
Abstract
Study design
Scoping review of experimental and quasi-experimental studies.
Objective
To systematically synthesize research testing the effects of leisure time physical activity (LTPA) interventions on chronic pain and subjective well-being (SWB) among adults with spinal cord injury (SCI).
Methods
Literature searches were conducted using multiple databases (Web of Science, Embase, CINAHL, Medline, PsychINFO and SPORTDiscus) to identify studies involving persons with SCI that measured and reported the effects of LTPA interventions on both chronic pain and at least one measure of SWB (e.g., affect, life satisfaction, satisfaction with various life domains). Relevant data were extracted from the studies and synthesized.
Results
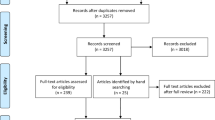
A total of 3494 articles were screened. Fifteen published articles, consisting of 12 different studies met the review inclusion criteria. Four different patterns of findings were observed regarding the effect of LTPA on chronic pain and SWB outcomes: (1) increased chronic pain, decreased SWB (1 article); (2) decreased chronic pain, improved SWB (12 articles); (3) increased chronic pain, improved SWB (1 article); and (4) unchanged levels of pain, improved SWB (1 article).
Conclusions
Results of most articles included in this scoping review suggest that LTPA interventions can reduce chronic pain and improve SWB for persons with SCI. Further research is needed to identify the mechanisms by which LTPA affects pain and SWB, in order to formulate LTPA prescriptions that maximize improvements in these outcomes.
Similar content being viewed by others

Introduction
Approximately 65% of persons with spinal cord injury (SCI) experience chronic pain from musculoskeletal or neuropathic origins, and report pain to be severe, debilitating, and worsening over time [1, 2]. Indeed, many individuals with SCI consider chronic pain to be the most disabling consequence of SCI [3]. Chronic pain is defined as any pain that lasts longer than 12 weeks, and can be categorized into three different tiers: nociceptive, neuropathic, and other [4]. People experience pain in different ways, as chronic pain exists due to a dynamic interaction of biological, psychological, and social factors unique to each person [5].
For persons with SCI who experience chronic pain, this interplay of factors often compromises subjective well-being (SWB) (e.g., increases the risk of depression or anxiety, decreases life satisfaction) [6]. SWB [7] is a multidimensional construct that encompasses various cognitive and affective components. The cognitive component includes an individual’s satisfaction with life and important life domains, whereas the affective component refers to an individual’s positive emotions (e.g., joy, pleasure) and negative emotions (e.g., anxiety, sadness; [7]). Ultimately, high SWB is characterized by high levels of positive affect and life satisfaction, and relatively few negative feelings.
Previous research among people with and without SCI demonstrates that severe disease or disability often result in physical and psychological distress that can negatively impact a person’s SWB [8, 9]. Indeed, pain has been shown to be directly related to the affective component of SWB for persons with SCI [9, 10] such that those who report lower levels of chronic pain experience higher levels of positive affect. Moreover, in studies of people with SCI and other disabilities, pain has been conceptualized as influencing SWB [11, 12]. Thus, efforts to reduce chronic SCI pain sensations could be important for improving SWB in this population [13].
Treatments to reduce pain sensations in individuals with SCI produce inconsistent results [14]. Treatment options are primarily pharmaceutical; however, in addition to eliciting debilitating side effects, pharmaceuticals result in just 50% pain reduction for only 30% of individuals with SCI-related chronic pain [1]. The refractory nature of SCI pain to extant treatments, coupled with the putative effects of chronic pain on SWB, demonstrate the need for further research to identify effective pain treatment options [15].
Leisure time physical activity (LTPA) may be an option. LTPA is defined as any physical activity an individual engages in during their free time such as wheeling in a park, playing sport, or exercising [16]. Research suggests that LTPA can reduce pain sensations for persons with SCI. For example, in a survey study of experiences with various nonmedication treatment modalities for SCI-chronic pain, participants reported pain relief to be greatest following muscle strengthening exercises [17]. Additionally, two separate exercise-training studies showed exercise to be effective in reducing shoulder pain for persons with SCI [18, 19]. Furthermore, general bodily pain was reduced for persons with SCI who participated in the exercise condition of a 9-month randomized controlled trial of an aerobic and resistance exercise-training intervention [20]. Although the tiers of SCI-related pain evaluated across these studies varied, the positive results demonstrate the potential for LTPA as a treatment option for SCI-related pain.
Research has also demonstrated significant relationships between LTPA and various aspects of SWB (e.g., life satisfaction, positive affect) for persons with SCI. Indeed, one meta-analysis showed that LTPA had small but significant negative correlations with depressive symptoms and positive correlations with overall life satisfaction [16]. Additionally, evidence reported in two literature syntheses suggests that regular participation in LTPA could enhance the overall SWB of adults with SCI [21, 22]. Collectively, these results are consistent with findings from a recent meta-analysis conducted in the general population, which reported a small but significant positive effect of LTPA on SWB [23].
