
Abstract
Study design
Systematic review.
Objectives
We aimed to provide a comprehensive overview of the English and Chinese literature reporting epidemiological data on spinal cord injury (SCI) in China.
Methods
3 English and 3 Chinese language electronic databases were searched from the earliest record to 15 March 2020. Sociodemographic characteristics, incidence rates, etiology and lesion characteristics, in-hospital mortality, and secondary health conditions and complications were extracted from included reports.
Results
A total of 51 studies were included, 32 in the Chinese language. Forty-seven studies were based on hospital records. Mean age of incident cases ranged from 34 to 55 years and male-to-female ratios ranged from 0.35:1 to 15.3:1. SCI incidence varied from 14.6 to 60.6 per million. Thirty-five studies reported only on traumatic SCI with traffic accidents, high falls, low falls and being hit by objects being the most common causes. Specific causes for non-traumatic SCI were poorly reported. Proportions with tetraplegia and complete injury ranged from 37.4% to 82.0% and 14.1% to 73.9%, respectively. Reported in-hospital mortality attributed to SCI varied from 1.1% to 18.4%. Leading cause of in-hospital mortality for acute SCI was respiratory problems; respiratory problems, urinary tract infections and pressure sores were the most common complications.
Conclusion
Epidemiological data on SCI in China are only available for a limited number of provinces and mostly outdated. Updated data on incidence with accurate geographical information and etiology across all Chinese provinces are needed for targeted implementation of preventive strategies. Research on community outcomes needs to be developed in China.
Similar content being viewed by others


Introduction
Regularly updated epidemiological data on spinal cord injury (SCI) are important for tracing case numbers and causes, identifying prevention targets and risk factors for poor health outcomes or premature mortality after onset, as well as for public health and clinical resource allocation [1,2,3,4]. More specifically, having sound data on the epidemiology of SCI enables the optimization of targeted preventive interventions as well as the development of rehabilitation services and ultimately health policy planning. China is an interesting case for studying the epidemiology of SCI because of its rapid economic growth, urbanization, and an aging population. Growth in private car ownership and in traffic volume since early 2000 has led to a significant increase in traffic accidents [5]. This likely impacts on traumatic SCI incidence. Moreover, population ageing has led to an increase in non-communicable diseases and disability, with an increase in non-traumatic SCI being a possible consequence [6].
Two systematic reviews of the epidemiology of SCI in China have been conducted. Yuan and colleagues [7] reviewed 17 studies published until January 2018 and Chen and colleagues [8] reviewed 32 studies from January 1978 to August 2017. Both reviews used narrow inclusion criteria. Yuan and colleagues restricted their review to four cities and four provinces, including only publications in English, while Chen and colleagues solely reviewed studies that focused on the treatment costs of traumatic SCI and ignored other data. A non-systematic, narrative review by Reinhardt and colleagues [9] on epidemiological data solely covered the English literature as indexed in PubMed up to 2016.
The present study aims to address these gaps by systematically reviewing the English and Chinese literature reporting epidemiological data on SCI in China, extracting data on study methodology, demographic and injury characteristics, incidence and prevalence rates; and outcomes including in-hospital mortality, and secondary health conditions and complications.
Methods
Design
This is a systematic review of the literature.
Eligibility criteria
We included original articles written in Chinese or English that reported epidemiological data on: (1) demographic characteristics of the studied SCI populations; (2) incidence and/or prevalence estimates; (3) injury characteristics; and/or (4) outcomes including in-hospital mortality for incident SCI as well as readmissions and secondary health conditions and complications for traumatic or non-traumatic SCI in China. As a minimum requirement, included studies needed to report on patient source and sample size, age and gender, and basic etiology of SCI (traumatic vs. non-traumatic). Included were only studies that reported data for defined populations/cohorts based on hospital records or population-based registries and surveys. No restrictions regarding year of publication were imposed.
