
Abstract
Study design
This is a qualitative, phenomenological study.
Objective
To investigate media portrayal of spinal cord injury (SCI) as perceived by people with SCI and explore its impact on their lived experience.
Setting
People with SCI living in Australia.
Method
Twenty-four participants, recruited using purposive and snowball sampling, completed in-depth, semi-structured interviews. Thematic data analysis followed an inductive, iterative process.
Results
Participants perceived media portrayed SCI through a narrow lens, describing how people with SCI were ‘absent’ or portrayed as either ‘pity or pedestal’. Participants said media portrayed an inaccurate picture of their lived experience that perpetuated misunderstandings of SCI. This portrayal fostered unreasonable public expectations and assumptions about living with SCI, which presented in the participant’s lives as uncomfortable interactions and inappropriate remarks. The impact for participants was a burden to explain SCI and justify what it meant for them. People with SCI would like media to portray a broader, more authentic representation of SCI to improve public understanding and to reduce the negative impact on their lives.
Conclusion
People with SCI perceived a narrow and inaccurate portrayal of SCI in media that overlooked potential quality of life, overshadowed health and life domains they considered important and reinforced the idea that SCI can be overcome. People with SCI were mostly concerned with what was absent in media portrayal of SCI rather than what was present. Action for change lies in promoting information, expanding narratives and raising awareness to diverse abilities of people with SCI.
Similar content being viewed by others


Introduction
Media can shape attitudes towards people with disability, including those with spinal cord injury (SCI) [1,2,3]. Media and disability studies propose that traditional (medicalised) framing of disability as illness, financial burden and dependence, potentially stigmatises and excludes people with disability from society [1,2,3], and negatively shapes identity for people with disability [4]. Alternatively, progressive framing considers social context, where people with disability are recognised as equal members of society, and disability is a construct of a person’s health condition and environment [1,2,3]. Progressive framing is found to positively shape identity for people with disability [4]. Analysis of portrayal of SCI in print media has found that traditional framing was most prominent, with progressive framing emerging more recently [5]. Progressive media portrayal has been shown to promote positive public perception, with greater perceived competence [6] and employability [7], of people with SCI.
Research seeking to understand media portrayal of disability as perceived by people with disability is sparse, yet highly relevant when seeking to understand the impact of media [1, 8]. Available studies include heterogeneous populations of people with disability [4, 9,10,11,12,13,14,15,16]. These studies call for greater authenticity [9,10,11], as media portrayal of disability was considered unrealistic [4, 10, 11, 14, 17], limited [10, 17], stereotyped [9,10,11,12, 14, 16] and dominated by polar narratives [4, 9,10,11, 17]. There is less consensus, however, on self-reported impact of the ‘supercrip’ frame [1,2,3]. The ‘supercrip’ is an example of a traditional media frame where people with disability are portrayed as deviating from the norm for overcoming their disability [1,2,3], and is often delivered with an inspirational tone [18]. This media frame has been received both negatively by people with disability for ‘simultaneously’ [15] raising and lowering society’s expectations for individuals with disability [15], and positively in that it showcases success [9, 15] and offers hope of societal integration [9].
SCI can happen to anyone, at any age, and generally without warning. In response to a sudden, traumatic event, people call upon established beliefs and knowledge, often shaped and absorbed by media [19]. Negative beliefs of disability have been linked to negative impacts on participation and life satisfaction among people with newly acquired SCI [20]. In the community, individual and societal attitudes are common barriers faced by people with SCI across health and life domains [21,22,23,24,25,26,27]. No identified studies have investigated how beliefs and attitudes towards SCI are informed by media, as perceived by people with SCI, and no studies have examined the impact of media on the lived experience of SCI. The aim of this study, therefore, was to answer the following research questions:
-
1.
How do people with SCI perceive media portrayal of SCI?
-
2.
How does media portrayal of SCI compare to, and impact, the lived experience of SCI?
Method
Theoretical framework
This qualitative study is founded on disability theory, where the experience of disability is understood through a social, cultural and political context [1]. The line of enquiry was performed with a phenomological lens, allowing for investigation of common meaning [28, 29] among a group of people with lived experience of a phenomena. For this study, the phenomenon investigated was the experience of media portrayal of SCI among a population of people with SCI living in the community.