Taken together, there is evidence that (a) LTPA can reduce SCI-related pain [17,18,19,20], (b) LTPA can improve SWB in people with SCI [21, 22], and (c) SCI-related pain is related to SWB [11, 24]. Additionally, some researchers have suggested that changes in pain may mediate the effects of LTPA on aspects of SWB [11, 25, 26] meaning that LTPA interventions that reduce chronic pain should also improve SWB. This possibility has received little attention in the SCI literature [11], despite the need for interventions that address these two interrelated outcomes in the context of SCI rehabilitation [27]. One way to examine the feasibility of developing LTPA interventions that will have concomitant (or mechanistic) effects on pain and SWB is to review studies that have tested the concurrent effects of an LTPA intervention on both chronic pain and SWB among persons with SCI.
The primary reason for looking at LTPA interventions that measure both chronic pain and SWB (rather than interventions that measure only chronic pain or only SWB) is that LTPA intervention protocols are notoriously inconsistent (i.e., LTPA frequency, intensity, time, type) [28] in the SCI literature. This feature makes it difficult to identify which characteristics of an LTPA protocol (e.g., what type or frequency of activity) lead to improvements in different outcomes measured across different studies. An LTPA intervention protocol that leads to improvements in one type of physiological or psychosocial outcome may not lead to changes in another physiological or psychosocial outcome [22, 28], highlighting the importance of looking at the concurrent effects of a particular LTPA intervention on outcomes that may be interrelated or have a mechanistic relationship. Therefore, to advance an understanding of (a) whether the effects of a particular LTPA intervention on SWB may be related to/mediated by changes in pain, and (b) characteristics of LTPA interventions that may lead to changes in both chronic pain and SWB, a scoping review was conducted of studies that tested the effects of LTPA interventions on both pain and SWB, concurrently.
The overarching purpose of this scoping review was to systematically catalog and synthesize studies that tested the effects of an LTPA intervention on both chronic pain and SWB among persons with SCI. By focusing only on studies that included both outcome measures, our goal was to shed light on the nature of the relationship between these two outcomes in response to LTPA interventions; specifically, whether LTPA has concomitant effects on pain and SWB. Cataloging characteristics of LTPA interventions in relationship to chronic pain and SWB outcomes is critical for developing LTPA prescriptions to improve these outcomes in people with SCI and to optimize rehabilitation outcomes.
Methods
Protocol design
Arksey and O’Malley’s 5-stage scoping review methodological framework [29] guided this scoping review. The protocol for this review was published on Open Science Framework on 2019/05/10 and can be found here: https://doi.org/10.17605/OSF.IO/3H2P6.
Stage 1: identify the research question
The primary research question for this scoping review was: “What is known from previous literature regarding the effects of LTPA interventions on both chronic pain and SWB among individuals with SCI?”
Stage 2: identify relevant studies
The search strategy was developed with input from the entire authorship team. An experienced Health Sciences Librarian provided guidance regarding search criteria specific to each database. Examples of the search terms included: physical activity, exercise, nociceptive pain, neuropathic pain, affect, satisfaction. Included terms were identified and adapted from a previously conducted meta-analysis of the SCI, SWB and LTPA literature [16]. The complete search strategy is available online: (https://doi.org/10.17605/OSF.IO/3H2P6). The first author (KRT) conducted searches within the following databases: MEDLINE, EMBASE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycInfo, SportDiscus, and Web of Science. The search strategy was not limited based on year of publication, and the initial search was completed on January 20, 2019. Following completion of each search, citations were exported to an online management system (RefWorks™, ProQuest LLC, Michigan, USA) where article duplicates were identified and removed. Reference lists of included studies and related systematic reviews were hand searched to identify additional, relevant citations.
Stage 3: study selection
The inclusion criteria for this scoping review were: (1) experimental or quasi-experimental research designs (e.g., randomized controlled trials, pre–post test studies) that (2) evaluated the effects of LTPA participation by human adults (18+) with SCI > 1 year. LTPA was defined as physical activity an individual engages in during their free time [16]. Similar to a previous meta-analysis of studies of LTPA and SWB in people with SCI [16], we included studies that evaluated the effects of sport participation, or activities which aimed to improve or maintain one or more components of physical fitness (e.g, aerobic fitness, muscular strength/endurance, body composition). Third, studies had to have evaluated, and reported the effects of LTPA on both chronic pain and SWB. SWB was defined according to Diener’s definition of the construct, which explains SWB as including affect, life satisfaction, and satisfaction with various life domains [7]. This tripartite conceptualization of SWB can be measured with reliable and valid self-report scales and has been widely studied within and between cultures [30]. Individuals may vary in the life domains that are most important to them, making SWB responsive to different predictors according to personal values or cultural factors [31]—yet international surveys also exhibit consistency in people’s views of a good or satisfying life [32]. As such, studies that included measures of positive and negative affect, life satisfaction, and satisfaction with a variety of important life domains (e.g., social relationships) were included.
