
Abstract
Study design
Cross-sectional study.
Objective
To document the labour market participation rate and investigate the impact of social and economic characteristics on this outcome among individuals with spinal cord injury or disease (SCI/D) who participated in a multidisciplinary rehabilitation programme in Brazil.
Setting
A specialised rehabilitation centre in southern Brazil.
Methods
An interview was performed with former rehabilitation clients with SCI/D. A total of 111 community-dwelling individuals with SCI/D who had been previously rehabilitated in a large regional rehabilitation centre were considered. Employment status and demographic, injury, work, and economic characteristics were self-reported via interview. Descriptive statistical analyses were performed.
Results
The labour market participation rate was 21.6% (24 individuals). Five respondents were employed in formal work activities, and the other 19 were involved in informal activities (self-employed). Since the onset of injury, a shorter time was associated with nonparticipation in occupational work. Individuals with a higher level of education were more likely to be working. Household income was higher among the participants who had returned to work than among those who had not returned.
Conclusion
There is a relatively low labour market participation rate among rehabilitated individuals with SCI/D in southern Brazil. The rehabilitation services should emphasise vocational training, access to education, and employment support for individuals with SCI/D from early onset after the injury. Public policies must be revised to support labour market participation among individuals with SCI/D in Brazil.
Similar content being viewed by others

Introduction
Spinal cord injury or disease (SCI/D) is a health condition associated with drastic life changes with low prevalence and high cost. Every year, ~500,000 individuals worldwide are victimised by SCI/D [1]. The injury causes devastating physical disabilities that may lead to secondary health conditions, activity limitations and participation restrictions that negatively impact the quality of life [2,3,4,5]. Therefore, SCI/D rehabilitation should include disability recovery/management and community reintegration, including social and occupational aspects of life.
Participation in daily occupational activities, including employment, is critical for health and wellbeing [6]. For individuals with disabilities, including those with SCI/D, working can provide more than money to support a particular lifestyle; it can also give a sense of identity, social connections and life motivation [7, 8]. Although employment has been positively associated with quality of life [3], a low return to work rate has been shown among individuals with SCI/D, especially in low-income countries [9,10,11].
In individuals with SCI/D, the return to work process involves negotiating uncertain everyday life situations, including physical and attitudinal barriers [9, 12]. Several factors associated with employment following SCI/D have been described in the literature as determinants, such as age at the injury, time since injury, impairment/functional status, education and training degrees, receiving social and environmental support, and rehabilitation-related factors [9, 13,14,15,16,17,18]. However, there is scarce information about employment among Brazilian individuals with SCI/D.
In Brazil, support for participation in the working life of individuals with disabilities is stated in the Brazilian inclusion law of individuals with disabilities (Law 13.146/2015) in the Statute of Individuals with Disabilities [19], which includes individuals with SCI/D. This law affirmed the autonomy and capacity of these citizens to carry out acts of civil life in conditions of equality with other individuals. Although it represents a tremendous recent legal advance in social inclusion in Brazil, the employment rates among individuals with disabilities are meagre. According to the Brazilian Institute of Geography and Statistics, ~45 million people, which corresponds to almost 24% of Brazilians, have some disability [20]. However, only 403,255, <1%, are employed. Additionally, previous surveys on employment among individuals with SCI in Brazil report very low employment rates (14–15%), especially in the southeastern region [21, 22].
To increase participation rates among individuals with disabilities, the factors beyond the legal aspects involved in working life, primarily socioeconomic and health condition-related aspects, need to be better understood. Therefore, this study aimed to examine the labour market participation of former rehabilitation clients living with SCI and its association with sociodemographic, economic, and injury-related characteristics in the southern region of Brazil.
Methods
Design
This descriptive cross-sectional study was conducted using interviews with individuals with SCI/D who participated in a rehabilitation programme at a local specialised rehabilitation centre (Centro Catarinense de Reabilitação, Florianópolis, SC, Brazil) over the last 25 years. Data collection took place from October 2019 to January 2020. Participants in working age at the onset of data collection in 2019 (i.e., in Brazil 18–64 years for men and 18–59 years for women) were included in the study analysis. The study was conducted according to the Declaration of Helsinki and covered by Universidade Federal de Santa Catarina (24149619.0.0000.0121). Participants signed a written informed consent form before participation.