Recruitment
Participants were recruited through advertisements distributed by SCI peer support networks and community health providers. Purposive sampling, combined with snowball sampling, was used to recruit people with SCI with a diverse range of characteristics (e.g., age, gender, and level and aetiology of SCI) that might reasonably influence the experience of media portrayal [28]. Recruitment ceased when no new information or themes were observed in the data [30].
Participants
Participants were adults (>18 years) with a self-reported diagnosis of SCI, who had completed inpatient rehabilitation and were living in the community. Considering the small population of people with SCI in Australia, we relied on participants who were able to offer a description of the phenomenon [28, 30] and had an interest in the topic. This was highlighted in the recruitment material. All participants provided written informed consent prior to taking part.
Interview procedure
Data were collected from in-depth semi-structured interviews performed by the lead investigator (LR) over 6 months (February to July 2020). Interviews were carried out in private, at a time convenient to the participant, for a duration of approximately 75 min. Interviews were captured via audio recordings and handwritten notes. Interviews were guided by a schedule (Table 1), based on existing literature, investigator experience and input from a consumer reference group. Media was defined as any communication offered through mass media [31] as explained by Wimmer and Dominick (2013) (Table 1). The interview schedule comprised open-ended questions, and prompts where necessary, to encourage detailed discussion of participants’ thoughts and experiences of media portrayal of SCI [30]. Accuracy in data collection was facilitated through member checking. This involved sending the interview transcript to the participant with a request to review it for accuracy. Participants were encouraged to provide any further reflections they had since the interview. Data collection and analysis were performed concurrently to identify ‘new avenues of inquiry’ [32], informing future interviews and providing richer data for analysis.
Data analysis
Thematic data analysis was guided by the method described by Creswell (2018) and followed iterative frameworks proposed by Braun and Clarke (2006) and Sundler (2019). To promote data familiarisation [29, 33], interviews were transcribed verbatim by the lead investigator (LR). Participant names were replaced with pseudonyms. Each transcript was read several times by two investigators (LR plus either NS or MS), with ideas and concepts for coding written concurrently [29, 33], along with emerging ideas [28]. Using NVivo Software (Version 12), the initial analysis highlighted ‘significant statements’ [28] made by each participant, line by line, and inductively coded according to the primary feature of each statement [28]. Inductive coding allowed for a data-driven thematic process to help remain true to the lived experience [29]. Codes were collated into themes according to relationships [33] and common thread [29]. Following an iterative process, themes were reviewed and refined, ensuring coherence and accuracy in overall meaning [33]. Themes were defined and named according to the overall ‘essence’ [33] with recognition of sub themes and significant statements [28, 29, 33].
Trustworthiness
To promote accuracy, strategies as described by Creswell (2018) were followed. Potential bias was addressed from the outset by acknowledging and clarifying the experiences and preconceived ideas of the investigators. Investigators included a physiotherapist working in a specialist SCI health service (LR); a physiotherapist with expertise in disability and qualitative research (NS); and a journalism academic with expertise in qualitative research (MS). Throughout the analysis, investigators’ thought processes were openly shared and documented, helping to maintain a transparent and inductive approach [28]. From a participant perspective, accuracy was promoted by member-checking and familiarisation with the context and culture of the study group [28]. Data triangulation was performed by involving all three investigators in data analysis and interpretation, using a reflective journal and consulting with a consumer reference group [28]. Detailed description of the setting, along with rich findings that are meaningful to understanding the lived experience of SCI, enabled transferability of findings [28]. Rigour was promoted by following a documented, systematic and transparent methodological process, which adhered to the consolidated Criteria for Reporting Qualitative Research checklist [34].
Results
Context
Twenty-four people with SCI took part (Table 2). Most participants acquired their SCI as an adult and reported having little or no knowledge of SCI at the time of injury, feeling ‘ignorant’ or ‘oblivious’, with limited understanding of disability.
‘I actually didn’t even really notice people in wheelchairs, which was bad, and I probably did assume…people in wheelchairs were more disabled than what they actually are.’ (Ben)
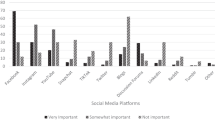
Many participants reflected how they relied on peers with SCI, rather than recalling media images, to learn about SCI. Participants said they currently used a variety of media such as radio, television (free to air and subscription), and digital and broadsheet news. Media participants most preferred or engaged with was the government funded national broadcaster (n = 17), and described themselves as cautious with forms of media that had commercial interests and/or an objective to entertain. Twenty-three participants described engaging in social media, with Facebook the most popular (n = 23).