Articles were excluded if the studies: (1) did not provide original quantitative data (e.g., systematic reviews), (2) implemented LTPA in conjunction with another intervention (e.g., LTPA and cognitive behavioral therapy), (3) had not undergone full peer-review (e.g., conference proceedings, abstracts, theses), (4) were published in languages other than English. This scoping review incorporated a two-staged article screening process: (1) a title and abstract review, and (2) a full text review. Stage 1 involved the primary and secondary (SVCL) review authors independently screening 3494 titles and abstracts yielded by the search against the inclusion criteria.
As the literature became better understood throughout the title and abstract screening process, inclusion criteria were updated for the full text review (i.e., stage 2). These criteria modifications coincide with the iterative process of scoping reviews [29]. Stage 2 involved KRT and SVCL both independently screening all full text articles against the inclusion criteria. Throughout stages 1 and 2, KRT and SVCL disagreed on five articles for inclusion, indicating >99% agreement. After short discussion, all articles were agreed upon by consensus. Although RBS and KMG were allocated as mediators prior to screening (in case of disagreements), KRT and SVCL resolved disagreements without needing to involve RBS or KMG. Figure 1 displays an overview of the scoping review article inclusion/exclusion process.

Note: An asterisk indicates reference lists of included articles, or related systematic reviews; double asterisks indicate reasons for exclusion: Not SCI-specific (n = 14); studies that were not experimental or quasi-experimental (n = 16); duplicate (n = 2); did not evaluate all three constructs (n = 8); rehabilitation intervention, not a LTPA intervention (n = 2); combined intervention (n = 5).
Stage 4: charting the data
Using a data abstraction tool that was co-developed by the research team, KRT charted data from each article (Table 1). The following information was extracted from each article: author(s), year of publication, title, study design, study location (community versus lab), participant age, participant activity status (physically active versus inactive at study baseline), years post injury, level of injury, total number of participants, LTPA intervention characteristics (i.e., type, duration, frequency, intensity), pain information (i.e., type, pain measurement tool) and key outcomes, and SWB information (i.e., construct, measurement tool) and key outcomes.
RBS reviewed the completed data abstraction spreadsheet to corroborate that data were extracted accurately. The senior author (KMG) provided guidance on categorizing the types of LTPA to be consistent with previous reviews [16]. Of the authorship team members, the fourth author (DW) possesses the greatest expertise on SWB and consulted with KRT to assist with SWB data abstraction. This strategy maximized appropriate classification of SWB constructs.
Stage 5: collating, summarizing, and reporting the results
Systematic (aggregate) reviews typically aim to combine similar types of data and prioritize a homogenous set of studies, whereas scoping (configurative) reviews typically prioritize the identification of patterns provided by heterogeneity across studies [33]. Indeed, scoping reviews are usually undertaken to provide a descriptive account of all existing research evidence in an area, and to describe the breadth of concepts underpinning a research area. Scoping reviews are often conducted to facilitate formulation of future research priorities rather than to assess the quality of individual studies [34]. Thus, the authors did not perform a quality appraisal for the included studies. A scoping review methodology, rather than a meta-analysis, was employed given the limited number of intervention studies in the LTPA-chronic pain-SWB literature among persons with SCI, coupled with the heterogeneity of methods used in the interventions. Data were summarized using narrative synthesis, which relies on the use of words and text to explain the findings of the synthesis [35]. Ultimately, the effects of LTPA on chronic pain and SWB among adults with SCI, documented during the charting process, formed the results of this scoping review.
Results
Articles retrieved
The search yielded a total of 3494 citations. After screening for inclusion/exclusion criteria, and hand searching included articles and related systematic reviews, 15 published articles, consisting of 12 different studies, were included in this review. Figure 1 outlines the study selection process, while Table 1 provides details of relevant data extracted from each article. Specific characteristics of each article (e.g., measures used, results, statistical significance) are outlined in Table 1 and Fig. 2. This scoping review reports the results of included articles, by summarizing the patterns of change in SCI-chronic pain and SWB following LTPA participation. A graphical representation of changes in pain and SWB, reported by each included article, is presented in Fig. 2.

Note:  = improved.
= improved.  = worsened.
= worsened.  = no change. *p < 0.05.
= no change. *p < 0.05.
Article characteristics
Five articles were published prior to 2010 and all other articles were published between 2011 and 2018. Specifically, articles were published in 2003 (n = 2) [11, 20], 2004 (n = 1) [36], 2006 (n = 1) [18], 2007 (n = 1) [37], 2011 (n = 2) [19, 38], 2012 (n = 1) [39], 2015 (n = 1) [40], 2016 (n = 2) [41, 42], 2017 (n = 2) [43, 44], and 2018 (n = 2) [45, 46]. There was a total sample of 238 participants with SCI included within the studies (Mean = 19.9 ± 15.9; Median = 12.5), consisting of both physically active and inactive individuals. Regarding injury level, 51 persons reported tetraplegia, 176 individuals reported paraplegia, and 11 persons did not report their injury level.
Research was conducted in five countries, with the majority of the articles written by authors in Canada (n = 7) [11, 20, 36, 37, 40, 43, 46] and the United States (n = 5) [18, 19, 38, 41, 42]. Articles reported on studies that implemented experimental designs (i.e., randomized controlled trials; n = 8) [11, 18,19,20, 36, 38, 43, 45], and quasi-experimental designs (i.e., pre–post test, n = 7) [39,40,41,42, 44,45,46].