Participants and procedures
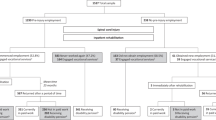
One hundred eleven adult individuals who fulfilled the eligibility criteria participated in this study. They were (1) residents of Santa Catarina State (SC, Brazil), (2) over employable age in Brazil, (3) formally diagnosed with SCI (traumatic or non-traumatic), and (4) had already been enroled in the local outpatient Neurological Rehabilitation Program after injury. Individuals were ineligible for the study if the researcher team identified cognitive or communication problems in the medical record that precluded the interview or if they could not be reached after three phone calls on alternate days and times. In the first step, the head of the Nursing Service screened the available clinical registry of the central data bank (physical and electronic files) from 1996 to January 2020 and selected 254 potential individuals to participate in the study.
The selected potential participants were contacted through phone calls. They were informed of the objectives, confidentiality and voluntary nature of participation in the study, and those who gave consent were interviewed. One hundred and twenty individuals were not reached by the phone contact registered in the medical record; eight had died, four did not meet the inclusion criteria, and one chose not to participate. The eligible participants underwent a structured interview to collect sociodemographic and economic data. A face-to-face interview was performed for 55 participants who could schedule an interview. The interviews were conducted by phone at previously agreed times for the other participants who could not attend. Clinical injury data information was collected from rehabilitation centre medical registries of the individuals. A trained research team performed all procedures.
Labour market participation was the main topic of interest in our study and was defined as involvement in a remunerative work activity. The participants who had remunerative work activity were allocated to employment status: employed or self-employed. Employed individuals worked in typical scenarios with a regular work contract (full-time or part-time). On the other hand, self-employed status means that the person does not have a formal agreement or an employee. Most of the self-employment activities are performed in the informal economy (a sector of the economy that is not taxed or monitored by the government). Participants were asked to select their current occupational situation from a list: working (yes/no), if yes, employed or self-employed; student; or retired (receiving a government disability benefit) before the SCI and at the onset of the study. Moreover, information about personal income, household income adequacy, years of education and marital status was also collected. These are specific and straightforward questions chosen by the researcher to answer the questions of this study. The other clinical data were collected from the clinical discharge registry of the Rehabilitation Centre data bank.
Data analysis
Descriptive statistical analyses were performed using IBM SPSS Statistics (Version 25.0). The proportions of aetiology, origin, marital status, and sex were described to identify the participants. Differences among the continuous variables age, time since injury, years of education, and personal and household income distributions between participants who had occupational work (yes/no) and between the employment status of the working participants (employed or self-employed) were analysed using the Mann–Whitney nonparametric test. Categorical variables were associated with occupational work status (yes/no) and with the employment status of the working participants (employed or self-employed) using the chi-square test. To further determine which variable categories were independently associated with the binomial variables “occupational work status” and “employment status”, binomial logistic regression analysis was performed using these dependent variables and the variables that had previously shown a p ≤ 0.05 in the chi-square analysis. Odds ratios and their 95% confidence intervals were recorded for each level of the independent variables. We chose one level of each dependent variable as a reference group to allow the most salient interpretation of the results. The level of significance adopted was p ≤ 0.05 for all analyses. For the chi-square and binomial logistic regression analyses, the years of education were categorised into education levels based on the International Standard Classification of Education (ISCED) [23]. Categorical variables are represented by absolute and relative frequencies. Continuous variables are reported as the mean and standard deviation or median and interquartile interval.
Results
Participant and injury characteristics
One hundred and eleven individuals with SCI participated in this study. The median age at the beginning of the study was 39 years and ranged from 20 to 63 years old. Most participants were male (76.6%). Overall, the median age at onset of injury was 30 years. The mean age was 29 years among individuals with traumatic injuries and 38 years among individuals with non-traumatic injuries.
