
Abstract
Study design
Retrospective cohort study.
Objectives
To investigate the association between neutrophil percentage-to-albumin ratio (NPAR) and pneumonia in patients with SCI.
Setting
Department of Rehabilitation Medicine Center, West China Hospital, Sichuan University.
Methods
SCI patients admitted to West China Hospital within 24 h of injury were consecutively enrolled. Blood samples were collected on admission. Pneumonia was diagnosed based on chest radiography and clinician records of patient symptoms and laboratory tests. Multivariable logistic regression analysis was performed to determine the relationship between NPAR and pneumonia. Receiver operating characteristic (ROC) curves were generated to assess the predictive value of NPAR.
Results
A total of 264 SCI patients were included, of whom 65 (24.6%) developed pneumonia. NPAR was positively correlated with pneumonia (OR 2.66, 95% CI, 1.06–6.71, p = 0.038). Patients in the upper NPAR tertile (2.35–3.71) had a higher risk of pneumonia than patients in the lower tertile (1.66–2.12) after adjustment for potential confounders (OR 2.55, 95% CI, 1.05–6.19, p = 0.039). The risk of pneumonia increased stepwise across NPAR tertiles (p for trend = 0.031). The optimal cutoff value of NPAR for predicting pneumonia was 2.17 with a sensitivity of 0.82 and a specificity of 0.50. There was a significant interaction between NPAR and neurological level of injury (p for interaction = 0.034), with no significant association between NPAR and pneumonia in patients with cervical SCI.
Conclusions
A higher NPAR was independently associated with higher risk of pneumonia in a dose-dependent manner in patients with non-cervical SCI.
Similar content being viewed by others


Introduction
Pneumonia is one of the most common infections following acute traumatic spinal cord injury (SCI), ranging in frequency from 14% to 74% [1, 2]. It has been reported that pneumonia increases length of stay and impacts the neurological outcome in patients with SCI [3, 4]. Early identification of patients at high risk of pneumonia may assist with improving their management and prognosis, shortening length of stay, and reducing healthcare costs [2]. Therefore, a simple and effective biomarker is needed to predict pneumonia following SCI.
Neutrophils play a crucial role in the innate cellular immune system, and a high neutrophil percentage is predictive of bloodstream infection [5]. Albumin is the most abundant protein in plasma. Previous studies suggest that changes in serum albumin could reflect the severity of inflammation and illness in acute disease [6]. Recently, the neutrophil percentage-to-albumin ratio (NPAR) has been used as a novel predictor of systematic inflammation and infection. Several studies found that NPAR was associated with all-cause mortality in patients with coronary artery disease, sepsis or septic shock, myocardial infarction, cardiogenic shock, and acute kidney injury [7,8,9,10,11,12]. However, the relationship between NPAR and pneumonia in patients with SCI remains unclear. In the current study, we explored the association between NPAR and pneumonia in these patients.
Methods
Study population
This study retrospectively and consecutively enrolled SCI patients admitted to West China Hospital between January 1, 2016 and September 31, 2021. Patients were included if they fulfilled the following inclusion criteria: (1) admitted with 24 h after injury and (2) had a traumatic etiology. The exclusion criteria were as follows: (1) younger than 18 years; (2) missing neurological level of injury (NLI); and (3) missing the American Spinal Injury Association Impairment Scale (AIS) on admission. This study was approved by the Scientific Research Department of West China Hospital, and the need for informed consent was waived.
Data collection
The demographics and baseline characteristics were documented. The extent of neurological impairment was assessed using the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) on admission. Admission NLI was categorized into four groups: C2-C4, C5-C8, T1-T12, and L1-L4. Blood samples were collected for laboratory measurements in the emergency department upon admission. White blood cell (WBC) counts, including absolute numbers of neutrophils, were measured using an automated hematology analyzer (Sysmex, Kobe, Japan). Serum albumin levels were determined with an Olympus AU-5400 automatic analyzer (Olympus, Tokyo, Japan). Multi-trauma was defined as concurrent traumatic injuries in other body systems (e.g., rib or sternal fractures, peripheral limb fractures, and presence of pneumothorax and/or hemothorax) [13].
Outcome
The primary outcome was pneumonia, which was diagnosed during hospitalization according to radiological findings based on Centers for Disease Control and Prevention (CDC) criteria in accordance with recent consensus definitions for stroke-associated pneumonia [14, 15]. In brief, pneumonia was assessed by a combination of clinician records of patient symptoms and laboratory tests, including chest radiograph records and sputum microbiology tests.