A total of four different types of LTPA were described across the 15 included articles. These included individually prescribed exercise (n = 11) [11, 18,19,20, 36,37,38,39, 42, 44, 45], yoga (n = 2) [40, 43], community based, self-selected physical activity (n = 1) [46], and seated tai-chi (n = 1) [41]. A minimum of one LTPA characteristic was prescribed to participants in each study. Study duration of LTPA protocols ranged from an acute study (1 session) [44], to a 9-month exercise-training intervention [20]. LTPA session frequency ranged from 1 to 4 times per week (Mean = 2), with sessions lasting between 5 and 120 min.
Pain and SWB constructs
Studies evaluated 27 SWB constructs, using 32 different questionnaires. Three different types of pain were independently evaluated using 9 different questionnaires: general bodily pain (n = 7) [11, 20, 36, 37, 40,41,42], shoulder pain (n = 4) [18, 19, 38, 42], and neuropathic pain (n = 2) [44, 46]. Specifically, general bodily pain and neuropathic pain were both evaluated using 4 separate measures, while shoulder pain was evaluated using 2 measures, and nociceptive pain was evaluated using 1 measure. Multiple types of pain were evaluated within two studies: (1) neuropathic, nociceptive, and shoulder pain [39], and (2) shoulder pain and general bodily pain [45]. Based on the lack of specificity of pain definitions within SCI literature, pain was categorized as “general bodily pain” if it was not defined as nociceptive, neuropathic, or visceral [4].
Key findings
Fifteen articles reported on the effects of LTPA on chronic pain and SWB for persons with SCI. Within these articles, four different patterns of findings emerged regarding changes in chronic pain and SWB outcomes in response to a LTPA intervention. These patterns are discussed separately in the following sections.
Increased pain, decreased SWB
One article reported increased levels of general bodily pain, and decreased subjective well-being following participation in an exercise program. Specifically, increased levels of general bodily pain and pain catastrophizing, combined with decreased mindfulness, and more negative affect were reported following participation in an 8-week yoga program [40].
Increased pain, improved SWB
One article reported that following a 6-week yoga program, participants’ average general bodily pain increased, while their overall anxiety-depression, self-compassion, and levels of mindfulness improved [43].
Decreased pain, improved SWB
Decreased levels of pain, and improved aspects of SWB were reported in 12 articles. Specifically, five articles reported a decrease in general bodily pain. Decreased general bodily pain and depressive symptoms, and an overall improvement in quality of life were reported by Hicks et al. [20], following a 9-month progressive aerobic and resistance exercise-training intervention. In a secondary analysis of the 3-month data from that trial [11], exercise condition participants reported decreased bodily pain and stress compared to the control group, coupled with improved quality of life and satisfaction with physical function. Further, pain was shown to mediate exercise-related changes in depressive symptoms. Another secondary analysis of this 9-month randomized controlled trial [36] revealed that although bodily pain and stress decreased for participants in the exercise group, perceived pain mediated exercise-related changes in stress levels but did not mediate the effects of exercise on depression. Reduced general bodily pain, and improved emotional well-being were also reported following a 12-week, seated tai-chi exercise program [41]. Furthermore, in an acute study, following 15–45 min of body-weight supported treadmill training, participants reported decreased bodily pain and improved feelings of pleasure [37].
Shoulder pain was also shown to improve following four exercise programs. Specifically, participants reported decreased shoulder pain and improved satisfaction with their shoulders following an 8-week home-based exercise program [18]. Further, one primary [19] and one secondary [38] analysis of data from the same study demonstrated that a 12-week home-based exercise-training program led to decreased shoulder pain and improved quality of life. Last, Wilbanks et al. [42] reported decreased levels of shoulder pain and improved quality of life following a 6-week aerobic exercise-training program.
Two studies evaluated acute changes in neuropathic pain related to LTPA. First, following at least one of two bouts of self-selected, community-based exercise performed within a single week, participants reported decreased neuropathic pain and improved feelings of pleasure [46]. Second, neuropathic pain, depressive symptoms, and anger decreased following a single session of exercise that involved wheelchair propulsion [44].
One study measured changes in multiple tiers [4] of pain following an aerobic exercise program [39]. Participants reported decreased musculoskeletal and neuropathic pain, and improved quality of life following a 10-week aerobic exercise program [39].
Unchanged levels of pain, improved SWB
One 6-week home-based aerobic exercise program did not impact shoulder or general bodily pain for participants [45]. However, self-efficacy and quality of life were improved at the end of this program.
Discussion
This scoping review aimed to catalog research evidence in which the effects of LTPA on both chronic pain and SWB were evaluated among persons with SCI. Through a systematic process, 15 relevant articles were identified. By synthesizing this literature, we were able to identify patterns of change in chronic pain and SWB outcomes in response to LTPA interventions. Our review has also brought to light priorities that should be addressed in future studies of the effects of LTPA on pain and SWB.
