groups. Together, these results suggest that the increased [tKB]s after exercise is likely explained by reduced uptake of ketone bodies from the skeletal muscles.
[tKB]s increased after exercise only in SCIC
Endurance activities are associated with increased fat utilization. Triglycerides, stored in adipose tissue and within muscle fibers, are the main source of FFA during exercise [17] and during the first few hours of recovery [18]. The release of FFA into the blood is primarily due to sympathetic nervous activity directed towards the adipocytes [17]. After β-oxidation of FFA in the mitochondria, acetyl-coenzyme A (acetyl-CoA) is provided to the TCA cycle as substrate. Ketone bodies are synthesized in the liver by the condensation of 2 acetyl-CoA molecules, which are then transported to the extrahepatic tissues and used as an energy source in the brain and muscles [17]. [tKB]s is determined by the balance between ketone supply from the liver into the blood and disappearance from blood into peripheral tissues.
Persons with SCIC have muscular atrophy and increased storage of intramuscular fat [19]. Furthermore, accumulation of lipids could interfere with glucose metabolism in skeletal muscles due to reduced sensitivity of insulin receptors [20], resulting in enhanced fat utilization. With respect to the observed increase in serum ketone bodies, higher production of ketones bodies could be considered. However, similar [FFA]s, [Glc]p, and [Ins]s between groups suggest ketone supply was not substantially altered. Thus, it is more likely that there was reduced uptake of ketones bodies from the bloodstream to the muscles in SCIC during and after prolonged exercise, not enhanced production of ketones bodies. If RER is lower in SCIC than in AB, this idea would be supported (see Supplementary Appendix for metabolic responses). Additional studies are needed to study the time course of changes immediately post-exercise, and whether similar results would be expected under different exercise conditions; for example, under long-duration exercise with glycogen depletion or with different nutritional strategies before and after exercise in SCIC.
Ketones are critical energy sources in the peripheral tissues, and act as the substrates of lipolysis during non-glycolytic aerobic metabolism. MCT1 and MCT2 transporters control the uptake of ketones and are expressed in the skeletal muscles, heart, brain, muscle, and kidney [7]. Skeletal muscle tissues are a primary location for ketone uptake in AB persons, but individuals with SCIC have drastically less muscle mass in which to uptake ketone bodies from the blood [21]. Muscle atrophy and selective transformation from type I to type II fibers in paralyzed areas [5] would further disadvantage ketone use as an energy source, as ketone usage is related with mitochondrial volume [22], which is larger in non-atrophied type I muscle fibers. Although it is possible the production of ketones was enhanced in SCIC compared with AB, the actual usage of ketone bodies in the peripheral tissues may not be augmented, leading to our observation of [tKB]s in the blood.
Insulin inhibits lipolysis, gluconeogenesis, and glycogenolysis in the liver. In the present study, the decrease in [Ins]s following exercise in both groups suggests that lipolysis would be enhanced after exercise, although this would not solely account for the increase in serum ketones in SCIC. Previous studies have suggested that insulin sensitivity itself decreased in SCIC compared with paraplegia [23] and AB persons [24]. As a result, decreased insulin sensitivity could lead to secondary increases in lipid metabolism to overcome an energy deficit during exercise in SCIC [25]. While this is an attractive theory, the change in plasma glucose was also similar between groups in the present study, suggesting trivial differences in insulin sensitivity.
Finally, one other potential mechanism for increased post-exercise [tKB]s is negative energy balance secondary to SCIC. In a negative energy balance state, the central nervous system and red blood cells have priority use of glucose because they almost entirely dependent on glucose metabolism. However, as other tissues can rely on fat metabolism, the liver increases synthesis of ketone bodies to supply fuel to tissues that can use substrate other than glucose, such as skeletal muscle [26]. Nutritional health after SCIC varies widely, with previous reports indicating 40–50% of SCIC patients admitted to hospitals were at risk of nutritional deficiency, including up to 12% who were severely malnourished. At the opposite end of the spectrum, there are also individuals who suffer from obesity due to high energy intake, which likely exceeds energy expenditure [27]. In the present study, body weight in persons with SCIC was comparable to AB. The influences of the negative energy balance would be minor in the study.
Increasing [FFA]s after exercise in SCIC
In general, catabolic processes (i.e., glycolysis, gluconeogenesis and lipolysis) are activated by catecholamines. Venous infusion of catecholamines has been shown to increase [Glc]p and [FFA]s in healthy subjects [28]. However, catecholamines do not seem to influence glucose and lipid profiles during and after endurance exercise in SCIC, given the lack of correlation in the present study. A previous study using the microdialysis technique in healthy participants revealed that lipolysis in the abdominal subcutaneous adipose tissue was stimulated by phentolamine (an α-adrenergic inhibitor) during 120-min rest, while in contrast, lipolysis was attenuated by propranolol (a β-adrenergic blocker) during 30-min exercise [29]. In the present study, energy expenditure in exercising SCIC was lower than in AB, because the low absolute workload was ~5 W. However, the increase in [FFA]s after exercise was comparable to AB. Mechanisms of lipolysis in SCIC would not be related with sympathoexcitation, which does not occur in the SCIC group.
