
Abstract
Study design
Knowledge translation (KT) study.
Objectives
To demonstrate how to use systematic, community-engaged methods to (1) translate the international scientific spinal cord injury (SCI) exercise guidelines into community and clinical practice guidelines, and (2) develop supporting resources.
Setting
Canada.
Methods
An expert panel of SCI researchers and stakeholders translated the guidelines and developed a supporting resource, using a KT process guided by an adapted version of the Appraisal of Guidelines, Research and Evaluation (AGREE) II Instrument. Pilot tests with end-users were conducted throughout.
Results
The panel recommended (1) the two scientific exercise guidelines be combined and presented in a single message titled “The Canadian SCI physical activity guidelines”; (2) development of an online supporting resource, with educational and motivational information presented in “layers” to address the needs and preferences of diverse end-users. The top layer presents and explains the Canadian SCI physical activity guidelines. The deeper layers include information on benefits, overcoming barriers, activity examples, safety tips, and links to existing resources. Interviews with adults with SCI (n = 8) and survey-data from end-users (n = 90) showed that the guidelines and supporting resource were perceived as clear, useful, and appropriate.
Conclusion
Using community-engaged methods, the two scientific SCI exercise guidelines were combined into one single physical activity guideline message. This KT process provides a template for groups in other countries to translate the scientific SCI exercise guidelines to their local settings using a similar systematic, community-engaged approach.
Sponsorship
Rick Hansen Institute; Social Sciences and Humanities Research Council of Canada.
Similar content being viewed by others


Introduction
A fundamental barrier to physical activity (PA) for people with spinal cord injury (SCI) is a lack of knowledge and resources about the amount and type of activity needed to achieve health and fitness benefits [1,2,3]. To address this gap, an international consortium utilized a systematic and evidence-based approach to develop two international scientific SCI exercise guidelines [4, 5]. The fitness guideline states that “for cardiorespiratory fitness and muscle strength benefits, adults with a SCI should engage in at least 20 min of moderate to vigorous intensity aerobic exercise two times per week AND three sets of strength exercises for each major functioning muscle group, at a moderate to vigorous intensity, two times per week” [5]. The cardiometabolic health guideline states that “for cardiometabolic health benefits, adults with a SCI are suggested to engage in at least 30 min of moderate to vigorous intensity aerobic exercise three times per week” [5].
Two separate guidelines were formulated to delineate the relative strength of the scientific evidence underpinning each guideline. Given the supporting evidence, the panel endorsed the fitness guideline with a “strong recommendation” and the cardiometabolic health guideline received a “conditional recommendation” [5]. Although this delineation is important to maintain the scientific integrity of the guidelines, it is not necessarily important to end-users of the guidelines.
Indeed, the guideline development panel recognized at least three challenges to implementing separate fitness and cardiometabolic health guidelines in community and clinical practice settings [5]. First, two guidelines may be confusing as users may not know which guideline to follow. Second, the word “exercise” might limit people’s thinking about opportunities to be physically active (e.g., restrict thinking to activities performed in a gym). Third, introducing a new cardiometabolic health guideline may overshadow the pre-existing fitness guideline [6], and the importance of exercising for fitness. Recognizing that these challenges could only be addressed by adapting the scientific evidence, the panel recommended distinguishing between “scientific SCI exercise guidelines” and “community and clinical practice guidelines” [5]. Specifically, the panel called for a community-engaged strategy to translate the scientific SCI exercise guidelines into guidelines that can be communicated to and used in community and clinical practice settings [5].
Community and clinical practice guidelines can address the basic informational needs regarding what types and amounts of PA people should do. However, to be maximally effective, guidelines should be presented along with evidence-informed resources that teach and encourage people with SCI how to achieve the guidelines [7, 8]. Such resources are unlikely to be implemented and used, however, unless they are tailored to local audiences and settings (i.e., presented in a manner that aligns with users’ needs and preferences) [7]. By engaging stakeholders throughout the guideline and resource development and adaptation processes [9,10,11], we can ensure that we address the preferences, concerns, and feedback from people living with SCI in a specific community. Adopting such a community-engaged approach will result in products that are meaningful for potential end-users [10, 12].
