
Abstract
Study design
Qualitative.
Objectives
The objective of this study was to examine whether individuals with a SCI would have considered Medical-Assistance-in-Dying (MAiD) following their SCI and whether these individuals felt they would have been able to make an informed decision about this potentially permanent option early in their experience.
Setting
Manitoba, Canada.
Methods
Participants with varying neurological levels of SCI and classification were included. The time since SCI ranged from <6 months to >50 years. A focus group of five individuals was conducted first to calibrate questions. Twenty-three participants were then individually interviewed. Participants’ responses were transcribed and coded into themes.
Results
Half of the participants reported having suicidal ideation within the first 2 years of experiencing a SCI. However, no participants thought that they would have been able to make an informed decision about MAiD during this time. Most participants reported that they were able to adapt and reframe their lives to alter their views. There was higher agreement that MAiD should be available for individuals who had experienced a reframed, informed view.
Conclusion
This study indicates that people with SCI do not feel that informed decision making about ending their life can be made early after SCI despite high levels of reported suicidal ideation in that early time frame. A reframing process helps to facilitate informed decisions about living with a SCI. The reframing process is correlated with opportunities of rehabilitation, peer mentor support, and re-integration into the community.
Similar content being viewed by others

Introduction
Medical assistance in dying refers to the legal act of a health care provider directly administering a substance that causes intentional death [1]. MAiD is legal in Canada and is becoming available in an increasing number of countries around the world [1,2,3]. It is clearly legally distinguished from other end of life directives such as withdrawal of treatment or Do-Not-Resuscitate orders.
Complicating the discussion of MAiD in individuals with SCI is the fact that suicidal thoughts and actions are common during the acute phase of treatment, and dramatic emotional difficulties can be noted after the experience of a SCI [4]. A systematic review of the literature estimated that suicide was the cause of death in between 5.8% and 11% of individuals with SCI [5]. Suicide levels peaked soon after SCI, with rates being approximately five times higher than age-matched controls in the first years since a SCI [6]. These levels decreased over time following SCI [7]. The percentage of individuals reporting suicidal ideation (i.e., thoughts about committing suicide) are also quite high, with up to 50% of individuals considering suicide within the first 5 years following their injury [8,9,10]. If MAiD was available to individuals with SCI during the acute post-injury phase, it is possible that the intense emotions and grief associated with a SCI would impair an individual’s ability to make an informed decision about MAiD. Thus, an uninformed decision could be made before the person has experienced living with a SCI and has gained an understanding of what their life will be like with a SCI. The challenge for physicians is to identify the point at which an informed decision can be made. This would require physicians to be able to identify the point at which the grief reaction to the SCI does not play a major part in decision making and where the person has enough experience with a SCI to understand what the true experience of living with a SCI permanently will be like.
To our knowledge, no previous research has provided qualitative data describing the lived experiences and attitudes toward MAiD of the individuals with SCI themselves. The objective of this study, therefore, was to use structured interviews to examine whether individuals with a SCI would have considered MAiD following their SCI and whether these individuals would have been able to make an informed decision about this potentially permanent option to end life during their rehabilitation. This information, based on the participants’ own life experiences, provides a relevant framework from the lived perspective and these insights will assist physicians when they counsel patients and their families about MAiD.
Methods
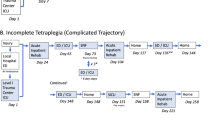
In the current research, individuals with a SCI were asked about suicidal ideation following their SCI and whether they would have considered MAiD in the acute or post-acute period if it were available. We define acute as <6 months and subacute as <2 years for the purpose of simplification of this paper, but are aware of a range of terminologies in medical literature to which these time frames may refer. Participants were asked if their opinions of both MAiD and suicide changed over the course of their rehabilitation and in their time living with SCI outside of the defined acute/subacute time window. The use of structured interviews allowed for the collection of both qualitative and quantitative data.
Participants
Five participants first took part in a focus group to calibrate the questions for the structured interviews. Twenty-three individual interviews then followed. All participants were members of a local SCI non-profit organization and were a part of a research database where they had agreed previously to be contacted for research purposes. First, an assistant asked participants if they would like more information about this study. If they agreed, they were then contacted by the first author.