Limitations
Finally, we have to mention some limitations of the study. First, although the statistical powers of the ketones were relatively high enough to guarantee minimum effects of type II error, the sample size was small. So, the preliminary results of the present study may help the future research plans. Even the exercise load performed in this study wearing the measurement devices was a hurdle for SCIC who do not have an exercise routine, because of their multiple disabilities. Unfortunately, metabolic responses could only be assessed for just 3 persons with SCIC and there may be low power to detect differences in some biomarkers. These data were presented as supplementary files. Direct metabolic markers (outside serum and plasma) immediately after exercise were not measured. For instance, lactate is a metabolic by-product of glycolysis and is also produced by glycogenolysis. We did not evaluate intramuscular glycogen content. Muscle biopsies or non-invasive magnetic resonance spectroscopy are established procedures for measuring metabolic activity inside the muscle, but we are unable to conduct these procedures in our laboratory. Although there was no a priory hypothesis for a sex difference, only men participated in this study. This is reflective of the sex distribution of our rehabilitation program. It has been reported that there are sex differences in lipid metabolism in able-bodied individuals [30], and the results of this study may not apply to women with SCIC.
Conclusion
Serum concentrations of ketone bodies increased after exercise only in SCIC, with unchanged [FFA]s and [Glc]p. Reduced utilization of ketones as an energy substrate during endurance exercise in SCIC may be due to less active skeletal muscle mass. The present results will provide constructive information to establish a strategy of nutritional promotion before and after exercise in SCIC, for example, matching glucose intake for exercise intensity during and after exercise in persons with SCIC. Future work is warranted to better understand fat metabolism during prolonged exercise in persons with SCIC, as well as best methods to incorporate this knowledge into nutritional recommendations to improve exercise performance.
Data availability
The dataset generated and analyzed during the current study is available from the corresponding author upon reasonable request.
References
Yekutiel M, Brooks ME, Ohry A, Yarom J, Carel R. The prevalence of hypertension, ischaemic heart disease and diabetes in traumatic spinal cord injured patients and amputees. Paraplegia. 1989;27:58–62.
Office of Sports Promotion for the Disabled, Health and Sports Division, Japan Sports Agency. Report on "Project for the Promotion of Sports for Persons with Disabilities in Local Communities (Survey and Research on the Promotion of Sports Participation by Persons with Disabilities). Sasakawa Sports Foundation, Tokyo, 2018. (In Japanese).
Guttmann L, Silver J, Wyndham CH. Thermoregulation in spinal man. J Physiol. 1958;142:406–19.
Kjaer M, Dela F, Sørensen FB, Secher NH, Bangsbo J, Mohr T, et al. Fatty acid kinetics and carbohydrate metabolism during electrical exercise in spinal cord-injured humans. Am J Physiol Regul Integr Comp Physiol. 2001;281:R1492–8.
Burnham R, Martin T, Stein R, Bell G, MacLean I, Steadward R. Skeletal muscle fibre type transformation following spinal cord injury. Spinal Cord. 1997;35:86–91.
Gilbert O, Croffoot JR, Taylor AJ, Nash M, Schomer K, Groah S. Serum lipid concentrations among persons with spinal cord injury - a systematic review and meta-analysis of the literature. Atherosclerosis. 2014;232:305–12.
Puchalska P, Crawford PA. Multi-dimensional roles of ketone bodies in fuel metabolism, signaling, and therapeutics. Cell Metab. 2017;25:262–84.
Lasko-McCarthey P, Davis JA. Protocol dependency of VO2max during arm cycle ergometry in males with quadriplegia. Med Sci Sports Exerc. 1991;23:1097–101.
Sato C, Kamijo YI, Sakurai Y, Araki S, Sakata Y, Ishigame A, et al. Three-week exercise and protein intake immediately after exercise increases the 6-min walking distance with simultaneously improved plasma volume in patients with chronic cerebrovascular disease: a preliminary prospective study. BMC Sports Sci Med Rehabil. 2022;14:38.
Kamijo Y, Takeno Y, Sakai A, Inaki M, Okumoto T, Itoh J, et al. Plasma lactate concentration and muscle blood flow during dynamic exercise with negative-pressure breathing. J Appl Physiol. 2000;89:2196–205.
Kouda K, Furusawa K, Sugiyama H, Sumiya T, Ito T, Tajima F, et al. Does 20-min arm crank ergometer exercise increase plasma interleukin-6 in individuals with cervical spinal cord injury? Eur J Appl Physiol. 2012;112:597–604.
Han I, Mukaimoto T, Ueda H, Kiyota H, Ohno M. Effects of intermittent bouts of aerobic exercise on oxygen consumption during and after exercise. NSSU J Sport Sci. 2012;1:1–7.
Martin Ginis KA, van der Scheer JW, Latimer-Cheung AE, Barrow A, Bourne C, Carruthers P, et al. Evidence-based scientific exercise guidelines for adults with spinal cord injury: an update and a new guideline. Spinal Cord. 2018;56:308–21.