Statistical analysis
Continuous variables were presented as means with standard deviations (SDs) or medians with interquartile ranges (IQRs) as appropriate. Categorical variables were shown as frequencies or percentages. Descriptive analyses of baseline characteristics were reported for groups with or without pneumonia using the Fisher’s exact test for categorical variables and the Mann-Whitney U test for numeric data. Variables within p < 0.10 in univariable analysis were defined as potential confounders. Multivariable logistic regression analysis was performed to explore the association between NPAR and pneumonia. Trends for the odds ratios (ORs) of pneumonia across NPAR tertiles (p for trend) were tested by entering the median value of NPAR in each tertile as a continuous variable [16]. A spline regression model was conducted to investigate the pattern and magnitude of the relationship between NPAR and pneumonia with four knots (at the 25th, 50th, 75th and 95th percentiles), and the reference point was set as the median value of NPAR in the first tertile. A receiver operating characteristic (ROC) curve was calculated to assess the diagnostic value of NPAR in predicting pneumonia. Discrimination of NPAR was evaluated by the area under the ROC curve (AUC). The optimum NPAR cutoff point was determined by the Youden index. In addition, we compared the AUC of NPAR with that of neutrophil percentage and albumin in predicting pneumonia (the Delong method) [17]. Subgroup analysis was performed to assess the potential effect modification by prespecified confounders: smoking, multitrauma, admission NLI, and admission AIS grade. Interactions between NPAR and variables on pneumonia were tested by the likelihood ratio test.
All statistical analyses were performed using R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria), MedCalc 15.2.2 (MedCalc Software bvba, Ostend, West Flanders, Belgium) and STATA 14.0 (Corporation, College Station, TX, USA). A two-sided P value less than 0.05 was considered statistically significant.
Results
Baseline characteristics and outcomes
We enrolled 274 patients with traumatic SCI; 10 patients were excluded because they were younger than 18 years (n = 6) or had missing NLI and AIS grade on admission (n = 4) (Fig. 1). In total, 264 patients were included in this study. The mean (SD) age was 42.3 (11.9) years, and 221 (83.7%) cases were males. The baseline characteristics of patients stratified by pneumonia were shown in Table 1. The median NPAR was 2.21 (IQR 2.07–2.44). Out of 264 patients, 65 (24.6%) patients developed pneumonia.

AIS American Spinal Injury Association Impairment Scale, NLI neurological level of injury, SCI spinal cord injury.
Association between NPAR and pneumonia
The univariable analysis showed that length of stay, body mass index (BMI), admission NLI, admission AIS grade, and tracheotomy were significant confounders affecting pneumonia incidence (p < 0.1, Table 1).
In multivariable logistic regression analysis, NPAR was positively associated with pneumonia when it was treated as a continuous variable (OR 2.66, 95% CI, 1.06-6.71, p = 0.038). When NPAR was classified into tertiles, the OR of pneumonia was 2.60 for T2 and 4.68 for T3, when compared with T1 without adjustment. After multivariable adjustment, T3 still had a significantly higher risk of pneumonia than T1 (OR 2.55, 95% CI, 1.05-6.19, p = 0.039), while T2 was no longer significantly different from T1(OR 1.47, 95% CI, 0.58-3.76, p = 0.420). The risk of pneumonia significantly increased stepwise across NPAR tertiles (p for trend = 0.031). As shown in Fig. 2, with an increase in NPAR, the adjusted ORs for pneumonia increased in a dose-dependent manner (Table 2).

Solid lines represent the odds ratio of pneumonia and dotted lines represent the corresponding 95% CI. ORs were adjusted for length of stay, BMI, admission NLI, admission AIS grade, and tracheotomy. OR = 1 was set as the reference line. AIS American Spinal Injury Association Impairment Scale, BMI body mass index, NLI neurological level of injury, NPAR neutrophil percentage-to-albumin ratio.
Predictive value of NPAR
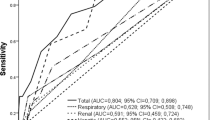
The ROC analysis suggested that the optimal cutoff value of NPAR for predicting pneumonia was 2.17, with a sensitivity of 0.82 and specificity of 0.50 (Fig. 3). Comparing the predictive value with other biomarkers, NPAR showed the highest AUC value (0.672 [0.612–0.729]) compared with albumin (0.669 [0.609–0.726]) and neutrophil percentage (0.509 [0.447–0.571]), but the difference between NPAR and albumin was not significant (p = 0.885) (Fig. 3).