The translation of the SCI scientific exercise guidelines into community and clinical practice guidelines and the development of supporting resources should be undertaken with the same rigor as the development of the guidelines themselves [5]. The Appraisal of Guidelines Research and Evaluation II (AGREE II) instrument is useful for ensuring rigor and transparency in the clinical guideline development process [13]. An adapted version of AGREE II has been used to guide the development of evidence-informed messages and resources that support delivery of PA guidelines to the general and specific populations, including Canadians with SCI [14,15,16]. This process has not yet been applied to the new SCI scientific exercise guidelines.
Therefore, the purposes of this knowledge translation (KT) project were to demonstrate how to use systematic, community-engaged methods to (a) translate the scientific SCI exercise guidelines into community and clinical practice guidelines suitable for dissemination and implementation in the Canadian context, and (b) develop an evidence-informed supporting resource for adults with SCI living in Canada. By documenting the systematic processes for translating the SCI exercise guidelines to local settings and the development of supporting resources, this paper may serve as a template for similar KT processes in other settings.
Methods
Overview
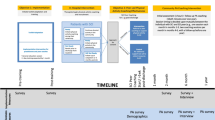
An expert panel was established to help guide the KT of the scientific SCI exercise guidelines. Figure 1 provides an overview of the project timeline with key steps including a 1-day expert panel consensus meeting and pilot tests of the translated guidelines and supporting resource with potential end-users. Our steps were guided by an adapted version of AGREE II to ensure a rigorous, systematic, and transparent approach [13]. Appendix 1 describes the original and adapted AGREE II items and how they were applied in the current project. The AGREE II instrument consists of 23 items reflecting the following six domains: scope and purpose, stakeholder involvement, rigor of development, clarity of presentation, applicability, and editorial independence. This paper is organized following these six AGREE II domains and guided by the AGREE Reporting Checklist [17] (Appendix 2).

This KT process included the translation of the guidelines and the development of an evidence-informed supporting resource. SCI PAG Spinal Cord Injury Physical Activity Guidelines.
Scope and purpose
The objectives, practical questions, target population, and potential end-users were formulated by the project leads (research lead: KMG; community lead: CBM). The expert panel members agreed upon the following statements:
Objectives: To provide an evidence-informed resource that includes user-friendly information on the scientific SCI exercise guidelines and explains how adults with SCI can implement these guidelines into their lifestyle.
Practical questions: What type of information is needed to support the dissemination and implementation of the SCI exercise guidelines in the Canadian community and clinical settings? How should this information be formatted and delivered to Canadians with SCI?
Target population: Adults with SCI (all levels of injury up to C3) who are 18–64 years old and have been injured more than 1 year, including adults with SCI who are not yet meeting the PAG.
Potential end-users: Adults with SCI, family members, friends and caregivers of adults with SCI, clinicians, practitioners, rehabilitation centres, community organizations, federal and provincial sport and health ministries, Canadian Society for Exercise Physiology, and public and private fitness centers.
Stakeholder involvement
The expert panel consisted of SCI researchers, adults with SCI, a clinician, a KT specialist, and representatives of SCI community organizations. Appendix 3 describes panel members’ expertise and roles. Panel members attended a 1-day consensus meeting, reviewed drafts of the guidelines and the supporting resource, and provided several rounds of feedback. To ensure the guidelines and resource would be relevant to individuals with SCI who do not use wheelchairs, an additional focus group discussion was conducted to identify resource preferences and views of this group. Ultimately, stakeholder engagement processes resulted in feedback from nearly 100 adults with SCI and other end-users (e.g., healthcare and fitness professionals, community organizations) (Fig. 1).