Studies on populations with spinal fractures that did not report separate data for those with SCI, those focusing on a specific etiology such as traffic accidents or neoplasms, or on a specific lesion type (complete or incomplete only) or lesion level (paraplegia or tetraplegia only) were also ineligible. If studies reported the same data in Chinese and English, the English language version was selected for data extraction. Comments, reviews, proceedings, conference abstracts, case reports, letters and editorials were excluded
Retrieval of records and search strategy
We searched the following databases for original peer-reviewed studies from the earliest record to 15 March 2020: Web of Science, PubMed, Embase, Wan Fang Data, China Science and Technology Journal Database (VIP) and China National Knowledge Infrastructure Database (CNKI). The search strategy combined relevant epidemiological terms and terms related to SCI in a free text search of all fields of database records, with the exception of PubMed where the search was restricted to title and abstract as otherwise too many irrelevant records were retrieved. An example for Embase was: ((“spinal cord” or “spinal cord injury” or “paraplegia” or “tetraplegia”) and (“epidemiology” or “incidence” or “etiology” or “prevalence”) and “China”). The full search strategy can be found in the Supplementary Appendix (Table S1). In order to capture all relevant reports, the reference lists of all included studies and relevant systematic reviews were also screened.
Study selection
All references from the six electronic databases were uploaded into EndNote (X9), and duplicates removed. Two authors (CC and WL) independently screened titles and abstracts based on the eligibility criteria. Full texts of relevant articles were then obtained, and both of the reviewers assessed these independently for eligibility. Conflicts were resolved by discussion among the reviewers, or where necessary by involvement of a third researcher (JR).
Data extraction and synthesis
Two authors (CC, and WL or XQ) independently completed data extraction. For each study, we extracted the following data into an Excel spreadsheet: (1) basic study characteristics, including first author, region of study, study period, data source (e.g. hospital records, database of community organization), case type (incident vs. prevalent), and sample size; (2) sample demographics: age range, mean age, modal age group, male-female ratio, employment status and type of occupation if employed; (3) incidence and prevalence estimates; (4) lesion characteristics: etiology, lesion level and severity; (5) duration of inpatient hospitalization (for hospital-based studies, separated by acute vs. rehabilitation and first admissions vs. readmissions if this information was available), secondary health conditions and complications (occurrence and leading cause), and in-hospital mortality (rate and leading cause).
Data were synthesized narratively using a synthesis without meta-analysis (SWiM) [10] approach.
Quality assessment
Quality assessment was performed by two authors (CC and WL) using the Appraisal tool for Cross-Sectional Studies (AXIS tool) [11]. The AXIS tool has 20 items (see Supplementary Appendix Table S2) that relate to the overall quality of reporting (7 items), study design (7 items), and sources of bias (6 items). Items were summed, with higher scores (range 0–20) indicating better quality.
Results
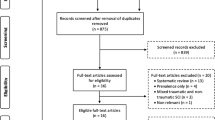
The study selection process is presented in Fig. 1. The initial database search yielded 1,108 records, with 386 from Web of Science, 55 from PubMed, 300 from Embase, 237 from Wan Fang Data, 55 from VIP and 77 from CNKI. Five additional records were identified from reference lists of papers included in full text review as well as the three previous reviews [7,8,9].

Adapted from Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
Study characteristics
Fifty-one relevant studies (*1–*51, see Supplementary Appendix for the reference list) were identified; their general characteristics are detailed in Table 1. Quality scores ranged from 5 to 17 (Median: 14, IQR: 13–15); details are given in Supplementary Appendix (Table S3). Regarding sources of bias, only 3 studies reported measures used to address non-responders/missing data and less than half of the studies (20) discussed the limitations of the study.