Thematic analysis
Data analysis found two primary themes: media portrays SCI through a narrow lens and media perpetuates a misunderstanding of SCI.
Media portrays SCI through a narrow lens
Overwhelmingly, participants reported how they perceived media to portray SCI through a narrow lens. Participants described an absence of people with SCI in media, and when they were present, an absence of facts. Absence was accentuated by a perceived dichotomy of images and narratives, where people with SCI were either to be pitied, or inspiring and put on a pedestal.
Absence
Participants felt that people with SCI rarely featured in media. Alex explained when he was younger he was ‘searching for role models in media’, and Ben said, ‘every time you go out you see people in wheelchairs, so they obviously make up the community, but they’re lacking in the media’. Many participants remarked with frustration how actors without disability were employed to play characters with SCI, and how stock images were used, where it was obvious the person in the wheelchair did not have a SCI. Both scenarios reduced authenticity and heightened the sense of absence.
The absence of facts about SCI was talked about by all participants. They reported how media stories often focused on walking and frequently omitted information on the type of SCI (complete or incomplete), which they identified as having significant bearing on physical and functional outcomes.
‘very rarely have I heard that differentiation between what a complete spinal cord injury is and what an incomplete spinal cord injury is, and there is a very big difference.’ (Ruth)
Participants felt that media stories often attributed a person’s physical and functional outcomes to ‘hard work’ and ‘determination’, creating an entertaining ‘feel good’ story, but left out critical information. Ryan described ‘getting an audience is more important than having an accurate story’. In addition, participants said that there was little recognition of the variation of impairments and functional outcomes, ‘either [you] sit or stand, there is nothing in-between’ (Sean). Some participants felt tetraplegia and paraplegia were often generalised, ‘paras are the superstars, you know, getting out…and the quads are the ones…who can’t do anything’ (Dan), with absence of the ‘wide range in between’ (Brett).
Pity or pedestal
When SCI was featured in media, the resounding perception from participants was that it was portrayed by two, polar narratives: ‘you’re a sufferer and you need to be pitied…or you’re inspirational so you’re up there, on a pedestal for all to be in awe of’ (Ruth). Pity was described alongside terms such as tragic, sad and dependent, with a focus on inability (e.g., unable to leave the house, unable to work). Participants believed that media gravitated towards traumatic SCI, such as motor vehicle accidents or sporting accidents, because of the drama, neglecting other causes of SCI. Sally, whose paraplegia was the result of an infection, reflected, ‘getting paralysed in a car accident is more emotional…the trauma of everything smashing and crashing’.
The alternate media narrative was ‘pedestal’, or ‘heroes’ who are celebrated for overcoming their SCI. Inspiration was perceived as a common undertone to this narrative, ‘it’s almost as though the only story worth telling is the inspiring one’ (Heather). The most common ‘pedestal’ stories described by participants were those on walking and cure and/or therapies, as Heather said, ‘public discussion of a cure always focuses on being able to walk again’, followed by sport. Seeing the Paralympic Games in mass media was considered positive, giving para sport ‘social approval’; however, participants remarked how the Paralympic Games was the only time they saw people with SCI portrayed positively in media.
Media perpetuates a misunderstanding of SCI
Participants described a perception that media projected an inaccurate picture of SCI and highlighted that they could not recognise their lives and experiences in what was portrayed. Participants acknowledged that the dominant tragic media narrative could have meaning soon after acquiring SCI; however, many felt this should not assume their whole life, ‘I’ve been described as suffering from paraplegia, but I haven’t suffered…I’m just doing normal things with my life’ (Ruth). For Aaron, ‘It does turn your life upside down, but the misery and the sorrow photos I don’t think are accurate, because I’m happy’. Appreciating that SCI is complex, participants felt that the inaccurate picture of SCI in media perpetuated misunderstanding. Participants reported that the personal impact of this included frequent navigation of unreasonable expectations, assumptions and behaviours by others towards them, and a burden to explain SCI and justify what it meant for them.