The effects of LTPA on chronic pain and SWB
Individuals with SCI often avoid physical activity in fear of increasing their levels of pain [47]. However, the majority of articles reviewed (n = 12) [11, 18,19,20, 36,37,38,39, 41, 42, 44, 46] reported that LTPA actually led to a decrease in participants’ pain levels. Of these 12 articles, each article also reported improvements in SWB constructs (e.g., feelings of pleasure, stress levels). These findings are critical, as they demonstrate that various forms of LTPA may both reduce pain sensations and improve multiple aspects of SWB for adults with SCI.
Given the designs of the reviewed articles, no inferences can be made regarding the causal directionality of the relationships between chronic pain and SWB following LTPA interventions. However, previous research has situated changes in pain as a mechanism for LTPA-induced changes in SWB among persons with SCI. For example, in one study, pain reduction was identified as a statistical mediator through which exercise improved life satisfaction and depressive symptoms [11]. Additionally, exercise-induced reductions in perceived pain statistically mediated changes in stress levels [36]. Collectively, these articles provide preliminary evidence of a mechanistic relationship whereby LTPA participation can lead to a reduction in pain and, in turn, improvements in SWB.
Three other patterns of changes in pain and SWB emerged across four reviewed articles (e.g., increased pain, decreased SWB), in addition to the concurrent beneficial effects of LTPA on chronic pain and SWB. These varying patterns highlight the differential impacts that LTPA may have on pain and SWB for persons with SCI. Given the variety of LTPA protocols implemented within each article, it is difficult to explain why these different findings emerged, and to compare findings between studies. Notably, however, yoga was the only ‘type’ of LTPA that consistently led to increased pain sensations [40, 43]. Inconsistencies between LTPA protocols also make it challenging to deduce which specific characteristics of LTPA protocols are most effective for improving pain and SWB. Two standardized exercise guidelines have been developed to improve overall fitness and cardiometabolic health for persons with SCI. For cardiorespiratory fitness and muscle strength benefits, adults with SCI should engage in: (a) 20 min of moderate-to-vigorous intensity aerobic activity two times per week, and (b) strength training two times per week, consisting of three sets of 8–10 repetitions of each exercise for each major muscle group [46]. For cardiometabolic health benefits, adults with SCI should engage in at least 30 min of moderate-to-vigorous intensity aerobic exercise three times per week [48]. However, the effect of following these exercise guidelines on chronic pain and SWB is not yet known. Moving forward, it is critical for researchers to prescribe exercise protocols that adhere to these standardized, scientific SCI Exercise Guidelines [48] to allow for comparison of findings between studies, and to identify whether adhering to these guidelines can also beneficially impact chronic pain and SWB for persons with SCI.
In addition to a lack of consistency in LTPA characteristics, the articles reviewed were also inconsistent in how pain was categorized and measured. Indeed, reviewed articles rarely specified the tier(s) of pain [4] being measured (Table 1). For example, eight articles categorized the type of pain as ‘general bodily pain’ [11, 20, 36, 37, 40, 41, 43, 46] rather than musculoskeletal, neuropathic, visceral, or other [4]. A comprehensive, mechanism-based, SCI pain classification tool (i.e., International Spinal Cord Injury Pain Classification) [49] was developed in 2012. This SCI pain classification tool was developed by consensus of clinicians and researchers with expertise in SCI-chronic pain, and has been shown to be applicable for persons with SCI during study development and participant screening [49]. Although seven of the reviewed articles were published following the development of the International SCI Pain Classification tool (i.e., >2012), only three articles used this tool and specifically categorized pain according to these tiers. Despite the inconsistencies in pain measurement tools, LTPA was effective for reducing all three tiers of pain [4]. Given the different mechanisms responsible for each type of pain, future studies must prioritize proper classification of SCI pain in order to identify specific LTPA protocols that impact each pain tier [4].
SWB constructs were also measured inconsistently using a variety of questionnaires. Twenty-seven SWB constructs were evaluated in the reviewed articles, using 32 different questionnaires. Given the multidimensional nature of SWB, it is unsurprising that multiple measures have been used to evaluate SWB constructs. However, many of these measures lack SCI-specificity. For example, quality of life was evaluated in eight articles using six different measures, while only two of these studies [39, 42] incorporated SCI-specific quality of life measures. Evidence supports the reliability and validity of quality of life measures for persons with SCI [50]. Using these SCI-specific tools standardizes data collection and allows for: (a) comparing results across published SCI-studies, and (b) comparing the effectiveness of exercise with the effectiveness of other SWB-enhancing interventions. It is crucial that future studies incorporate SCI-specific SWB measures to ensure that questionnaire items are relevant and applicable to persons with SCI. Further, incorporating SCI-specific SWB measures may help identify LTPA protocols that improve SWB for persons with SCI. It is important to note, however, that not one article included within this scoping review evaluated SWB in its entirety. Articles included in this review primarily included measures of life satisfaction (e.g., quality of life), but not satisfaction with various life domains, nor affective constructs. To be consistent with the definition of SWB [7], investigators should include measures of affective constructs, together with general life- and life-domain satisfaction.