NPAR neutrophil percentage-to-albumin ratio.
Subgroup analysis
Stratified logistic regression analyses were conducted to further evaluate the association between NPAR and pneumonia with adjustment for potential confounders (Table 3). The association between NPAR and pneumonia could be modified by NLI (p for interaction = 0.034). In patients with thoracic or lumbar SCI, NPAR had a significant positive relationship with pneumonia (OR 7.03, 95% CI, 1.86-26.56, p = 0.004), but it was no longer significant in patients with cervical SCI (OR 0.84, 95% CI, 0.22-3.14, p = 0.792).
Discussion
In this study, we investigated the relationship between NPAR and pneumonia in SCI patients. We found that NPAR positively correlated with pneumonia and that the risk of pneumonia increased with increasing NPAR tertiles in a dose-dependent manner after adjustment for confounders. This relationship was significant only for patients with thoracic or lumbar SCI.
There are several possible explanations for the relationship between NPAR and pneumonia. The increase in NPAR may be due to an increase in neutrophil percentage and/or a decrease in albumin levels. The acute myeloid response to traumatic SCI is hallmarked by systemic neutrophilia [18]. Neutrophils are the first peripheral cells to enter the injured central nervous system [19]. The recruited neutrophils in the injured spinal cord could promote additional damage by producing and releasing pro-inflammatory cytokines and other cytotoxic factors [20, 21]. It has been reported that neutrophil mobilization and recruitment to the lesion site are negatively associated with outcomes in SCI mice [22]. Moreover, the lungs are the major target of SCI-induced acute inflammation [23]. Therefore, due to the injurious role of neutrophils, patients with a high neutrophil percentage might be at high risk of pneumonia.
Hypoalbuminemia is associated with adverse clinical outcomes in hospitalized patients [6]. Although serum albumin has been broadly used to reflect nutrition status in clinical practice, the relevance of serum albumin as a specific nutrition marker has been questioned in recent decades [24]. A prospective cohort study of 2465 patients suggested that both inflammation and elevated nutritional risk were independently associated with hypoalbuminemia in acutely ill patients [6]. It has also been reported that hypoalbuminemia was associated with impaired immune function and pulmonary edema, which could increase the risk of infection [25, 26]. In addition, a retrospective study involving 705 ischemic stroke patients found that serum albumin level is an independent predictor of stroke-associated pneumonia [27]. Therefore, patients with relatively low serum albumin levels might be at high risk of pneumonia. In the current study, the predictive value of NPAR outperformed that of neutrophil percentage and albumin. Based on the above evidence, we proposed that NPAR, a combination of neutrophils and albumin, could be a potential predictor of pneumonia in SCI patients.
In our study, an interaction between NPAR and NLI was discovered: NPAR was positively associated with pneumonia only in patients with thoracic or lumbar SCI. There is a possible explanation for this phenomenon. Injuries to the cervical spinal cord lead to an increased risk of respiratory impairments due to disruption of spinal nerves that innervate respiratory muscles [28]. The severity correlates with higher spinal injuries [29]. In our study, patients with pneumonia had a higher proportion of cervical SCI than patients without pneumonia (66.1% vs 38.2%). Therefore, we speculate that in patients with cervical SCI, the role of NLI in the risk of pneumonia attenuates the association between NPAR and pneumonia, which makes the effect of NPAR insignificant.
Patients are at high risk of pneumonia following SCI due to multiple causes, such as deterioration of gas exchange, insufficient coughing, and SCI-induced systemic immune depression [30]. In our study, the incidence rate of pneumonia was 24.6%, which was similar to a retrospective study of 161 SCI patients [18], but was lower than a cohort of 37 patients with cervical and complete motor function injury [31]. The discrepancy across studies might have resulted from different diagnostic criteria of pneumonia and study populations. In accordance with a recent consensus on stroke-associated pneumonia, we combined chest radiographs as well as clinical and microbiological signs to conduct a complete diagnosis [15]. A more standardized method to evaluate pneumonia following SCI is needed.