Participants explained how polar media narratives unravelled with their interactions with others. Participants described how people assumed what their life was like. Most public assumptions they encountered were negative and centred on inabilities in function, relationships and participation, such as inability to drive, marry or work. Dan, who has tetraplegia, recognised media images of people with tetraplegia rarely acknowledged their skills and abilities and described how these negative assumptions had played out during a job interview, ‘…the guy’s realised I couldn’t move my fingers and his whole attitude changed on how I could do things…and that’s when I knew I wasn’t going to get the job’. Participants also described how some people assumed they were a Paralympian or aspired to be one; however, as Sam described ‘not everyone with a spinal cord injury has to do sport’. Dan reflected if you do not become an athlete ‘does that then make you a lesser person?’.
Many participants described how the inspirational undertone of media stories about SCI played out in their social interactions. Participants remarked how they are often told they were inspiring just for doing everyday things, said by people to be ‘nice’ or because of a lack of awareness. Alex suggested the term is ‘disabling’, and some participants described how it was a default comment projected at anyone with a disability. Most participants described feeling uncomfortable being called inspiring, and frustrated when a superficial comment was made. Participants did however provide examples of positive experiences, when inspiration was valued and founded on genuine achievement. Nick explained, ‘…they need to use it in [the correct] context’.
Participants perceived the absence of facts, focus on walking and fixation on a cure for SCI, risked false hope and misconstrued quality of life with SCI. Despite acknowledging the importance of hope and the positive role media stories can have, participants described the potential negative impact on people’s lived experience. For example, participants described that it could cause people with SCI not to engage in rehabilitation, to focus only on walking, to neglect other facets of their recovery and/or place undue pressure to work hard to walk again. Luke, who has complete paraplegia, described people’s reactions to him as ‘why aren’t you trying to walk?’. While participants expressed happiness for people who regain the ability to walk, Andrew described how people think, ‘…if you give up the hope of walking then you’ve quit’. Many participants reflected how media’s celebration of walking was frequently connected to happiness and better quality of life. However, as Ryan said, ‘you don’t have to be standing on your feet to be happy and successful, or to be productive, or to be a family person’. Dan described how media ‘portrays people who don’t walk as though they are missing out on something, and I think that’s wrong’.
Many participants described how stories on walking assumed full recovery, neglecting other SCI impairments they considered had a greater bearing on their lived experience, especially bowel and bladder management. Given the choice between walking and bowel and bladder function, participants said they would take the latter ‘every single time’ (Ruth). Participants highlighted that recovery included many things, such as learning how to do activities of daily living and forming relationships, ‘there is so much more to recovery that the media don’t talk about…’ (Andrew). In some cases, the hard work and determination that goes into learning these skills was overshadowed by the focus on walking.
Participants talked about how media’s narrow lens did not recognise various presentations of paraplegia and tetraplegia. They explained how as a result, the public often assumes that all people with paraplegia are the same and all people with tetraplegia are the same; however, as Luke described, ‘…we are all affected very differently’. Participants recognised that the popular media image of tetraplegia was of celebrity Christopher Reeve. Participants with tetraplegia who could move their arms and use a manual wheelchair described how people assumed they have paraplegia, and had their abilities questioned, their diagnosis challenged and at times encouraged to work harder. Brett, who has tetraplegia, described, ‘people think that you’re not having a go’.
Participants revealed how experience enabled them to navigate the negative expectations, assumptions and behaviours made towards them. While most felt confident to correct people’s misunderstanding of SCI, many appreciated that for others this may not be as easy. Most participants described these assumptions and interactions as a burden—‘I always feel I’m spending 5 to 10 minutes dispelling all the assumptions’ (Emma). Participants recognised people ‘mean well’ and while they felt awkward or frustrated with unwanted remarks and behaviour, they also reported letting reactions go by not wanting to deter people from engaging with people with disability again. Participants frequently reflected that when media portrayed a broader, more authentic narrative of SCI, there were ‘feelings of validation and the experience [of having a SCI] normalised’ (Heather). Maria described that ‘it would be great if [we] are portrayed as active members of the community because that’s how I would like to feel.’
Discussion
Findings from this study suggest that people with SCI perceive that media frames SCI as something that can be overcome, overlooks potential quality of life living with SCI and overshadows health and life domains they considered important. The impact of current media portrayal was a perceived burden for people with SCI to explain SCI and justify what it meant for them. Overall, this study reveals that people with SCI were mostly concerned with what was absent in media portrayal of SCI rather than what was present, and proposed that a wider lens would provide opportunity to improve public understanding of SCI, reduce perceived burden and help normalise the experience living with SCI.