Most of the participants had sustained a traumatic SCI (82%) after a motorcycle accident (27.0%) and had their injury classified as AIS-A (61.3%). In non-traumatic SCI, the most common aetiology was compressive myelopathies (7.2%). The mean time since injury was 8 years (SD = 5.5), and most individuals had been injured for less than 6 years (42.3%) at the onset of the study. Table 1 shows the main SCI characteristics among the participants of the study.
Social and economic characteristics
Fifty-six participants (50.5%) were married or were in a stable relationship (civil partnership in Brazil) at the onset of the study. Slightly more than half of the participants (54.1%) were residents of the country regions of the State (Estado de Santa Catarina; Brazil). The participants had a median education time of 9 years (ranging from 1 to 18 years). Moreover, the median monthly income was BRL 1344.50 (USD 341.24) for personal income and BRL 2500.00 (USD 634.50) for household income (respectively 135% and 250% of the minimum wage in Brazil in 2019; i.e., BRL 998.00). A median of three people was financially dependent on the participant’s personal income (other householder members who lived from the participant’s monthly income). Table 2 shows the social and economic characteristics of the study participants.
Overview of occupational characteristics
Before SCI, 108 individuals (97.3%) reported involvement in work activities (labour participation). Of these, 82 individuals (75.9%) were employed in formal work activities. At the onset of the study (after the injury), only 24 individuals (21.6%) reported involvement in the labour market. Of these, 5 were employed in formal work activities, and the other 19 individuals were self-employed. Most individuals (93.7%) retired for disability after the injury. However, some reported that they were retired at the time of the study (disability benefit/retirement) but had informal work activities (self-employed). The median time since the injury was 6 years (2–30).
Impact of the individual’s characteristics on labour market participation
The time of injury, education years, and household income were higher among participants with occupational work activity (p ≤ 0.02; Table 3). Moreover, education years and household income were higher among employed workers than self-employed workers (p ≤ 0.02; Table 3). Age and personal income did not show significant differences among comparisons.
Furthermore, time since injury and education level (ISCED) are associated with having or not having an occupational work activity (p ≤ 0.05; Table 3). Compared with participants with <5 years of SCI, those with time since the injury of 6 to 10 years and more than 10 years were 3.4 and 3.8 times more likely to have occupational work activity (p ≤ 0.03; Table 4). Despite ISCED levels 2 and 3 being at least 5.3 times more likely to have occupational work activity than level 1, the analysis did not reach a statistical significance level (Table 4). Moreover, sex and classification were not associated with labour participation (Table 3).
Discussion
Individuals with SCI/D usually undergo extensive multidisciplinary rehabilitation to optimise participation in the community. Although occupational employment is an essential aspect of life, little attention is given to this aspect in general rehabilitation programmes. Generally, these rehabilitation programmes mainly focus on physical rehabilitation, psychological support, assistive technology exploration, and caregiver support. This study shows a relatively low labour market participation rate (21.6%) in rehabilitated individuals with SCI/D in southern Brazil, and overall, work participation has occurred primarily in a self-employed manner. Time since the onset of injury, between 1 and 5 years, was associated with nonwork activity involvement. Participants with more than 6 years of injury were at least three times more likely to have occupational work activity than those under 5 years. Furthermore, participants with more than 7 years of education (ISCED levels 2 and 3) were approximately five times more likely to have occupational work activity than those under 6 years.
Although there is substantial variability among countries, labour market participation among the participants of our study is lower than the average worldwide rates, typically between 30–40% [10, 11, 21]. Unlike other countries, Brazil has few data regarding employment among individuals with SCI/D. A recent international survey reported a very low employment rate of 14% in individuals with SCI/D in the southeastern region of Brazil [21]. Since Brazil is a large country, it is not surprising that different areas can present significant differences in working status in this population. If, on the one hand, the large size of Brazil promotes a tremendous and rich cultural diversity, it also leads to substantial socioeconomic problems on the other hand. Krause et al. [13] showed differences related to the geographic area in employment among individuals with SCI/D in the United States, and the authors reported that participants in the Midwest showed a greater employment status (50%) than southeastern participants (26%). Moreover, when controlling for other variable predictors, such as years of education, geographic location was not significantly related to employment status. This information reinforces that socioeconomic area status is one of those sociodemographic factors that can promote significant differences in labour market participation among individuals with SCI/D, even in different regions of the same country.