Forty-eight (94%) studies were based on reviews of hospital records, two were based on information from community surveys, and one extracted information from a database of a community organization providing services to people with SCI. Thirty-five studies reported on incident cases (all based on admissions to hospital with new SCI in a given period), three studies reported on prevalent cases, and for 13 studies this was unclear. Of the three studies reporting on prevalent cases, two were community surveys: one (Chan *1) was based on samples of people with SCI registered as outpatients at various rehabilitation centers or as users of a community resource center in Hong Kong (average time since injury 13.3 years, (standard deviation [SD] 10) and the other one (Wang *30) reports results from a mailed survey of members of a Taiwanese SCI patient organization and users of community-based outpatient rehabilitation centers with a range of time since SCI from 6 months to over 10 years (no average given). The third study (Chang *2) analyzed data on people with SCI who had received services from community-based outpatient rehabilitation centers. These data were extracted from the management system of the Disabled Persons Federation of Shanghai (time from injury to service 12.8, SD 10.6). Epidemiological data reported covered the period from 1978 to 2017; only one study from Hong Kong (Chan *1) did not report the study period. Maximum sample size was 3,832, and minimum was 35. The data were from 21 provinces, representing a total of 956 million population (census 2010): Tianjin, Guangxi, Guangdong, Shanxi, Fujian, Beijing, Jilin, Shaanxi, Liaoning, Hunan, Hubei, Jiangsu, Shanghai, Chongqing, Heilongjiang, Taiwan, Sichuan, Guizhou, Shandong, Hong Kong and Anhui. Over 50% of the studies investigated SCI populations from only five provinces/cities, namely: Tianjin (10 studies), Beijing (6 studies), Shanghai, Guangdong, and Shanxi (4 studies from each). Three studies did not report the geographical area of data collection. No studies were found for 13 provinces: Xinjiang, Tibet, Gansu, Qinghai, Neimenggu (inner Mongolia), Henan, Hebei, Yunnan, Jiangxi, Hainan, Macao, Zhejiang and Ningxia (Fig. 2), representing a population of 407 million (census 2010).

The figure shows the distribution of studies (A) and reported SCI incidence (B) across various provinces and territories of China. The numbers of studies from each province and SCI incidence in each province of China where data was available are presented in these two maps of China highlighting the relevant provinces and cities and using shading to indicate the number of studies reporting relevant data. Pop Population size, mio Million.
Demographic characteristics
Of the studies included in this review, one reported on children only (Wang *32) and one on elderly persons only (Yu *48). When we exclude these two studies, the mean age of incident cases investigated ranged from 34–54 years, and the mean age of prevalent cases was 45.2 years. Ten studies did not report details on the age range. The largest age group in most studies comprised people aged 30–60 years; only three studies (Jiao *34, Feng *12, Chen *3) reported that the largest age group was under 30 years. A study from Beijing (Wang *32) reported the lowest male-to-female ratio (0.35:1) and a study from Shanxi (Jiang *18) the highest (15.3:1). There were only two studies in which the male-to-female ratio was below 1, the one from Beijing (0.35:1) (Wang *32) and one from Sichuan (0.94:1) (Liu *23). Twelve articles reported on the rate of people with SCI who were not employed at injury which ranged from under one (Yang *43) to 87% (Wang *30). Studies showed a high proportion of persons not in employment before 2010, which declined in 2010-2014 and was lowest in the last five years (2015-2019) (Table 2). Less than half of the studies reported on the type of occupation of people with SCI who were employed at the time of the injury. The most common occupational groups were unskilled worker and small farmers/farmhands.
Incidence and prevalence
Incidence rates, that is the number of cases with new SCI in a defined area during a specific time period divided by the total population at risk during the same time period, were reported in nine studies (see Table 2, Fig. 2). Incidence rates for traumatic SCI varied from 14.6 per million per year in Taiwan in 1985 (Chen *3) to 60.6 per million per year in Beijing in 2002 (Li *21). Only one study drew on data collected after 2010 (Ru *28), and only one study conducted in 2005 (Wei *34) included non-traumatic SCI. The latter study estimated the combined incidence rate for both traumatic and non-traumatic SCI but did not provide numbers for the etiology subgroups. An increasing trend in incidence rates over time was found in two studies from Taiwan (Chen *3, Chen *4) and two from Tianjin (Ning *24, Yu *46). Two studies from Beijing conducted at different time points (Li *21, Wei *34) showed similar incidence rates. However, the latter study (Wei *34) also included an unspecified proportion with non-traumatic SCI (Fig. 2).