Rigor of development
Literature search
A purposive search was conducted to identify articles on (1) development and dissemination of PAG for people with SCI in a Canadian context, (2) PA participation, benefits, and predictors/correlates relevant for Canadians with SCI, and (3) development and adaptation of PAG messages. While a purposive search (instead of a systematic search) may introduce a risk of selection bias, it allows flexibility to include articles on topics relevant for our local context (i.e., Canada). Appendix 4 describes the criteria used to select articles for each of the above mentioned topics. Strengths of the evidence base included:
the use of community-engaged methods to develop the previous SCI physical activity guideline, the previous Canadian PA resource, and the SCI exercise guidelines [5, 6, 14];
the availability of Canadian-specific findings on PA predictors/correlates and preferences [18, 19], an overview of evidence-informed PA programs for people with SCI [20], and experimental evidence supporting the use of SCI-specific behavior change interventions;
the availability of systematic reviews on what should be included in effective PAG messaging [7, 8].
Limitations of the evidence base included:
insufficient evidence to support fitness or health benefits of PA for people with acute SCI [5, 21];
insufficient evidence to draft specific recommendations for different types of activities (e.g., sports) [5, 21];
a lack of SCI-specific systematic reviews on effective PAG messaging.
The multistep KT process
We used a multistep approach to translate the guidelines and develop a supporting resource:
Panel members reviewed the scientific SCI exercise guidelines articles [4, 5, 22] and the previous Canadian PA resource [14] prior to the consensus meeting.
Project lead (KMG) described the development of the scientific exercise guidelines at the beginning of the meeting.
The panel discussed and made decisions regarding the key KT issues raised by the guideline development team [5] (how to message two guidelines, whether to use the term “exercise” or “PA”).
In small working groups, panel members discussed and made recommendations for resource content (e.g., PA benefits, overcoming barriers). Working groups reported back to all members who provided further feedback.
Three panel members (KMG, FH, SG) held a debriefing meeting to refine the information and prepare next steps.
Appendix 5 includes the agenda of the 1-day consensus meeting.
The panel recommended (1) combining the two scientific exercise guidelines into a single PAG message and (2) developing an online, mobile-friendly supporting resource, with educational and motivational information. Moreover, the panel recommended replacing the word “exercise” with “PA”, because PA is broader, including both recreational and daily physical activities. The panel decided to call the translated guidelines “The Canadian Spinal Cord Injury Physical Activity Guidelines (SCI PAG)”.
After the consensus meeting, two panel members (KMG, FH) worked with a graphic designer to draft the first version of the SCI PAG. The second and final versions incorporated the panel’s recommendations and panel members’ feedback. Appendices 6 and 7 outline key recommendations and supporting evidence for the Canadian SCI PAG resource. The first author (FH) created an outline of the complete supporting resource based on the panel members’ discussions during the consensus meeting. The MoSCoW method (Must have, Should have, Could have, and Won’t have), a prioritization method commonly applied in software engineering and business management, was used to prioritize panel members’ recommendations and suggestions [23]. In the context of this project, the first author (FH) labeled panel members’ recommendations and suggestions into one of the four MoSCoW categories based on discussions during the consensus meeting (see OSF [24]). The first author (FH) worked together with a technical writer to create the content of the resource.
Panel members reviewed the SCI PAG and the supporting resource and had the opportunity to provide feedback at three time points (Fig. 1):
After drafting the first version (V1) of the SCI PAG (July 2018).
After drafting the second version (V2) of the SCI PAG and a first version of the content of the supporting resource (January 2019).
After drafting the third version of the SCI PAG (June 2019).
The first two rounds of feedback (pilot test 1 and pilot test 2) were collected via an online survey, and the last round of feedback was collected via email. The clarity, usability, and appropriateness of the SCI PAG and supporting resource were pilot tested at various stages of development with different groups of potential end-users (Fig. 1). Appendix 8 describes the pilot test procedures.