Karvonen MJ, Kentala E, Mustala O. The effects of training on heart rate: a longitudinal study. Ann Med Exp Biol Fenn. 1957;35:307–15.
Nishiyama K, Kamijo YI, van der Scheer JW, Kinoshita T, Goosey-Tolfrey VL, Hoekstra SP, et al. Lipid metabolism after mild cold stress in persons with a cervical spinal cord injury. Spinal Cord. 2022. https://doi.org/10.1038/s41393-022-00788-9.
Zimmermann G, Bolter LM, Sluka R, Höller Y, Bathke AC, Thomschewski A, et al. Sample sizes and statistical methods in interventional studies on individuals with spinal cord injury: a systematic review. J Evid Based Med. 2019;12:200–8.
Ranallo RF, Rhodes EC. Lipid metabolism during exercise. Sports Med. 1998;26:29–42.
Kimber NE, Heigenhauser GJF, Spriet LL, Dyck DJ. Skeletal muscle fat and carbohydrate metabolism during recovery from glycogen-depleting exercise in humans. J Physiol. 2003;548:919–27.
Gorgey AS, Dudley GA. Skeletal muscle atrophy and increased intramuscular fat after incomplete spinal cord injury. Spinal Cord. 2007;45:304–9.
Elder CP, Apple DF, Bickel CS, Meyer RA, Dudley GA. Intramuscular fat and glucose tolerance after spinal cord injury –a cross-sectional study. Spinal Cord. 2004;42:711–6.
Shah PK, Stevens JE, Gregory CM, Pathare NC, Jayaraman A, Bickel SC, et al. Lower-extremity muscle cross-sectional area after incomplete spinal cord injury. Arch Phys Med Rehabil. 2006;87:772–8.
Grabacka M, Pierzchalska M, Dean M, Reiss K. Regulation of ketone body metabolism and the role of PPARα. Int J Mol Sci. 2016;17:2093.
Bauman WA, Adkins RH, Spungen AM, Waters RL. The effect of residual neurological deficit on oral glucose tolerance in persons with chronic spinal cord injury. Spinal Cord. 1999;37:765–71.
Karlsson AK. Insulin resistance and sympathetic function in high spinal cord injury. Spinal Cord. 1999;37:494–500.
Bluvshtein V, Korczyn AD, Pinhas I, Vered Y, Gelernter I, Catz A. Insulin resistance in tetraplegia but not in mid-thoracic paraplegia: is the mid-thoracic spinal cord involved in glucose regulation? Spinal Cord. 2011;49:648–52.
Rodwell VW, Bender DA, Botham KM, et al. Overview of metabolism & the provision of metabolic fuels. In: Harper’s illustrated biochemistry. New York: McGraw-Hill Medical; 2015. p. 139–51.
Dionyssiotis Y. Malnutrition in spinal cord injury: more than nutritional deficiency. J Clin Med Res. 2012;4:227–36.
Macdonald IA, Bennett T, Fellows IW. Catecholamines and the control of metabolism in man. Clin Sci. 1985;68:613–9.
Arner P, Kriegholm E, Engfeldt P, Bolinder J. Adrenergic regulation of lipolysis in situ at rest and during exercise. J Clin Investig. 1990;85:893–8.
Palmisano BT, Zhu L, Eckel RH, Stafford JM. Sex differences in lipid and lipoprotein metabolism. Mol Metab. 2018;15:45–55.
Acknowledgements
We thank all participants for their cooperation in our study. We also appreciate the service of Dr. Sven Hoekstra, Ph.D. from Loughborough University for kindly editing this manuscript. Grants: Mitacs-Japan Society for the Promotion of Science (JSPS) Internship program in 2017 (FT as host supervisor to JA).
Funding
This study was supported by grants from Nachikatsuura Research Foundation (L1221) to FT and also supported by funding from the Japan Society for the Promotion of Science through JSPS Postdoctoral Fellowships for Research in Japan (Summer Program; ID# SP17401; 2017).
Author information
Authors and Affiliations
Contributions
KN, Y-iK, YN, and FT conceived and designed research; KN, Y-iK, JSA, TM, YM, YU, KK, and TO performed the experiments; KN and Y-iK analyzed the data; KN, Y-iK, JSA, YN, and FT interpreted the results; KN prepared the figures; KN and Y-iK drafted the manuscript; all authors edited and revised the manuscript; all authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics
The study protocol and the methods applied in this study conformed to the guidelines of the Declaration of Helsinki and were approved by the Review Board on Human Experiments, Wakayama Medical University.
Informed consent
Informed consent for inclusion in this study was obtained from the participants.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Nishiyama, K., Nishimuara, Y., Au, J.S. et al. Serum concentrations of ketones increase after hand-ergometer exercise in persons with cervical spinal cord injuries: a preliminary prospective study. Spinal Cord 61, 139–144 (2023). https://doi.org/10.1038/s41393-022-00859-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-022-00859-x