Prevalence rates were not reported in any study.
Injury characteristics: Etiology, lesion level and lesion severity
Thirty-five (69%) studies reported on traumatic SCI only and 16 studies on both traumatic and non-traumatic SCI; none of the studies focused on non-traumatic SCI only. In the studies reporting on both traumatic and non-traumatic SCI, only three (18%) reported proportions for different etiologies; traumatic SCI accounted for 58% (Chang *2), 72% (Yuan *50), and 90% (Wei *34), respectively. Modal age groups (average age was only reported by Wei *34) differed between those studies; the younger the modal age group was, the higher was the reported proportion of traumatic SCI. Trauma was the leading cause of SCI among those aged 16–60 years, while non-traumatic causes were more common in people who were older. The following specific causes were reported for traumatic SCI in at least one of the reviewed studies (Table 2): traffic accidents, falls at ground level (low falls), falls from a height (high falls), crush injury (mostly resulting from falling objects), work-related injury, sport-related injury, and surgical complications. Among these causes, traffic accidents, high falls, low falls and being hit by falling objects were the leading causes in all reports apart from one 2012 study from Shanxi (Jiang *19) which listed coal mine work-related injuries as the most frequent cause of SCI, and one 2000 report from Hong Kong (Chan *1) which noted that work-related injuries and surgical complications were the most common causes. Specific causes for non-traumatic SCI were not reported in any study.
Twelve studies (Chan *1, Chen *3, Chen *8, Feng *13, Li *22, Ning *24, Ning *25, Ru *28, Wang *30, Yang *41, Yi *44, Zhou *51) reported on lesion level and lesion severity, while 16 studies (Chang *2, Chen *5, Chen *6, Hao *14, Hua *16, Huang *17, Jiang *18, Niu *26, Wang *32, Wei *34, Yang *39, Yang *40, Yang *43, Yu *46, Yu *47, Yuan *50) reported only on lesion severity. The proportion with tetraplegia was higher than that with paraplegia in nine studies (Chen *8, Feng *13, Li *22, Ning *24, Ning *25, Ru *28, Yang *41, Yi *44, Zhou *51), while three studies (Chan *1, Chen *3, Wang *30) reported the opposite.
In-hospital mortality and complications
Eleven studies (21.6%) reported the average length of stay in the hospital, all for a first admissions for acute SCI; the duration ranged from 13.7 to 100 days. Two studies (Chen *3, Chen *4) reported length of stay by lesion level and lesion severity. In both, length of stay was longest for people with complete tetraplegia. Reported in-hospital mortality attributed to SCI in studies of incident cases varied from 1.1% (Yang *41) to 18.4% (Chen *9); 31 studies did not provide mortality figures. A comparison of eight studies conducted in Tianjin from 2010 to 2019 and two performed in Guangdong in 2011 and 2017 shows decreasing in-hospital mortality. Eighteen studies (35%) reported the leading cause of death, which were respiratory problems in all studies except one from Tianjin conducted in 2016 (Zhou *51). (Table 3).
Most studies reported a high occurrence of secondary health conditions and complications, ranging from 25 to 88% in studies of prevalent cases and from 6 to 97% in studies of incident cases. Only two studies reported a rate of secondary health conditions and complications below 10%, one from Liaoning performed in 2014 (Ru *28) (8%) and one from Tianjin performed in 2016 (6%) (Zhou *51). In the 25 studies that reported on the occurrence of complications in hospital, on average 26% of the patients treated experienced any complications (weighted by sample size; 95% confidence interval: 19% to 34%). The three most common complications were respiratory problems, urinary tract infections and pressure sores. In the only study (Wang *30) that reported on secondary health conditions and complications in community-dwelling persons with SCI, prevalence was 88% with urinary tract infections, pain, and pressure ulcers being the most frequent conditions (Table 3).