Strengths and limitations of the scoping review
This scoping review has multiple strengths including the rigorous, systematic methods used for searching, evaluating and cataloging the research evidence guided by the expertise of a Health Sciences Librarian; the synthesis of pain and SWB constructs observed across studies; identification of important issues and gaps in the literature; and the provision of critical next steps for improving future LTPA, chronic pain and SWB research among individuals with SCI. However, limitations exist.
First, classifying LTPA protocols as ‘exercise’ or ‘physical activity’ is helpful for distinguishing between different ‘types’ of LTPA, but does not account for all variations in LTPA characteristics that could influence pain and SWB (e.g., intensity, duration, frequency). Second, we categorized the ‘tiers’ of pain, and ‘constructs’ of SWB measured in each study based on information provided in the articles. Another review team may have classified some pain and SWB outcomes differently, particularly when measure descriptions were vague. Third, the search strategy was limited to the English language, which may have introduced a language bias and narrowed our scope of the literature. Fourth, articles were included in this scoping review if they evaluated both chronic pain and SWB changes in response to LTPA. While studies testing the effects of LTPA on chronic pain and SWB, independently, may shed light on the independent effects of LTPA on these outcomes, the reviewed studies shed light on the concurrent effects of LTPA on these outcomes. Finally, we followed a traditional scoping review approach [29] which precludes the weighting of higher versus lower quality studies in formulating conclusions.
Research recommendations
This review has highlighted important research limitations including widely varying LTPA protocols, a lack of proper pain classification within studies, and the need for consistent use of SCI-specific measures of chronic pain and SWB. First, future research should use consistent exercise protocols with SCI-specific chronic pain and SWB measures in order to accurately compare results across studies and to identify protocols that have the largest positive impact on chronic pain and SWB. Second, the results of reviewed articles suggest that LTPA-induced improvements in chronic pain and SWB often occur simultaneously. However, there is a critical need to conduct randomized controlled trials and investigate the mechanisms responsible for the effects of LTPA on chronic pain and SWB among persons with SCI (e.g., increased levels of serotonin). Rather than investigating individual outcomes, researchers must use theory- and empirically-driven models to identify constructs that explain the effects of LTPA on chronic pain and SWB outcomes [51, 52].
Conclusion
This scoping review systematically synthesized articles that tested the effects of LTPA interventions on chronic pain and SWB among adults with SCI. The majority of reviewed articles demonstrated that LTPA can simultaneously reduce chronic pain and improve SWB. These results provide direction for future research, particularly with respect to developing theory and models that explain the effects of LTPA on chronic pain and SWB, and developing LTPA interventions that maximize the positive effects of LTPA on these outcomes.
References
Finnerup NB, Johannesen IL, Sidrup SH, Bach FW, Jensen TS. Pain and dysesthesia in patients with spinal cord injury: a postal survey. Spinal Cord. 2001;39:256–62.
Dijkers M, Bryce T, Zanca J. Prevalence of chronic pain after traumatic spinal cord injury: a systematic review. J Rehabil Res Dev. 2009;46:13–29.
Siddall PJ, Loeser JD. Pain following spinal cord injury. Spinal Cord. 2001;39:63–73.
IASP. IASP taxonomy. http://www.iasp-pain.org/Education/Content.aspx?ItemNumber=1698&navItemNumber=576. Accessed 4 Aug 2019.
Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133:581–624.
Budh CN, Österåker AL. Life satisfaction in individuals with a spinal cord injury and pain. Clin Rehabil. 2007;21:89–96.
Diener E. Subjective well-being. Psychol Bull. 1984;95:542–75.
Van Campen C, Van, Santvoort M. Explaining low subjective well-being of persons with disabilities in Europe: the impact of disability, personal resources, participation and socio-economic status. Soc Indic Res. 2013;111:839–54.
Fuhrer MJ. Subjective well-being of people with spinal cord injury: relationships to impairment, disability, and handicap. Top Spinal Cord Inj Rehabil. 1996;4:56–71.
Weaver F, Guihan M, Pape TL-B, Legro M, LaVela S, Collins E, et al. Creating a research agenda in SCI based on provider and consumer input. Spinal Cord Injuries Psychosocial. Process. 2001;14:77–88.
Martin Ginis KA, Latimer AE, McKechnie K, Ditor DS, McCartney N, Hicks AL, et al. Using exercise to enhance subjective well-being among people with spinal cord injury: the mediating influences of stress and pain. Rehabil Psychol. 2003;48:157.
Hanley MA, Jensen MP, Ehde DM, Robinson LR, Cardenas DD, Turner JA, et al. Clinically significant change in pain intensity ratings in persons with spinal cord injury or amputation. Clin J Pain. 2006;22:25–31.
Burke D, Lennon O, Fullen BM. Quality of life after spinal cord injury: the impact of pain. Eur J Pain. 2018;22:1662–72.
Guy SD, Mehta S, Harvey D, Lau B, Middleton JW, O’Connell C, et al. The CanPain SCI clinical practice guideline for rehabilitation management of neuropathic pain after spinal cord: recommendations for model systems of care. Spinal Cord. 2016;54:S24.