Results
Clarity of presentation
The panel recommended the development of an online resource in which the translated guidelines and supporting information is presented in “layers” to tailor the information to the needs and preferences of end-users (i.e., people who want more detailed information can go deeper into the “layers” of the website). Figure 2 depicts the layered structure of the Canadian SCI PAG resource.

The resource is available via www.sciguidelines.com.
Pilot test 1: panel members and adults with SCI
The clarity and appropriateness of the SCI PAG V1 were evaluated by expert panel members (n = 6). Panel members’ responses to survey questions were mixed with medians between 4.5 and 6.0 on 7-point Likert scales. Some panel members mentioned that the SCI PAG diagram was not clear enough and, in particular, not tailored towards adults with SCI who are not yet doing any PA. Additional telephone interviews with three adults with SCI confirmed that more information was needed to clarify the presentation and terminology used in the SCI PAG V1. Results are presented in Appendices 9 and 10.
Pilot test 2: panel members
The clarity, usability, and appropriateness of the SCI PAG V2 and the content of the supporting resource were evaluated by panel members (n = 9). Responses were positive with medians between 6.0 and 7.0 on 7-point Likert scales. Similarly, members were generally positive about the content of the supporting resource, illustrated by medians ≥ 6.0 or higher, with the exception of the items on risks of PA and information for power wheelchair users (Table 1; Appendix 11).
Pilot test 3: adults with SCI
The clarity, usability, and appropriateness of the SCI PAG V2 and supporting resource were evaluated by eight adults with SCI. As illustrated in Appendix 12, participants were positive about the clarity, usability, and appropriateness of the SCI PAG V2 and the supporting resource. Participants provided specific directions to further improve the SCI PAG and supporting resource in terms of content, layout, and navigation (Appendix 12).
Pilot test 4: potential end-users
The clarity, usability and appropriateness of SCI PAG V2 were evaluated by a diverse group of potential end-users (n = 90) including people with SCI, family members/caregivers/friends of people with SCI, healthcare and fitness professionals, and representatives of SCI community organizations via a short online survey. All survey item medians were 6.0 or 7.0 indicating that the SCI PAG were perceived as clear, useful, and appropriate for adults with SCI (Table 2).
Details on how we addressed feedback from each pilot test, including the different versions of the Canadian SCI PAG, are available via OSF [24]. The final resource is available via www.sciguidelines.com.
Discussion
This paper documents the use of systematic and community-engaged methods to translate the international scientific SCI exercise guidelines into SCI PAG suitable for dissemination and implementation in Canadian community and clinical practice settings. In response to stakeholder needs and preferences, the Canadian SCI PAG has two levels: the starting level is the SCI scientific fitness guideline and the advanced level combines the SCI scientific fitness and cardiometabolic health guidelines (Appendix 13). We also developed an evidence-informed supporting resource to help Canadians with SCI achieve the PAG.
The steps taken in our KT project are built upon the general literature on developing, updating, and adapting guidelines [10, 13, 25, 26], KT literature [9, 12, 27, 28], PAG messaging literature [7, 8, 11], and SCI-specific PAG literature [5]. Table 3 summarizes our 10-step KT approach by providing a general description of each step, an example from our KT project, and the supporting evidence. Our 10-step approach can serve as a template for other groups in other settings and other countries to translate the scientific SCI exercise guidelines to their local context. We believe that this 10-step approach will result in the development of high-quality, evidence-informed resources that are relevant and useful for end-users, and, ultimately, will have the potential to benefit local SCI communities world-wide.
Applicability
Barriers and facilitators
The panel discussed a variety of potential barriers and facilitators to the dissemination and implementation of the Canadian SCI PAG and supporting resource. Most of the discussed barriers and facilitators were described in previous literature and/or identified and described by the scientific SCI exercise guidelines panel (e.g., limited time for clinicians to discuss PA, limited equipment availability for people with SCI) [1, 3, 5]. Potential barriers specifically relevant to the Canadian SCI PAG (resource) include: (1) people may get confused between the previous Canadian resource [14] and the new resource, (2) the amount of PA that people should be doing according to the SCI PAG might overwhelm people with SCI who are not yet doing any PA, and (3) it will be hard to reach adults with SCI who are not registered with one of the provincial SCI community organizations.