Additionally, most of the participants in our study (93.7%) retired for disability after the injury. This social assistance may promote low labour market participation rates after the onset of SCI/D, especially for employment at formal work. Our results show that only five of the 24 individuals who returned to work were employed. The others were self-employed. Previous studies have shown that disability benefits are negatively related to formal employment after injury, especially in low-income countries [16, 24]. In reviewing the critical factors related to the work participation of individuals with SCI/D, fear of losing financial and medical benefits has been reported as a barrier to returning to work [9, 25]. Considering these previous data, we hypothesise that the high disability retirement/benefit rate may explain our low rate of work labour participation, especially in employment with formal contracts. Self-employment allows individuals to execute some remunerated work activity in the informal market without registration to complement income and maintain their disability benefits.
Since SCI/D is a clinical condition that can cause severe and permanent disabilities, the Brazilian Social Security System provides a disability retirement/benefit for individuals with SCI/D. However, this disability benefit has the same value as the minimum wage in Brazil. In 2019, it was BRL 998.00 (~USD 253.29). This wage is lower than the minimum wage necessary considering the price of basic food set in Brazil in 2019 (BRL 4342.57; ~USD 1102.15) [26]. It is reasonable to think that this promotes an insufficient income among the benefited people, leaving them to supplement their income in a self-employed manner to maintain the benefits.
Among the individual characteristics in our study, time since SCI/D and years of education were associated with labour participation. The time since injury and years of education were higher in working participants. Additionally, a shorter time since the injury (up to 5 years) and education level were associated with a nonwork participation status. A review of the return to work in individuals with SCI/D showed that employment rates improved over time since the onset of injury [9]. Additionally, lack of education or training years are commonly reported barriers to social participation, including employment after SCI/D [9, 13, 14].
Although a previous study reported that younger individuals with SCI/D who sustained paraplegia are more likely to be employed than those with a tetraplegia disability [13], our results do not show an association between these features and return to work. However, we had few participants with tetraplegia (21.6%), which may challenge the generalisability/representativity of our findings. The sample limitation also might have affected the results regarding the age of the participants. Although without reaching the established significance level, our results show a statistical tendency for employed participants to be younger than self-employed (Table 3). On the other hand, a recent study showed that sociodemographic characteristics were more notably associated with participation than were SCI/D characteristics [15]. Additionally, household income was higher among the working participants than those not working in our study. Working as the main activity and higher family incomes have been associated with higher scores on participation and quality of life [15]. This reinforces the importance of rehabilitation programmes inserting vocational rehabilitation into their general programmes. Rehabilitation professionals must find creative ways to identify and neutralise barriers to employment among individuals with SCI/D. This means that programmes need a vocational rehabilitation specialist on the rehabilitation team [27, 28].
Limitations
While this study focuses on labour market participation and related factors among individuals with SCI/D in Brazil, its data may not represent the Brazilian population. Brazil is a country with large continental dimensions and significant variation in its sociodemographic profile. Our study included only a sample of rehabilitated individuals with SCI/D in the southern region of Brazil. Thus, our results may be translated to other Brazilian states or other countries with similar economic characteristics. Notably, the southern state of Santa Catarina has an estimated population of seven million habitants and a very high Human Development Index (HDI, 0.808). This HDI is similar to developed countries and the third major among the 27 Brazilian states [29, 30].
Additionally, this study does not report knowledge on employment trajectories (times of employment and unemployment) after discharge from rehabilitation. Future research should address this employment trajectory, including the return-to-work trajectory. Overall, the sample size and low recruitment rate may have influenced the analysis and limited some interpretations of the results of the study.