Widerström-Noga E, Anderson KD, Perez S, Martinez-Arizala A, Cambridge JM. Subgroup perspectives on chronic pain and its management after spinal cord injury.J Pain 2018;19:1480–90.
Martin Ginis KA, Jetha A, Mack DE, Hetz S. Physical activity and subjective well-being among people with spinal cord injury: a meta-analysis. Spinal Cord. 2010;48:65.
Cardenas DD, Jensen MP. Treatments for chronic pain in persons with spinal cord injury: a survey study. J Spinal Cord Med. 2006;29:109–17.
Nawoczenski DA, Ritter-Soronen JM, Wilson CM, Howe BA, Ludewig PM. Clinical trial of exercise for shoulder pain in chronic spinal injury. Phys Ther. 2006;86:1604–18.
Mulroy SJ, Thompson L, Kemp B, Hatchett PP, Newsam CJ, Lupold DG, et al. Strengthening and optimal movements for painful shoulders (STOMPS) in chronic spinal cord injury: a randomized controlled trial. Phys Ther. 2011;91:305–24.
Hicks AL, Martin KA, Ditor DS, Latimer AE, Craven C, Bugaresti J, et al. Long-term exercise training in persons with spinal cord injury: effects on strength, arm ergometry performance and psychological well-being. Spinal Cord. 2003;41:34.
Martin Ginis KA, Jörgensen S, Stapleton J. Exercise and sport for persons with spinal cord injury. PMR. 2012;4:894–900.
Tomasone JR, Wesch NN, Ginis KA, Noreau L. Spinal cord injury, physical activity, and quality of life: a systematic review. Kinesiol Rev. 2013;2:113–29.
Buecker S, Simacek T, Ingwersen B, Terwiel S, Simonsmeier BA. Physical activity and subjective well-being in healthy individuals: a meta-analytic review. Health Psychol Rev. 2020;1–19.
Rintala DH, Loubster PG, Castro J, Hart KA, Fuhrer MJ. Chronic pain in a community-based sample of men with spinal cord injury: prevalence, severity, and relationship with impairment, disability, handicap, and subjective well-being. Arch Phys Med Rehabil. 1998;79:604–14.
Rejeski WJ, Martin K Jr, Ettinger WH, Morgan T. Treating disability in knee osteoarthritis with exercise therapy: a central role for self‐efficacy and pain. Arthritis Rheumatism. 1998;11:94–101.
Smeets RJ, Vlaeyen JW, Kester AD, Knottnerus JA. Reduction of pain catastrophizing mediates the outcome of both physical and cognitive-behavioral treatment in chronic low back pain. J Pain. 2006;7:261–71.
Kennedy P, Hasson L. The relationship between pain and mood following spinal cord injury. J Spinal Cord Med. 2017;40:275–9.
van der Scheer JW, Ginis KA, Ditor DS, Goosey-Tolfrey VL, Hicks AL, West CR, et al. Effects of exercise on fitness and health of adults with spinal cord injury: a systematic review. Neurology. 2017;89:736–45.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8:19–32.
Diener E, Heintzelman SJ, Kushlev K, Tay L, Wirtz D, Lutes LD, et al. Findings all psychologists should know from the new science on subjective well-being. Can Psychol/Psychol Can. 2017;58:87.
Diener E, Diener M. Cross-cultural correlates of life satisfaction and self-esteem. Culture and well-being. Dordrecht: Springer; 2009. p. 71–91.
Helliwell JF, Barrington-Leigh CP, Harris A, Huang H. International evidence on the social context of well-being. Cambridge, MA: National Bureau of Economic Research; 2009.
Barnett-Page E, Thomas J. Methods for the synthesis of qualitative research: a critical review. BMC Med Res Methodol. 2009;9:59.
McKinstry C, Brown T, Gustafsson L. Scoping reviews in occupational therapy: the what, why, and how to. Aust Occup Ther J. 2014;61:58–66.
Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the conduct of narrative synthesis in systematic reviews. A Prod ESRC Methods Program Version. 2006;1:b92.
Latimer AE, Ginis KA, Hicks AL, McCartney N. An examination of the mechanisms of exercise-induced change in psychological well-being among people with spinal cord injury. J Rehabil Res Dev. 2004;41:643–52.
Martin Ginis KA, Latimer AE. The effects of single bouts of body-weight supported treadmill training on the feeling states of people with spinal cord injury. Spinal Cord. 2007;45:112–15.
Kemp BJ, Bateham AL, Mulroy SJ, Thompson L, Adkins RH, Kahan JS. Effects of reduction in shoulder pain on quality of life and community activities among people living with SCI paraplegia: a randomized control trial. J Spinal Cord Med. 2011;34:278–84.
Norrbrink C, Lindberg T, Wahman K, Bjerkefors A. Effects of an exercise programme on musculoskeletal and neuropathic pain after spinal cord injury—results from a seated double-poling ergometer study. Spinal Cord. 2012;50:457–61.