Commonly, participants perceived media to frame SCI as something that can be overcome, using narratives that attribute outcomes to individual hard work and determination, with little recognition to the type of SCI or context to a person’s situation. Similar to findings from Hardin and Hardin (2004), this was received negatively by participants for potentially misappropriating society’s expectations for people with SCI. Overcoming SCI, together with a common inspiration narrative, is consistent with the ‘supercrip’ media frame [1,2,3] found in disability media studies. Participants perceived that their lives were commonly overlooked in media, with value placed on ability to walk again or becoming a Paralympic athlete, rather than on domains such as family, work, study and travel. Participants readily shared that living with a SCI has challenges; however, media portrayal that suggests walking offers a better quality of life did not reflect their experience and was not consistent with current evidence [20, 25, 35,36,37]. Framing SCI in this way ignores external factors known to influence quality of life and participation for people with SCI such as the physical environment and societal attitudes [21,22,23,24, 26, 27]. Participants described that media’s focus on walking overshadowed health and life domains considered important to them. Maximising motor function is important for people with SCI [38, 39]; however, bowel and bladder function [38, 39], sexual function, health and relationships [39] are also expressed priorities. Understanding how media portrays these domains requires further investigation; however, our findings reveal that participants want the public to understand that there is more to SCI than inability to walk, or for those who do walk, other impairments can be real. Predominately, the narrow lens as perceived by participants in this study reflected traditional media framing of SCI, which supports previous media content analysis [5] and research in other disability populations [4, 9,10,11,12,13,14,15,16].
Our findings reveal how media portrayal of SCI can have a negative impact on people’s lives. Participants described dealing with unreasonable public expectations and assumptions, manifesting as uncomfortable interactions and remarks from others. Participants identified that people meant well, but lacked awareness, as media portrayal limited the range of narratives for the public to fall back on. Participants described how experience overtime, self-assurance with their own story and an ability to identify and navigate what may be realistic and misleading in media meant the impact of media portrayal of SCI did not necessarily directly affect participants. It did however present as a burden to explain SCI and justify what it meant for them. This burden is best understood in context of the many social and environmental barriers faced by people with SCI [21,22,23,24, 26, 27], and could be considered more profound for people with less experience, that is people with newly acquired SCI, and/or people with low self-efficacy. Participants shared concerns for how media portrayal could negatively impact people with newly acquired SCI—potentially risking false hope, causing people not to engage in rehabilitation and/or placing unnecessary pressure to do better. Understanding that people can rely on preconceived ideas shaped by media at time of trauma [19], further investigation into the acute experience could help extend these findings.
Taken together, our findings point to the importance of exploring what is absent in media portrayal of SCI rather than what is present. Participants’ speculation on why media focuses on overcoming SCI and walking is supported by media literature that recognises that injury, surprise, entertainment, drama and cures are more likely to be newsworthy [40]. Our study however found that focusing on these values is detrimental to the wider community of people with SCI. People with SCI wanted media to offer broader, more authentic portrayals of SCI, supporting research that recognises that people with disability want the same of disability in media [9,10,11]. Participants believed that improved media portrayal would help bring people with SCI into the ‘public sphere’, debunk assumptions and expectations and normalise the experience of living with a disability. Acknowledging factors that go into producing different genres of media, we propose action for change sits in being cognisant of what is absent by promoting SCI facts, expanding narratives and raising awareness to the diverse abilities of people with SCI, while being aware of preferred language authenticity in images. To help mitigate any unintended consequences resulting from a shift in narrative, changes in media portrayal should also be done in consultation with people with SCI. Further research examining media industry, including different media outlets and genres, and other stakeholders, including people with SCI who produce media content [2, 3], will provide valuable context to how media portrayal of SCI is created.
A strength of this study is the previously unexplored lens to the experience of living with a SCI, in the context of media portrayal. A theoretical framework and detailed method provides transparency and repeatability. Sample size facilitated a deep exploration of the phenomenon. A limitation is that people with non-traumatic SCI and incomplete SCI, although included, were underrepresented. The majority of participants were engaged in work or study, displayed confidence in talking about their SCI and described ability to negotiate attitudes and behaviours of others. These characteristics should not be inferred for the wider population of people with SCI; however, we could speculate that these findings are more impactful for people with less experience with SCI and/or self-confidence. This study purposely defined media broadly to capture the overall experience of media portrayal and its impact. A limitation of this approach is that it does not acknowledge nuances between media genres.