The sample size of 23 was based on the recommendations of Brod and colleagues [11] who found that at least 12 participants were necessary for reliable analysis of qualitative data. The participants varied on a number of relevant characteristics including the time since the SCI occurred, whether the SCI was complete (i.e., American Spinal Injury Association Impairment Scale (AIS) A) or incomplete (AIS B-D), the neurological level of the SCI and demographics (see Table 1). Inclusion criteria were the presence of a traumatic or non-traumatic SCI and the ability to provide informed consent. All participants were 16 years or older at the time of injury except for one participant who sustained the injury as an infant (age 1) but whose condition was stable over her life. All participants were at least 18 years or older at the time of participation.
This study received ethical approval from the university human research ethics board. A 24th participant initially consented but contact was lost without any data collection and thus was not included in collection results. All others completed the study. Individuals received an honorarium for participating in this study ($200 for focus-group participants and $75 for individual interviews).
This study was performed following established checklists for conducting qualitative research: the consolidated criteria for reported qualitative research (COREQ) [12], and the standards for reporting qualitative research (SRQR) [13] as well as the guideline for reporting involvement of patients and the public 2 (GRIPP) [14].
Design
The current research utilized a patient-reported-outcome (PRO) model in which the effects of treatments are described by the individuals who experienced them [11].
The focus group interview was conducted by the first author, who had no previous clinical interactions with the participants. The focus group purpose was to calibrate relevant questions from discussion of these sensitive topics first in a shared group setting. All focus group participants agreed that the individual interview question sets in Appendix 1 were applicable and emotionally sensitive to ask in individual interview formats.
The 23 individual interviews were conducted by the first author, and were recorded for transcription and later analysis. Nineteen interviews were conducted in person, with the remaining four being conducted over the telephone. Two participants had their significant others accompany them during the interview at their own request but the interview process consisted of a discussion with the participant alone. Because the interview questions were open-ended, the duration of the interviews varied from 0.5 to 3.0 h. Participants were instructed to provide as much detail as they wished in their responses. The interviewer did not ask questions outside of the interview question set (Appendix 1).
Participants were mailed transcripts of their responses and were asked to edit as necessary any responses to ensure that the final transcripts accurately captured the participants’ intended meaning.
Data analysis
All of the edited interview transcripts were de-identified prior to analysis. The transcripts then underwent thematic analysis in order to identify themes that emerged from the raw data itself. This Grounded Theory approach [15] is inductive in nature and allows the data to be structured based on the participants’ responses rather than on a priori themes constructed by the investigators. This approach was critical for the current study, as the primary goal was to examine suicidality and opinions of MAiD from the perspective of the person living with SCI.
This initial thematic analysis was conducted by the first author, who established a coding system that classified responses according to themes and subthemes. Preliminary operational definitions were developed for each theme and subtheme. A second investigator independently reviewed this coding system. Revisions were performed until all investigators agreed that the coding system provided accurate depictions of the data.
Two research assistants were provided training and blinded formats of assigning coding based on operational definitions prior to coding the de-identified transcripts. The assistants determined which themes and subthemes were present in each transcript; if initial coding was inconsistent this was discussed until consensus was reached. In only five instances were the coders unable to reach consensus; in these cases, the first author acted as the arbitrator.
When possible, qualitative data involving simple binary responses (e.g., Yes/No) were treated in a quantitative manner such as percentage of participants who experienced suicidal ideation. However, the emphasis was placed upon the qualitative analyses of the themes that emerged from the 23 individual interviews.
Results
The individual interviews produced information that can be treated as both qualitative and quantitative data. The quantitative data is presented in Tables 2 and 3. Given our sample size, one cannot draw conclusions from the quantitative data, thus it is simply presented in table format to help inform hypotheses of future research. The remainder of the results will focus on the qualitative data.