Patients suffering from pneumonia had poorer functional recovery and long-term survival than those who did not develop pneumonia [3]. Therefore, early prediction of pneumonia may enable clinicians to be more vigilant in conducting preventive measures. We found that NPAR was an independent predictor of pneumonia, even after adjustment for clinically significant pneumonia predictors, including length of stay, NLI, AIS grade, and tracheotomy. NPAR is a combination of neutrophils and albumin levels, both of which are accessible in daily clinical practice. NPAR amplifies the changes in neutrophil percentage and albumin, especially when these two parameters fluctuate within the normal range, which might be overlooked by clinicians.
Our study has some limitations. First, this was a single-center retrospective study, which could lead to selection bias. Second, as in all observational studies, we cannot account for confounding due to unmeasured covariates. Third, neutrophils and serum albumin levels are two dynamic parameters, and the interval between injury and admission might lead to bias. However, we only included SCI patients with 24 h of injury, and univariable analysis suggested that interval was not regarded as a significant confounder. Fourth, due to the retrospective design of this study, we did not have data on the long-term outcome of SCI patients.
Conclusion
In conclusion, we found that NPAR was independently associated with pneumonia in patients with non-cervical SCI and that the risk of pneumonia increased stepwise with increasing NPAR. Monitoring NPAR may help clinicians identify patients at high risk of pneumonia. Further studies are needed to verify our results and understand the mechanism underlying the association between NPAR and pneumonia.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Weinberg DS, Hedges BZ, Belding JE, Moore TA, Vallier HA. Risk factors for pulmonary complication following fixation of spine fractures. Spine J. 2017;17:1449–56.
Agostinello J, Battistuzzo CR, Batchelor PE. Early clinical predictors of pneumonia in critically ill spinal cord injured individuals: a retrospective cohort study. Spinal Cord. 2019;57:41–8.
Kopp MA, Watzlawick R, Martus P, Failli V, Finkenstaedt FW, Chen Y, et al. Long-term functional outcome in patients with acquired infections after acute spinal cord injury. Neurology. 2017;88:892–900.
Winslow C, Bode RK, Felton D, Chen D, Meyer PR Jr. Impact of respiratory complications on length of stay and hospital costs in acute cervical spine injury. Chest. 2002;121:1548–54.
Pan YP, Fang YP, Xu YH, Wang ZX, Shen JL. The diagnostic value of procalcitonin versus other biomarkers in prediction of bloodstream infection. Clin Lab. 2017;63:277–85.
Eckart A, Struja T, Kutz A, Baumgartner A, Baumgartner T, Zurfluh S, et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: a prospective study. Am J Med. 2020;133:713–22. e7
Sun T, Shen H, Guo Q, Yang J, Zhai G, Zhang J, et al. Association between neutrophil percentage-to-albumin ratio and all-cause mortality in critically ill patients with coronary artery disease. Biomed Res Int. 2020;2020:8137576.
Wang X, Wang J, Wu S, Ni Q, Chen P. Association between the neutrophil percentage-to-albumin ratio and outcomes in cardiac intensive care unit patients. Int J Gen Med. 2021;14:4933–43.
Gong Y, Li D, Cheng B, Ying B, Wang B. Increased neutrophil percentage-to-albumin ratio is associated with all-cause mortality in patients with severe sepsis or septic shock. Epidemiol Infect. 2020;148:e87.
Cui H, Ding X, Li W, Chen H, Li H. The neutrophil percentage to albumin ratio as a new predictor of in-hospital mortality in patients with ST-segment elevation myocardial infarction. Med Sci Monit. 2019;25:7845–52.
Yu Y, Liu Y, Ling X, Huang R, Wang S, Min J, et al. The neutrophil percentage-to-albumin ratio as a new predictor of all-cause mortality in patients with cardiogenic shock. Biomed Res Int. 2020;2020:7458451.
Wang B, Li D, Cheng B, Ying B, Gong Y. The neutrophil percentage-to-albumin ratio is associated with all-cause mortality in critically ill patients with acute kidney injury. Biomed Res Int. 2020;2020:5687672.
Yue JK, Winkler EA, Rick JW, Deng H, Partow CP, Upadhyayula PS, et al. Update on critical care for acute spinal cord injury in the setting of polytrauma. Neurosurg Focus. 2017;43:E19.
Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36:309–32.