Conclusion
People with SCI perceived that media portrays SCI through a narrow lens, which is inaccurate and perpetuates a misunderstanding of SCI and the lived experience. Participants believed that media’s narrow lens enforces a notion that SCI can be overcome, overlooks potential quality of life, overshadows health and life domains considered important to people with SCI and fails to acknowledge the social and environmental factors that can impact the lived experience of SCI. Findings suggest that media portrayal of SCI can foster unreasonable public expectations and assumptions about living with SCI, manifesting for people with SCI as uncomfortable interactions and inappropriate remarks from others. The implication of findings belongs in the concern for what is absent in media portrayal of SCI rather than what is present. Action for change lies in promoting SCI facts, expanding narratives and raising awareness to the diverse abilities of people with SCI, while being cognisant of preferred language and authenticity in images.
Data availability
The datasets generated and analysed during the current study are not publicly available due to the possibility of identifying information occurring in the in-depth qualitative data, but are available from the corresponding author on reasonable request.
References
Barnes C, Mercer G. Exploring disability. 2nd ed. Malden, USA: Polity Press; 2010.
Ellis K, Goggin G. Disability and the media. Palgrave Macmillan; London; 2015.
Haller BA. Representing disability in an ableist world: essays in mass media. Louisville, KY: Avocado Press; 2010.
Zhang L, Haller B. Consuming image: how mass media impact the identity of people with disabilities. Commun Q. 2013;61:319–34.
Rees L, Sherwood M, Shields N. Tragedy or over-achievement: a media analysis of spinal cord injury in Australia. Media Int Aust. 2020;00:1–15.
Kittson K, Gainforth HL, Edwards J, Bolkowy R, Latimer-Cheung AE. The effect of video observation on warmth and competence ratings of individuals with a disability. Psychol Sport Exerc. 2013;14:847–51.
Reinhardt JD, Pennycott A, Fellinghauer BAG. Impact of a film portrayal of a police officer with spinal cord injury on attitudes towards disability: a media effects experiment. Disabil Rehabilitation. 2014;36:289–94.
Thompson TL, Braithwaite DO. Handbook of communication and people with disabilities: research and application. Mahwah, N.J.: Lawrence Erlbaum Associates; 2000.
Kama A. Supercrips versus the pitiful handicapped: reception of disabling images by disabled audience members. Communications. 2004;29:447–66.
Ross K. But where’s me in it? Disability, broadcasting and the audience. Media Cult Soc. 1997;19:669–77.
Ross K. All ears: radio, reception and discourses of disability. Media Cult Soc. 2001;23:419–37.
Wilde A. Spectacle, performance, and the re-presentation of disability and impairment. Rev Disabil Stud Int J. 2010;6:34–43.
Burnett JJ, Paul P. Assessing the media habits and needs of the mobility-disabled consumer. J Advertising. 1996;25:47–59.
Sancho J. Disabling prejudice attitudes towards disability and its portrayal on television. British Broadcasting Commission; 2003. http://downloads.bbc.co.uk/guidelines/editorialguidelines/research/disabling-prejudice.pdf.
Hardin M, Hardin B. The ‘supercrip’ in sport media: wheelchair athletes discuss hegemony’s disabled hero. Sociol Sport Online. 2004;7:v7i1_1.
Hargreaves J, Hardin B. Women wheelchair athletes: competing against media stereotypes. Disabil Stud Q. 2009;29. https://dsq-sds.org/article/view/920.
Haller BA, Zhang L. Stigma or empowerment? What do disabled people say about their representation in news and entertainment Media? Rev Disabil Stud. 2014;9:19–33.
Schalk S. Re-evaluating the supercrip (Essay). J Lit Cultural Disabil Stud. 2016;10:71.
Bury M. Illness narratives: fact of fiction? Sociol Health Illn. 2001;23:263–85.
Kennedy P, Smithson E, McClelland M, Short D, Royle J, Wilson C. Life satisfaction, appraisals and functional outcomes in spinal cord-injured people living in the community. Spinal Cord. 2009;48:144.