Twelve major themes emerged from the qualitative analysis of participants’ responses to the interview questions. Of these themes, eight are relevant to the current study of suicidality and MAiD (Appendix 2). The remaining four themes will be discussed as part of a separate paper. The eight themes are presented below, with representative quotes from participants in Table 4.
Suicidal ideation and behavior
This theme involved thoughts related to suicide and, in some individuals, a discussion of their suicide attempts. Suicidal ideation and behavior was frequently linked to fears related to a loss of independence, concerns related to a perceived inability to achieve life goals, and a feeling of letting friends or family down. It was generally discussed as part of a description of the participants’ reasoning during the acute treatment phase following a SCI.
Changing views post-SCI life: cognitive reframing
Participants stated that their understanding of what life with a SCI would be like changed over time. Many of these changes focused on gaining functional abilities that participants had assumed would not be possible immediately following their SCI. This improvement was described as occurring mostly through rehabilitation experiences that allowed a reframing of day-to-day independence following SCI.
Understanding post-SCI life: emotional reframing
This theme related to participants’ changing emotional state following a SCI. Participants reported intense negative emotions during the acute SCI time period. However, most reported increasing positivity over time. This change was linked with acquiring additional knowledge about life with a SCI from books/websites, rehabilitation professionals, peer counselors, peer mentors and from the participants’ own lived experiences. A critical factor in this emotional reframing of post-SCI life was guidance from peer mentors (i.e., other individuals with SCI) that was described as being the most relevant to this experience and contributing to a feeling of normalizing new emotions.
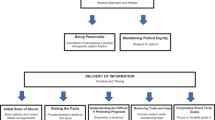
Disconnection with the medical team
A common theme in many interviews was a perceived lack of empathy from or emotional connection with the medical team. Participants felt that medical personnel were uncomfortable discussing treatment options. Many also indicated that they did not receive proper access to trained psychologists or psychiatrists during the acute and subacute phases. These perceived deficiencies increased the stress associated with the transition from being inpatients to living in the community and limited their ability to understand what to expect from a life with a SCI.
Appropriateness of MAiD to individuals with SCI
This theme related to whether each participant thought that MAiD would have been an appropriate option during the acute or subacute stage of treatment. This theme also included discussions about whether MAiD would have been appropriate in cases that were more physically severe than the participant’s own injury (e.g., tetraplegia vs. paraplegia). Some individuals reported feeling better about their SCI after seeing individuals with injuries that appeared more severe than their own, although no detectable differences to responses were noted by individuals who actually had a more severe physical injury.
Introduction of information related to MAiD
This theme related to how participants thought they would have responded to MAiD-related information if it had been presented following their SCI. It also clarified the time period in which participants felt that this information should be presented to individuals with SCI. Participants stated that they would most likely have responded with anger and/or a feeling of vulnerability had MAiD-related information been presented during the acute phase of treatment. All participants expressed that MAiD should not be discussed during this time period when they were more likely to have suicidal feelings that would need to be interpreted within a relevant context.
Lack of informed decision making
Many felt that during the acute and subacute time period, they would not have had sufficient understanding of what life with a SCI would be like to make an informed decision about MAiD. Drug side effects, emotional arousal, pain, and poor memory were also noted as factors that could alter an individual’s ability to make an informed decision about ending his or her life.
Desire for autonomy
Participants described the importance of being provided with the option to make their own informed decisions regarding their health and treatment. This desire for autonomy extended to the decision of whether to end his or her own life. Of importance, however, participants stated that informed decisions were only possible after an individual had undergone the cognitive and emotional reframing described above.
Adverse events
No documented adverse events were associated with participation in this study. One actively suicidal participant in the focus group (<2 years post-SCI) was referred to psychiatric services; however, upon follow-up, this patient no longer reported suicidal ideation.
Discussion
The current research provides important insights into the time course of suicidal ideation in individuals with SCI and the factors that may alter one’s opinion about the value of continuing life after having had a SCI. Critically, these data demonstrate that changing views of suicide over the course of rehabilitation, peer mentorship and normalization, and re-integration to community, could influence informed decision making involving MAiD. More than half of the participants in this study reported experiencing suicidal ideation at some point during the 2 years after their SCI. Consistent with previous research with individuals with other disabilities [16], this acute and subacute time period was typified by high emotional arousal, grief, fear of being a burden, anxiety about life with a SCI, and uncertainty about the future. Suicide was therefore described as being an escape from these, and other, concerns. Importantly, all participants stated that they would not have been able to make an informed decision about MAiD early after SCI without the opportunity to experience what a reframed life may be.