Discussion
This systematic review provides an update on the epidemiology of SCI in China, and is the first that includes epidemiological data from all provinces of China, where available. We reviewed 51 studies from 21 provinces; none reported national epidemiological data. Notably, the absence of any research related to SCI epidemiology in 13 provinces and cities with provincial status, and the existence of a single study only from another 13 provinces severely limits the derivation of epidemiological data for the entire country. This issue is even more severe when it comes to estimates of incidence rates, with relevant data being available only for six out of 34 provinces/territories and cities (Fig. 2). In addition, data are outdated: only one study reported on incidence rates after 2010. While the number of studies conducted in different provinces roughly reflects economic development, with more studies conducted in the better developed east and south of China, it is unclear why epidemiological research on SCI, and in particular attempts to estimate SCI incidence, have significantly declined in the last decade. One possible explanation is the increased competitiveness of research grants in China over the last decade, with studies solely reviewing hospital records generally not funded any longer.
The range of incidence rates for SCI reported in the studies was similar to estimates from a previous systematic review focusing on the Asian region [12] that found incidence rates for traumatic SCI ranging between 12.06 and 61.6 per million persons; the range was slightly lower than figures from North America (27.1 to 83.0 per million) [13]. However, incidence rates were only estimated for traumatic SCI, and only one study from Liaoning (Ru *28) was available from the last decade. At time of writing, data on the prevalence and incidence of non-traumatic SCI had not been collected in China.
A trend towards an increasing age at SCI was seen when comparing studies from the same province conducted at different time points, most likely owing to population ageing. In our review, there were significant gender and occupational differences between reports, with a higher proportion of men than of women incurring SCI, and a higher proportion of small farmers/farmhands and unskilled workers than of other occupational groups. High male-to-female ratios in traumatic SCI are well known from previous reviews [7, 14]. One possible reason for this finding in China is that men are more likely to work in high-risk occupations such as taxi or truck driver, construction worker or miner. For example, one report from Shanxi (Jiang *19) studied patients with SCI who had been working in coal mines and reported the highest male to female ratio. Insufficient safety provisions at work, unsafe transportation such as motorcycles and motorized tricycles and limited affordability of health care for treatment of non-traumatic conditions that may cause spinal cord lesions may be responsible for higher rates of SCI in peasants and unskilled workers. Efforts of the government of the People’s Republic of China to improve safety at work and on the road need to be intensified.
In the current study, traffic accidents and falls (including high falls and low falls) were the main causes of SCI, a finding already reported by earlier reviews [7, 9]. Increasing numbers of private cars and an increase in traffic volume due to urbanization may be important contributors to traffic-related injuries. Lack of safety on construction sites (Jiang *19) and an increasing numbers of suicide attempts [15] may play important roles in high falls. In contrast, low falls are more common in the elderly. Low falls may have become more pronounced due to a growing number of elderly people in China who live alone and not within the household of their children as it traditionally was the case. Being hit by falling objects is a cause we do not frequently see in other countries with data on SCI etiology. This type of mechanism may result from natural disasters (e.g., earthquakes and storms) but also from construction and mining accidents. It is further of note that studies including cases with non-traumatic SCI did not report any specific etiology. As a result, non-traumatic SCI in China remains a largely unknown issue.
Only a few studies reported on hospital mortality and an unknown number of patients with SCI may have died on site or while being transported toa hospital.