Potential facilitators to overcome these barriers include: (1) we have well-established partnerships between academic researchers and non-academic partners (e.g., people with SCI, community organizations, healthcare and fitness professionals) to optimize the implementation of the new SCI PAG resource; (2) the layered structure of the resource tailors the information to different needs of end-users (e.g., special information for people who are not yet doing any PA), and (3) we plan to promote the SCI PAG resource using different strategies (e.g., social media, presentations, webinars, word-of-mouth) to reach as many end-users as possible.
Implications
Potential implications include increased knowledge and awareness of the SCI PAG among Canadians with SCI, healthcare and fitness professionals, and policymakers, which may help Canadians with SCI to become (more) active, and may help healthcare professionals to discuss and prescribe PA in clinical settings. The SCI PAG resource may also help policymakers to formulate policies on improving PA opportunities for Canadians with SCI. Our SCI PAG resource may also have implications for SCI communities outside Canada. We hope that our efforts to KT the scientific SCI exercise guidelines will inspire other groups in other countries to develop similar resources tailored to their local context, and ultimately, positively impact people with SCI around the world.
Dissemination and implementation
The SCI Action Canada lab (www.sciactioncanada.ca) launched the Canadian SCI PAG resource in August 2019. A variety of dissemination strategies are being used to further promote its uptake in different Canadian settings. Strategies include, but are not limited to the dissemination via panel members’ personal networks, social media posts, communications platforms of SCI community organizations, communication via key SCI stakeholders (e.g., SCI fitness centres, rehabilitation centers, Spinal Cord Injury Research Evidence), webinars, and conference and community presentations. Furthermore, the panel suggested disseminating the SCI PAG resource via training programs for clinicians, fitness professionals, recreational therapists, and other health professionals and through collaborations with the Canadian Society for Exercise Physiology and other rehabilitation and fitness-related organizations.
Monitoring its uptake
We will monitor the number of visits and downloads of the Canadian SCI PAG resource via Google analytics. A simple evaluation of the reach of the SCI PAG resource is incorporated in an evaluation study on the impact of the Canadian Disability Participation Project [29]. Additional resources are needed to monitor the long-term uptake of the resource in different settings across Canada and to evaluate its impact on Canadians with SCI in terms of percentage of Canadians with SCI meeting the starting and advanced levels of the SCI PAG.
KT challenges
We experienced several challenges in our KT project. The first challenge related to the presentation of the SCI PAG. The panel discussed several ideas to visually/graphically depict the SCI PAG with minimal words, while illustrating how the two guidelines are linked to different benefits and conveying a message like “Start low, and gradually work your way up”. Despite working with design experts and generating several prototypes, we were unable to create a simple graphic that clearly conveyed the SCI PAG. We decided, therefore, to present the SCI PAG as a diagram.
The second challenge was balancing between maintaining scientific integrity and creating a clear and useful resource. As described in previous sections, it took us several iterations to develop an evidence-informed diagram of the SCI PAG that was perceived as clear and useful by end-users. To illustrate, our SCI PAG V1 was clearly linked to the scientific evidence, but was not considered as clear and useful. After removing the scientific terms and simplifying the SCI PAG diagram, we were able to create an evidence-informed SCI PAG resource that maintains integrity to the original guidelines but was perceived as clear and useful by a diverse group of potential end-users.
The third challenge was developing an online resource (website). The first author (FH) built the first drafts of the website using a university platform, as this platform was free and relatively easy to work in. As the first author is not a website developer nor a graphic designer, it became challenging to develop an online resource that is accessible, easy to navigate, and interesting to look at. Fortunately, additional funding became available to hire a website developer to improve our online resource prior to the official release of the SCI PAG resource.