The quantitative and qualitative data both indicate that suicidal ideation is quite common during the acute SCI phase of treatment. Given that suicidality is difficult to quantify unless an individual attempts to commit suicide [17], it is likely that the prevalence of suicidal thoughts is underestimated. Our data indicate that discussions of this topic should be included or discussed in more depth during SCI treatment.
Participants also reported that their understanding of what life with a SCI would be like changed over time. Many participants learned to focus on what aspects of life were still possible following a SCI rather than focusing on what was lost. This “reframing” of their perspective occurred as participants experienced rehabilitation and learned that they could lead a relatively independent life despite having had a SCI. Reframing was associated with transitions from negative emotions focused on SCI-related life limitations to more positive and realistic views of their remaining life. Participants stressed that informed decision making related to MAiD was only possible once an individual had experienced this cognitive and emotional reframing and had a context in which to understand their life with SCI. Our data suggests that physicians discussing MAiD with individuals who have experienced a SCI should ensure that reframing has occurred to facilitate informed decision making regarding life with SCI.
The process of reframing was facilitated by peer mentors (i.e., other individuals with a SCI). These individuals helped reduce the negative emotions of individuals who had experienced an SCI by providing emotional support and, critically, constructive solutions for problems they might encounter. These peers, who had already undergone “reframing”, helped the participants change their focus and also normalize the described “common” early desire to end one’s life. These preliminary findings suggest that the rehabilitation process would benefit from increased interactions with SCI peer mentors.
A final question in the current research related to whether participants felt that MAiD was an appropriate option for individuals with a SCI once informed decision-making was possible. The results of this quantitative question were equivocal, with almost half of the participants being unsure of its appropriateness. Only three participants said that MAiD should definitely not be an option for individuals with SCI in the long-term. These results are consistent with earlier quantitative research [3] that demonstrates that individuals with SCI place a high value on autonomy, particularly as it relates to important medical decisions such as MAiD.
These data are particularly timely given that MAiD is now available in many countries, and that the qualification of MAiD candidates in Canada may be altered to allow people with severe physical disabilities, but without foreseeable deaths, to access. As such, health care teams may experience increased pressure to provide their patients with information related to MAiD, and both patients and their families may ask and seek relevant guidance. Indeed, previous research has already shown that end-of-life counseling is highly sought after by patients and their families following severe injuries and illness [18]. However, MAiD decision making and counseling becomes much more difficult when the individual’s prognosis—and future quality of life—are less certain [19, 20]. Our data indicate that in the case of SCI, physicians and health care teams should proceed with caution when discussing MAiD. The participants in our study stated that they would not have been able to make an informed decision during the time period immediately following their SCI and some would have reacted with anger if it was involuntarily introduced to them in this time frame. These data, which are based on the perspective of individuals with SCI, suggest that if MAiD is available for people with SCI, the counseling on end-of-living decision making such as MAiD should not occur until reframing opportunities have occurred.
Limitations
Although our sample size of 23 individual participants is considered robust for a qualitative study [11], a larger number of participants may have allowed us to detect other distinct themes in the participants’ responses. A larger sample size would also improve the reliability of our quantitative data and would have allowed us to include more proportionate demographic data (such as educational levels that more accurately reflect the population). An additional limitation involves the homogeneity of our sample; all but one of the participants received post-SCI treatment in our local hospital network, which involves a dedicated SCI rehabilitation unit. Although it is unlikely that their experiences differed widely from individuals treated in other geographical locations, it is possible that other hospitals treat suicidality in a different manner or have more or less rehabilitation, community, or psychological support. It is possible that varying degrees of rehabilitation opportunity may alter the processes identified. The homogeneity of our sample was also seen in the fact that 91% of the participants lived in urban centers. Including more rural participants or those of varying cultures would allow researchers to determine if suicidality and attitudes toward MAiD differed as a function of geography or culture. In addition, the current study did not examine whether responses were affected by the cause of the SCI. Seven of the 23 participants received third-party compensation for the injury. A larger survey-based study could examine whether suicidal ideation and beliefs about MAiD were influenced by whether the SCI was due to the participants’ actions or to the actions of another individual.