One consequence of increased survival after SCI is the high number of reported complications. We found that respiratory problems, urinary tract infections and pressure sores were the main complications, which is consistent with results from other countries and underlines the global importance of research into the prevention and treatment of these conditions after the onset of SCI [16, 17]. However, we observed striking differences in the prevalence of secondary health conditions and complications across studies (ranging from 97% [Chen *6] to below 10% [Ru *28, Zhou *51]). It remains therefore unclear whether the data are comparable as it is highly likely that secondary conditions and complications were defined and assessed differently in these studies.
Several limitations of this review should be noted. First, our search strategy did not specify medical subject headings (MeSH) and the PubMed search was limited to the title and abstract only. This strategy was chosen to avoid the retrieval of too many irrelevant records. In contrast to studies with a primary epidemiological purpose which were likely to be captured by our search, we may have missed studies that had another main focus but nevertheless reported relevant epidemiological data. Second, most studies were reviews of hospital records and community-based research was very limited, making it impossible to draw any conclusions about community outcomes. However, hospital records might allow for more reliable conclusions, as non-response bias is less of concern than in community-based studies. Third, time series data are lacking and any time trends reported here are based on a comparison of cross-sectional studies from the same province conducted at different time points, often employing different methodology. This makes it impossible to disentangle longitudinal developments from variations in the selection of samples and the methodology used. Fourth, epidemiological data on SCI were variably defined in the included studies, for example with regard to level and completeness or lesion, precluding meta-analysis. It is desirable that future studies adhere to common data collection standards such as the international SCI Core Data Set [18], ICF (International Classification of Functioning, Disability and Health) Core Sets for SCI [19], and those suggested by the IPSCI (International Perspectives on Spinal Cord Injury) [20] to enable better comparability between studies.
Conclusions
Epidemiological data on SCI in China are sparse, especially for incidence, and are non-existent for prevalence. The available data were mostly extracted from hospital records and community studies were limited. Research has mainly concentrated on a few better-resourced provinces in the East and South of China, and for unknown reasons interest in the epidemiology of SCI seems to have declined in the past decades. As SCI is oftentimes preventable, epidemiological data on incidence with accurate geographical information and etiology across all Chinese provinces is a necessary requirement for a targeted implementation of preventive strategies. To this end, better collaboration between units for SCI rehabilitation and university-level public health institutes and governmental public health departments such as the Chinese Center for Disease Control and Prevention is suggested. Furthermore, SCI is not a death sentence and living a full life with SCI in the community is possible; to promote the latter, research on community outcomes and related factors needs to be developed in China. We hope that this review can serve as a wake-up call for all stakeholders involved in SCI prevention, treatment, rehabilitation, and support in China.
Data availability
All data generated or analyzed during this study are included in this published article and its supplementary information files.
References
Fitzharris M, Cripps RA, Lee BB. Estimating the global incidence of traumatic spinal cord injury. Spinal Cord. 2014;52:117–22.
Krause JS, Saunders LL. Health, secondary conditions, and life expectancy after spinal cord injury. Arch Phys Med Rehabil. 2011;92:1770–5.
McCammon JR, Ethans K. Spinal cord injury in Manitoba: A provincial epidemiological study. J Spinal Cord Med. 2011;34:6–10.
New PW, Jackson T. The costs and adverse events associated with hospitalization of patients with spinal cord injury in Victoria, Australia. Spine (Philos Pa 1976). 2010;35:796–802.
Reilly P The impact of neurotrauma on society: an international perspective. In: Weber JT, Maas AIR, editors. Neurotrauma: New Insights into Pathology and Treatment 2007. p. 3–9.
Zhou M, Wang H, Zhu J, Chen W, Wang L, Liu S, et al. Cause-specific mortality for 240 causes in China during 1990-2013: A systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet. 2016;387:251–72.
Yuan S, Shi Z, Cao F, Li J, Feng S. Epidemiological features of spinal cord injury in China: A systematic review. Front Neurol. 2018;9:683.