Conclusions
There is relatively low labour market participation in rehabilitated individuals with SCI/D in southern Brazil, mainly employed workers. Overall, work participation occurred primarily in a self-employed manner to supplement household income. Moreover, the time since injury and years of education were higher in worker participants. This shows that the more individuals adapt to living with SCI/D and the higher their levels of education are, the more likely they are to participate in the labour market.
Clinical implications
Future enhancements in rehabilitation services should emphasise vocational training, access to education, and employment support for individuals with SCI/D. Additionally, these results reveal a need to revise public policies to support labour market participation among individuals with SCI/D in Brazil.
Data availability
The data will be available from the corresponding author upon reasonable request.
References
WHO, ISCoS. International perspectives on spinal cord injury. In: Bickenbach J, Officer A, Shakespeare T, von Groote P, WHO, ISCoS, editors. WHO, ISCoS; WHO Press, Geneva, 2013.
Khorasanizadeh MH, Yousefifard M, Eskian M, Lu Y, Chalangari M, Harrop JS, et al. Neurological recovery following traumatic spinal cord injury: a systematic review and meta-analysis. J Neurosurg Spine. 2019;30:683–99.
Sturm C, Gutenbrunner CM, Egen C, Geng V, Lemhöfer C, Kalke YB, et al. Which factors have an association to the quality of life (QoL) of people with acquired spinal cord injury (SCI)? A cross-sectional explorative observational study. Spinal Cord. 2021;59:925–32.
Sturm C, Bökel A, Korallus C, Geng V, Kalke YB, Abel R, et al. Promoting factors and barriers to participation in working life for people with spinal cord injury. J Occup Med Toxicol. 2020;15:1–12.
Craig A, Nicholson Perry K, Guest R, Tran Y, Middleton J. Adjustment following chronic spinal cord injury: determining factors that contribute to social participation. Br J Health Psychol. 2015;20:807–23.
Modini M, Joyce S, Mykletun A, Christensen H, Bryant RA, Mitchell PB, et al. The mental health benefits of employment: results of a systematic meta-review. Australas Psychiatry. 2016;24:331–6.
Reed KS, Meade MA, Krause JS. Impact of health behaviors and health management on employment after SCI: psychological health and health management. Top Spinal Cord Inj Rehabil. 2016;22:111–20.
Meade M, Reed K, Saunders L, Krause J. It’s all of the above: benefits of working for individuals with spinal cord injury. Top Spinal Cord Inj Rehabil. 2015;21:1–9.
Lidal IB, Huynh TK, Biering-Sørensen F. Return to work following spinal cord injury: a review. Disabil Rehabil. 2007;29:1341–75.
Young AE, Murphy GC. Employment status after spinal cord injury (1992–2005): a review with implications for interpretation, evaluation, further research, and clinical practice. Int J Rehabil Res. 2009;32:1–11.
Bloom J, Dorsett P, McLennan V. Investigating employment following spinal cord injury: outcomes, methods, and population demographics. Disabil Rehabil. 2019;41:2359–68.
Hilton G, Unsworth C, Murphy G. The experience of attempting to return to work following spinal cord injury: a systematic review of the qualitative literature. Disabil Rehabil. 2018;40:1745–53.
Krause JS, Sternberg M, Maides J, Lottes S. Employment after spinal cord injury: differences related to geographic region, gender, and race. Arch Phys Med Rehabil. 1998;79:615–24.
Gross-Hemmi MH, Post MWM, Bienert S, Chamberlain JD, Hug K, Jordan X, et al. Participation in people living with spinal cord injury in Switzerland: degree and associated factors. Arch Phys Med Rehabil. 2019;100:1894–906.
Halvorsen A, Pape K, Post MWM, Biering-Sørensen F, Mikalsen S, Hansen AN, et al. Participation and quality of life in persons living with spinal cord injury in Norway. J Rehabil Med. 2021;53:jrm00217.
Ramakrishnan K, Chung TY, Hasnan N, Abdullah SJF. Return to work after spinal cord injury in Malaysia. Spinal Cord. 2011;49:812–6.