We additionally appreciate the complexities of MAiD as it may apply to those with a SCI and a more clearly anticipated imminent physical death, such as from poor pre-morbid status and severe co-morbidities. The majority of our interview participants described no imminent foreseeable death but this would be a valuable future qualitative piece. We did not track whether participants sought treatment from mental health services; these data were only included in our qualitative analyses if it was personally disclosed by the participants. Our study also did not address psychiatric diagnoses that may contribute to suicidal ideation [16, 17, 21].
Recall bias may be a limitation to our study, as we cannot quantify the degree to which participants interviewed recalled their experiences of the past accurately.
Conclusion
The current paper provides qualitative and, to a lesser extent, quantitative data related to suicidal thoughts and behaviors. It also provides novel information related to how MAiD is viewed by individuals with SCI. These data indicate that suicidal ideation is common soon after SCI, but decreases over time as individuals gain more experience and understanding of what life with a SCI will be like. The SCI participants in our study also stated that they could not have made an informed decision about MAiD during the acute/subacute stage after SCI, and none thought that making MAiD available at that time would have been appropriate. Access to relevant guidance from a lived perspective, such as through peer mentorship, and access to rehabilitation and community re-integration support were strong themes of encouraging a reframing opportunity allowing for a more informed view on life and death after SCI. Together, these data provide important guidance to physicians who must provide end-of-life counseling, and show the importance of learning from the lived experiences of individuals who have sustained severe neurological injuries such as SCI.
References
Statutes of Canada. Bill C-14: an act to amend the Criminal Code and to make related amendments to other Acts (medical assistance in dying). Chapter 3. Ottawa (CA): First Session, Forty-second Parliament, 2016 Jun 17 Royal Assent. Available from: https://laws-lois.justice.gc.ca/eng/annualstatutes/2016_3/fulltext.html.
Browne A, Russell JS. Physician-assisted death in Canada. Camb Q Health Ethics. 2016;25:377–83.
Waals EMF, Post MWM, Peers K, Kiekens C. Experiences with euthanasia requests of persons with SCI in Belgium. Spinal Cord Ser Cases 2018;4:62 https://doi.org/10.1038/s41394-018-0101-8. Published 2018 Jul 12
Salter JE, Ethans KD, Smith SD. Positive and negative affect in individuals with spinal cord injuries. Spinal Cord. 2013;51:252–6.
Kennedy P, Garmon-Jones L. Self-harm and suicide before and after spinal cord injury: a systematic review. Spinal Cord. 2017;55:2–7.
Cao Y, Massaro JF, Krause JS, Chen Y, Devivo MJ. Suicide mortality after spinal cord injury in the united states: injury cohorts analysis. Arch Phys Med Rehabil. 2014;95:230–5.
McCullumsmith CB, Kalpakjian CZ, Richards JS, Forchheimer M, Heinemann AW, Richardson EJ, et al. Novel risk factors associated with current suicidal ideation and lifetime suicide attempts in individuals with spinal cord injury. Arch Phys Med Rehabil. 2014;96:799–808.
Nam HS, Kim HR, Ha TH, Shin HI. Suicidal ideation in Korean persons with spinal cord injury. Spinal Cord. 2013;51:789–93.
Pinkerton AC, Griffin ML. Rehabilitation outcomes in females with spinal cord injury: a follow-up study. Paraplegia 1983;21:166–75.
Kishi Y, Robinson RG, Kosier JT. Suicidal ideation among patients with acute life-threatening physical illness: patients with stroke, traumatic brain injury, myocardial infarction, and spinal cord injury. Psychosomatics 2001;42:382–90.