Smith CJ, Kishore AK, Vail A, Chamorro A, Garau J, Hopkins SJ, et al. Diagnosis of stroke-associated pneumonia: recommendations from the pneumonia in stroke consensus group. Stroke. 2015;46:2335–40.
Park SY, Freedman ND, Haiman CA, Le Marchand L, Wilkens LR, Setiawan VW. Association of coffee consumption with total and cause-specific mortality among nonwhite populations. Ann Intern Med. 2017;167:228–35.
DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44:837–45.
Jogia T, Lübstorf T, Jacobson E, Scriven E, Atresh S, Nguyen QH, et al. Prognostic value of early leukocyte fluctuations for recovery from traumatic spinal cord injury. Clin Transl Med. 2021;11:e272.
David S, Kroner A, Greenhalgh AD, Zarruk JG, López-Vales R. Myeloid cell responses after spinal cord injury. J Neuroimmunol. 2018;321:97–108.
Kanyilmaz S, Hepguler S, Atamaz FC, Gokmen NM, Ardeniz O, Sin A. Phagocytic and oxidative burst activity of neutrophils in patients with spinal cord injury. Arch Phys Med Rehabil. 2013;94:369–74.
Kubota K, Saiwai H, Kumamaru H, Maeda T, Ohkawa Y, Aratani Y, et al. Myeloperoxidase exacerbates secondary injury by generating highly reactive oxygen species and mediating neutrophil recruitment in experimental spinal cord injury. Spine. 2012;37:1363–9.
Brennan, FH, Jogia, T, Gillespie, ER, Blomster, LV, Li, XX, Nowlan, B, et al. Complement receptor C3aR1 controls neutrophil mobilization following spinal cord injury through physiological antagonism of CXCR2. JCI Insight. 2019;4:e98254.
Sun X, Jones ZB, Chen XM, Zhou L, So KF, Ren Y. Multiple organ dysfunction and systemic inflammation after spinal cord injury: a complex relationship. J Neuroinflammation. 2016;13:260.
Lee JL, Oh ES, Lee RW, Finucane TE. Serum albumin and prealbumin in calorically restricted, nondiseased individuals: a systematic review. Am J Med. 2015;128:1023.e1–22.
Soeters PB, Wolfe RR, Shenkin A. Hypoalbuminemia: pathogenesis and clinical significance. JPEN J Parenter Enter Nutr. 2019;43:181–93.
Arques S. Human serum albumin in cardiovascular diseases. Eur J Intern Med. 2018;52:8–12.
Dziedzic T, Pera J, Klimkowicz A, Turaj W, Slowik A, Rog TM, et al. Serum albumin level and nosocomial pneumonia in stroke patients. Eur J Neurol. 2006;13:299–301.
Terson de Paleville DG, McKay WB, Folz RJ, Ovechkin AV. Respiratory motor control disrupted by spinal cord injury: mechanisms, evaluation, and restoration. Transl Stroke Res. 2011;2:463–73.
Brown R, DiMarco AF, Hoit JD, Garshick E. Respiratory dysfunction and management in spinal cord injury. Respir Care. 2006;51:853–68. discussion 69-70
Failli V, Kopp MA, Gericke C, Martus P, Klingbeil S, Brommer B, et al. Functional neurological recovery after spinal cord injury is impaired in patients with infections. Brain. 2012;135:3238–50. Pt 11
Liebscher T, Niedeggen A, Estel B, Seidl RO. Airway complications in traumatic lower cervical spinal cord injury: A retrospective study. J Spinal Cord Med. 2015;38:607–14.
Funding
This work was supported by the National Natural Science Foundation (82102656); China Postdoctoral Science Foundation (2021M692299); PostDoctor Research Project, West China Hospital, Sichuan University (2021HXBH021); Sichuan Provincial Natural Science Foundation of China (2022NSFSC1312).
Author information
Authors and Affiliations
Contributions
CQH and QW conceived and designed the study. CYW, XY, TTW, LYR, LW, and XS acquired the data, which CYW analyzed. CYW, XY, TTW, and MFD aided in data interpretation and wrote the manuscript. All authors were involved in revising the article and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was approved by the Scientific Research Department of West China Hospital (approval no. 2021-1413).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wang, C., Yu, X., Wang, T. et al. Association between neutrophil percentage-to-albumin ratio and pneumonia in patients with traumatic spinal cord injury. Spinal Cord 61, 106–110 (2023). https://doi.org/10.1038/s41393-022-00844-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-022-00844-4