Curtis KJ, Hitzig SL, Leong N, Wicks CE, Ditor DS, Katz J. Evaluation of a modified yoga program for persons with spinal cord injury. Ther Recreat J. 2015;49:97–117.
Shem K, Karasik D, Carufel P, Kao MC, Zheng P. Seated Tai Chi to alleviate pain and improve quality of life in individuals with spinal cord disorder. J Spinal Cord Med. 2016;39:353–8.
Wilbanks SR, Rogers R, Pool S, Bickel CS. Effects of functional electrical stimulation assisted rowing on aerobic fitness and shoulder pain in manual wheelchair users with spinal cord injury. J Spinal Cord Med. 2016;39:645–54.
Curtis K, Hitzig SL, Bechsgaard G, Stoliker C, Alton C, Saunders N, et al. Evaluation of a specialized yoga program for persons with a spinal cord injury: a pilot randomized controlled trial. J Pain Res. 2017;10:999–1017.
Sato G, Osumi M, Morioka S. Effects of wheelchair propulsion on neuropathic pain and resting electroencephalography after spinal cord injury. J Rehabil Med. 2017;49:136–43.
Nightingale TE, Rouse PC, Walhin JP, Thompson D, Bilzon JL. Home-based exercise enhances health-related quality of life in persons with spinal cord injury: a randomized controlled trial. Arch Phys Med Rehabil. 2018;99:1998–2006.
Todd KR, Martin Ginis KA. An examination of diurnal variations in neuropathic pain and affect, on exercise and non-exercise days, in adults with spinal cord injury. Spinal Cord Ser Cases. 2018;4:94.
Finley MA, Euiler E. Association of musculoskeletal pain, fear-avoidance factors, and quality of life in active manual wheelchair users with SCI: A pilot study. J Spinal Cord Med. 2019;1–8.
Martin Ginis KA, van der Scheer JW, Latimer-Cheung AE, Barrow A, Bourne C, Carruthers P, et al. Evidence-based scientific exercise guidelines for adults with spinal cord injury: an update and a new guideline. Spinal Cord. 2018;56:308–21.
Bryce TN, Biering-Sørensen F, Finnerup NB, Cardenas DD, Defrin R, Lundeberg T, et al. International spinal cord injury pain classification: part I. Background and description. Spinal Cord. 2012;50:413–7.
Tulsky DS, Kisala PA, Victorson D, Tate DG, Heinemann AW, Charlifue S, et al. Overview of the spinal cord injury–quality of life (SCI-QOL) measurement system. J Spinal Cord Med. 2015;38:257–69.
Sweet SN, Martin Ginis KA, Tomasone JR. Investigating intermediary variables in the physical activity and quality of life relationship in persons with spinal cord injury. Health Psychol. 2013;32:877.
Martin Ginis KA, van der Scheer JW, Todd KR, Davis JC, Gaudet S, Hoekstra F, et al. A pragmatic randomized controlled trial testing the effects of the international scientific SCI exercise guidelines on SCI chronic pain: protocol for the EPIC-SCI trial. Spinal Cord. 2020;1–9.
Funding
KRT is supported by a Joseph-Armand Bombardier Canada Graduate Scholarship (SSHRC), Killam Doctoral Scholarship (2019–2021), and WorkSafe BC Research Award (2019–2021). SVCL is supported by a Social Sciences and Humanities Research Council Doctoral Fellowship. RBS is supported by a Joseph-Armand Bombardier Canada Graduate Scholarship (SSHRC) and Gragopean Scholarship (2018–2021). KMG holds the Reichwald Family UBC Southern Medical Program Chair in Chronic Disease Prevention.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and design of this study, in addition to drafting or critically revising the article. KRT was responsible for designing the review protocol, writing the protocol and report, conducting the search, screening potentially eligible studies, extracting and analyzing data, interpreting results, writing manuscript, updating reference lists and creating tables and figures. SVCL was responsible for designing the review protocol, screening potentially eligible studies, reviewing data abstraction, and manuscript revision. RBS was responsible for designing the review protocol, reviewing data abstraction, and manuscript revision. DW was responsible for designing the review protocol, providing insight into proper SWB terminology, reviewing elements of data abstraction, and manuscript revision. KMG was responsible for designing the review protocol, assisting with writing the protocol and report, screening potentially eligible studies, analyzing data, interpreting results, manuscript revision and designing tables and figures.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Todd, K.R., Lawrason, S.V.C., Shaw, R.B. et al. Physical activity interventions, chronic pain, and subjective well-being among persons with spinal cord injury: a systematic scoping review. Spinal Cord 59, 93–104 (2021). https://doi.org/10.1038/s41393-020-00550-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-020-00550-z
This article is cited by
-
A Comparison of Neuropathic Pain Experiences Among Paralympic Versus Recreational Athletes with Spinal Cord Injury
Sports Medicine - Open (2023)
-
The effects of active upper-limb versus passive lower-limb exercise on quality of life among individuals with motor-complete spinal cord injury
Spinal Cord (2022)
-
The Impact of Residents' Leisure Time Allocation Mode on Individual Subjective Well-being: The Case of China
Applied Research in Quality of Life (2022)