Barclay L, McDonald R, Lentin P, Bourke-Taylor H. Facilitators and barriers to social and community participation following spinal cord injury. Aust Occup Ther J. 2016;63:19–28.
Reinhardt JD, Ruoranen K, Graf S, Horsewell J, Leiulfsrud A, Post MWM. ‘It takes two to tango …’ revisited: a qualitative study on integration and participation of people living with spinal cord injury in Switzerland. Disabil Soc. 2013;28:893–907.
Chang F-H, Liu C-H, Hung H-P. An in-depth understanding of the impact of the environment on participation among people with spinal cord injury. Disabil Rehabilitation. 2018;40:2192–9.
Joseph C, Wahman K, Phillips J, Wikmar LN. Client perspectives on reclaiming participation after a traumatic spinal cord injury in South Africa (Research report). Phys Ther. 2016;96:1372.
Pacheco Barzallo D, Gross-Hemmi M, Bickenbach J, Juocevičius A, Popa D, Wahyuni LK, et al. Quality of life and the health system: a 22-country comparison of the situation of people with spinal cord injury. Arch Phys Med Rehabilitation. 2020;101:2167–76.
Alve YA, Bontje P. Factors influencing participation in daily activities by persons with spinal cord injury: lessons learned from an international scoping review. Top Spinal Cord Inj Rehabilitation. 2019;25:41–61.
Amsters D, Schuurs S, Pershouse K, Power B, Harestad Y, Kendall M, et al. Factors which facilitate or impede interpersonal interactions and relationships after spinal cord injury: a scoping review with suggestions for rehabilitation. Rehabil Res Pract. 2016;2016:1–13.
Creswell JW. Qualitative inquiry & research design: choosing among five approaches. 4th ed. Poth CN, editor. Los Angeles: SAGE; 2018.
Sundler AJ, Lindberg E, Nilsson C, Palmér L. Qualitative thematic analysis based on descriptive phenomenology. Nurs Open. 2019;6:733–9.
Starks H, Brown Trinidad S. Choose your method: a comparison of phenomenology, discourse analysis, and grounded theory. Qualitative Health Res. 2007;17:1372–80.
Wimmer RD, Dominick JR. Mass media research. Cengage Learning; Boston MA; 2013.
Pope C, Ziebland S, Mays N. Qualitative research in health care: analysing qualitative data. Br Med J. 2000;320:114–6.
Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Res Psychol. 2006;3:77–101.
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19:349–57.
Geyh S, Ballert C, Sinnott A, Charlifue S, Catz A, Greve JMDA, et al. Quality of life after spinal cord injury: a comparison across six countries. Spinal Cord. 2012;51:322.
Hammell KW. Exploring quality of life following high spinal cord injury: a review and critique. Spinal Cord. 2004;42:491–502.
Barker RN, Kendall MD, Amsters DI, Pershouse KJ, Haines TP, Kuipers P. The relationship between quality of life and disability across the lifespan for people with spinal cord injury. Spinal Cord. 2008;47:149.
van Middendorp JJ, Allison HC, Ahuja S, Bracher D, Dyson C, Fairbank J, et al. Top ten research priorities for spinal cord injury: the methodology and results of a British priority setting partnership. Spinal Cord. 2016;54:341–6.
Simpson LA, Eng JJ, Hsieh JTC, Wolfe DL. The health and life priorities of individuals with spinal cord injury: a systematic review. J Neurotrauma. 2012;29:1548.
Harcup T, O’Neill D. What is news?. Journal Stud. 2017;18:1470–88.
Acknowledgements
The authors would like to thank the consumer reference group and all participants for offering their time and sharing their experiences to be part of this study.
Funding
This work was supported by an Australian Government Research Training Program Scholarship.
Author information
Authors and Affiliations
Contributions
LR, NS and MS contributed to the study design. LR was responsible for conducting the interviews; transcribing the interviews; data coding, analysis and interpretation; and writing the report. NS and MS contributed to data coding; analysis and interpretation; and provided critical feedback on the report.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. Ethics approval for this study was obtained from the La Trobe University Human Ethics Committee (HEC19522).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rees, L., Sherwood, M. & Shields, N. Media portrayal of spinal cord injury and its impact on lived experiences: a phenomological study. Spinal Cord 59, 504–511 (2021). https://doi.org/10.1038/s41393-021-00630-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-021-00630-8