Chen X, Chen D, Chen C, Wang K, Tang L, Li Y, et al. The epidemiology and disease burden of traumatic spinal cord injury in China: A systematic review. [Chinese]. Chinese. J Evid-Based Med. 2018;18:143–50.
Reinhardt JD, Zheng Y, Xu G, Lu X, Yin Y, Liu S, et al. People with spinal cord injury in China. Am J Phys Med Rehabil 2017;96:S61–S65.
Campbell M, McKenzie JE, Sowden A, Katikireddi SV, Brennan SE, Ellis S, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ. 2020;368:l6890.
Downes MJ, Brennan ML, Williams HC, Dean RS. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open. 2016;6:e011458.
Ning GZ, Wu Q, Li YL, Feng SQ. Epidemiology of traumatic spinal cord injury in Asia: A systematic review. J Spinal Cord Med. 2012;35:229–39.
Wyndaele M, Wyndaele JJ. Incidence, prevalence and epidemiology of spinal cord injury: What learns a worldwide literature survey? Spinal Cord. 2006;44:523–9.
Ackery A, Tator C, Krassioukov A. A global perspective on spinal cord injury epidemiology. J Neurotrauma. 2004;21:1355–70.
Savic G, DeVivo MJ, Frankel HL, Jamous MA, Soni BM, Charlifue S. Suicide and traumatic spinal cord injury-a cohort study. Spinal Cord. 2018;56:2–6.
Yi K, Han D, Hengxing Z, Zhijian W, Lu L, Dayu P, et al. Epidemiology of worldwide spinal cord injury: A literature review. J Neurorestoratol. 2017;6:1–9.
Joseph C, Nilsson Wikmar L. Prevalence of secondary medical complications and risk factors for pressure ulcers after traumatic spinal cord injury during acute care in South Africa. Spinal Cord. 2016;54:535–9.
DeVivo M, Biering-Sørensen F, Charlifue S, Noonan V, Post M, Stripling T, et al. International spinal cord injury core data set. Spinal Cord. 2006;44:535–40.
Cieza A, Kirchberger I, Biering-Sørensen F, Baumberger M, Charlifue S, Post MW, et al. ICF Core Sets for individuals with spinal cord injury in the long-term context. Spinal Cord. 2010;48:305–12.
Biering-Sørensen F, Brown DJ, Officer A, Shakespeare T, von Groote P, Wyndaele JJ. IPSCI: A WHO and ISCoS collaboration report. Spinal Cord. 2014;52:87.
Acknowledgements
The authors wish to thank Ruiling Lian, MS and Chuanteng Feng, MPH for their support in creating Fig. 2 and former Editor in Chief of Spinal Cord Dr. Lisa Harvey for encouraging us to undertake this review.
Author information
Authors and Affiliations
Contributions
CC wrote the first draft of this manuscript and JR, WL, and CF revised the manuscript for important intellectual content. CC and WL contributed in literature search, screening and data extraction; CC, XQ, WL, CF and JR designed the study and analyzed and interpreted the data and wrote the manuscript; CC, XQ, CF, WL, and JR have approved the submitted version of the manuscript. Each author had participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Chen, C., Qiao, X., Liu, W. et al. Epidemiology of spinal cord injury in China: A systematic review of the chinese and english literature. Spinal Cord 60, 1050–1061 (2022). https://doi.org/10.1038/s41393-022-00826-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-022-00826-6
This article is cited by
-
A scoping review of post-earthquake healthcare for vulnerable groups of the 2023 Turkey-Syria earthquakes
BMC Public Health (2024)
-
Epidemiology features of traumatic and non-traumatic spinal cord injury in China, Wuhan
Scientific Reports (2024)
-
Long-term trends and risk factors of tracheostomy and decannulation in patients with cervical spinal cord Injury
Spinal Cord (2024)
-
Research Progress of Antioxidants in Oxidative Stress Therapy after Spinal Cord Injury
Neurochemical Research (2023)