Kee KM, Mohamad NZ, Koh PPW, Yeo JPT, Ng YS, Kam JC, et al. Return to work after spinal cord injury: a Singaporean pilot community-based rehabilitation program. Spinal Cord. 2020;58:1096–103.
Roels EH, Reneman MF, New PW, Kiekens C, Van Roey L, Townson A, et al. International comparison of vocational rehabilitation for persons with spinal cord injury: Systems, practices, and barriers. Top Spinal Cord Inj Rehabil. 2020;26:21–35.
Brasil. Lei Brasileira de Inclusão da Pessoa com Deficiência. Estatuto da Pessoa com Deficiência; 2015.
IBGE. Sinopse do Censo 2010. Rio de Janeiro: Inst. Bras. Geogr. e Estatística—IBGE; 2011.
Post MWM, Reinhardt JD, Avellanet M, Escorpizo R, Engkasan JP, Schwegler U, et al. Employment among people with spinal cord injury in 22 countries across the world: results from the International Spinal Cord Injury Community Survey. Arch Phys Med Rehabil. 2020;101:2157–66.
Faleiros F, Marcossi M, Ribeiro O, Tholl A, Freitas G, Ribeiro M, et al. Epidemiological profile of spinal cord injury in Brazil. J Spinal Cord Med. 2022:1–8.
UNESCO. International Standard Classification of Education: ISCED 2011. Montreal: UNESCO Institute for Statistics; 2012.
Jang Y, Wang YH, Wang JD. Return to work after spinal cord injury in Taiwan: the contribution of functional independence. Spinal Cord. 2000;38:51–5.
Ottomanelli L, Lind L. Review of critical factors related to employment after spinal cord injury: implications for research and vocational services. J Spinal Cord Med. 2009;32:503–31.
DIEESE. Pesquisa nacional da Cesta Básica—Salário mínimo nominal e necessário [Internet]. Dep. Intersind. Estatísticas e Estud. Socioeconômicos—DIEESE; 2022. https://www.dieese.org.br/analisecestabasica/salarioMinimo.html.
Ottomanelli L, Barnett S, Goetz L, Toscano R. Vocational rehabilitation in spinal cord injury: what vocational service activities are associated with employment program outcome? Top Spinal Cord Inj Rehabil. 2015;21:31–9.
Cotner B, Njoh E, Trainor J, O’connor D, Barnett S, Ottomanelli L, et al. Facilitators and barriers to employment among veterans with spinal cord injury receiving 12 months of evidence-based supported employment services. Top Spinal Cord Inj Rehabil. 2015;21:20–30.
UNDP. Human development report 2019. United Nations Development Programme UN; 2019.
IPEA, PNUD. Radar IDHM: evolução do IDHM e de seus índices componentes no período de 2012 a 2017. Brasília: Instituto de Pesquisa Econômica Aplicada—IPEA; 2019.
Acknowledgements
We are grateful to all participants of the study for their time. We also thank the personnel of the Centro Catarinense de Reabilitação for being helpful with participants’ records.
Funding
This study was carried out with the support of the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq; Brazil) and Fundação de Amparo à Pesquisa e Inovação do Estado de Santa Catarina (TO2019TR767; FAPESC; Brazil).
Author information
Authors and Affiliations
Contributions
ADT, TCSL, SPBON, FF, CM-V, SMFV, JMS, NG, RGN, DAC and NAA contributed to the study conceptualisation and design. ADT, TCSL, SPBON, JMS, NG, DAC and NAA contributed to the data collection. ADT, TCSL and JI contributed to the data analysis. ADT and JI contributed to the data interpretation and writing of the report. SPBON, FF, CM-V, SMFV and RGN provided feedback on the report.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Tholl, A.D., Lima, T.C.S., Nogueira, S.P.B.O. et al. Labour market participation among rehabilitated individuals with spinal cord injury in Brazil: a cross-sectional study. Spinal Cord 61, 119–124 (2023). https://doi.org/10.1038/s41393-022-00846-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-022-00846-2