Brod M, Tesler LE, Christensen TL. Qualitative research and content validity: developing best practices based on science and experience. Qual Health Res. 2009;18:1263–78.
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;16:349–57.
O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89:1245–51.
Staniszewska S, Brett J, Simera I, Seers K, Mockford C, Goodlad S, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ 2017;358:3453.
Strauss A, Corbin JM. Basics of qualitative research: techniques and procedures for developing Grounded Theory. 2nd ed. Thousand Oaks, CA, US: Sage Publications, Inc; 1998. p. 12.
Khazem LR. Physical disability and suicide: recent advancements in understanding and future directions for consideration. Curr Opin Psychol. 2018 Aug; 22: 20-18-22. https://doi.org/10.1016/j.copsyc.2017.07.018.
Harris EC, Barraclough BM, Grundy DJ, Bamford ES, Inskip HM. Attempted suicide and completed suicide in traumatic spinal cord injury. Spinal Cord. 1996;34:752–3.
Heyland DK, Dodek P, You JJ, Sinuff T, Hiebert T, Tayler C, et al. Validation of quality indicators for end-of-life communication: results from a multicentre survey. CMAJ 2017;189:980–9.
Balaban BR. A physician’s guide to talk about end-of-life care. J Gen Intern Med. 2000;15:195–200.
Turgeon AF, Dorrance K, Archambault P, Lauzier F, Lamontagne F, Zarychanski R, et al. Factors influencing decisions by critical care physicians to withdraw life-sustaining treatments in critically ill adult patients with severe traumatic brain injury. CMAJ 2019;191(Jun):E52–63. Doi: 0.1503/cmaj.190154
Halpern J, Arnold RM. Affective forecasting: an unrecognized challenge in making serious health decisions. J Gen Intern Med. 2008;23:1708–12.
Acknowledgements
Research assistants: Stella Entcheva, Jamie Hudon, Alyssia Wilson, Mayur Nankar. Special thanks to the Spinal Cord Injury Manitoba Inc. and Darlene Cooper and Gail Burnside. Special thanks to Dr. Jitender Sareen, department of Psychiatry University of Manitoba, who contributed to advice about a safety protocol and general feedback for the research design. Also, many thanks to our study participants who shared their personal journeys.
Funding
This work was supported by the Rick Hansen Institute for Spinal Cord Injury Research [Grant #2012–31] and the Health Sciences Centre Manitoba 2018 Staff Fellowship Award. These funding supports had no direct involvement in the research.
Author information
Authors and Affiliations
Contributions
NT is the primary author who conceived the initial study question. She performed the conceptual design, preliminary literature review, and interviews of all participants. She analyzed the data to create themes and subthemes for preparation of further independent review by research assistants. She participated in writing the paper with novel data at all layers of revision. KE is a secondary author who participated in conceptual design and overviewing the interview process, as well as obtaining grant funding. She participated in overviewing data analysis and directly contributed to all stages of writing the final paper. SDS is a secondary author who participated in conceptual design, and particularly assisted with data analysis, summation, and participated at all stages of writing the final paper.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethics statement
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
41393_2021_619_MOESM1_ESM.pdf
Supplementary File Appendix 1: Final Question Sets for Individual Interviews, Appendix 2: SCI Qualitative Research Operational Definitions of Themes and Subthemes
Rights and permissions
About this article

Cite this article
Tchajkova, N., Ethans, K. & Smith, S.D. Inside the lived perspective of life after spinal cord injury: a qualitative study of the desire to live and not live, including with assisted dying. Spinal Cord 59, 485–492 (2021). https://doi.org/10.1038/s41393-021-00619-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-021-00619-3
This article is cited by
-
Perception of facing life's challenges in patients with spinal cord injury in Iran: a qualitative study
BMC Psychology (2022)
-
Perspectives on medical assistance in dying amongst persons with traumatic spinal cord injury: a qualitative study
Spinal Cord (2022)
-
Ethical issues and dilemmas in spinal cord injury rehabilitation in the developing world: a mixed-method study
Spinal Cord (2022)