Future directions
Future research is needed to investigate how to develop effective PAG messages targeting the heterogeneous SCI population. Similarly, we need more research on how to implement the SCI PAG with PA promotion and behavior change programs for people with SCI, and how to develop SCI PAG resources that can effectively contribute to increasing PA levels among people with SCI.
We hope that other groups in other countries will translate the SCI exercise guidelines and create supporting resources for their SCI community and share their KT efforts. Subsequently, this may create unique opportunities to compare KT processes between different settings and countries and gain further insights into best KT practices in the context of SCI PAG resources. More specifically, an international comparative study on different SCI PAG resources might contribute to a better understanding of what SCI PAG messages and resources are preferred by different SCI communities in different settings.
Conclusion
We demonstrated how to use systematic and community-engaged methods to translate the international scientific SCI exercise guidelines into SCI PAG guidelines that are suitable for dissemination and implementation in Canadian community and clinical practice settings. The supporting evidence-informed resource provides user-friendly information on the SCI PAG to help Canadians with SCI achieve the PAG and assist healthcare and fitness professionals, organizations, and policymakers to promote PA among Canadians with SCI. We provide a template for groups in other countries to translate the international scientific SCI exercise guidelines to local settings using a similar systematic and community-engaged approach.
Data availability
The quantitative datasets generated and analysed during this study are available in the Open Science Framework (OSF) repository (https://doi.org/10.17605/OSF.IO/RYP8E). Summaries of our qualitative data as well as the steps taken to translate the guidelines and develop the supporting resource are published in supplementary files and on OSF.
References
Martin Ginis KA, Ma JK, Latimer-Cheung AE, Rimmer JH. A systematic review of review articles addressing factors related to physical activity participation among children and adults with physical disabilities. Health Psychol Rev. 2016;10:478–94.
Wolfe DL, Martin Ginis KA, Latimer AE, Foulon BL, Eng JJ, Hicks AL. Physical activity and SCI. In: Eng JJ, Teasell RW, Miller WC, Wolfe DL, A.F T, Hsieh JTC, editors. Spinal cord injury, Rehabilitation evidence. Version 3.0. 2010.
Fekete C, Rauch A. Correlates and determinants of physical activity in persons with spinal cord injury: a review using the International Classification of Functioning, Disability and Health as reference framework. Disabil Health J. 2012;5:140–50.
Goosey-Tolfrey VL, van der Scheer JW, Lexell J, Clements K, Martin Ginis KA, International SCI Exercise Guidelines Project Group. Development of scientific exercise guidelines for adults with spinal cord injury. Br J Sports Med. 2018;52:1166–7.
Martin Ginis KA, van der Scheer JW, Latimer-Cheung AE, Barrow A, Bourne C, Carruthers P, et al. Evidence-based scientific exercise guidelines for adults with spinal cord injury: an update and a new guideline. Spinal Cord. 2018;56:308–21.
Martin Ginis KA, Hicks AL, Latimer AE, Warburton DE, Bourne C, Ditor DS, et al. The development of evidence-informed physical activity guidelines for adults with spinal cord injury. Spinal Cord. 2011;49:1088–96.
Brawley LR, Latimer AE. Physical activity guidelines for Canadians: strategies for dissemination of the message, expectations for change and evaluation. Appl Physiol Nutr Metab. 2007;32 Suppl 2F:S189–205.
Latimer AE, Brawley LR, Bassett RL. A systematic review of three approaches for constructing physical activity messages: What messages work and what improvements are needed? Int J Behav Nutr Phys Act. 2010;7:36.
Gagliardi AR, Brouwers MC, Bhattacharyya OK. Guideline implementation R, application N. A framework of the desirable features of guideline implementation tools (GItools): Delphi survey and assessment of GItools. Implement Sci. 2014;9:98.
Harrison MB, Legare F, Graham ID, Fervers B. Adapting clinical practice guidelines to local context and assessing barriers to their use. CMAJ. 2010;182:E78–84.
Leone L, Pesce C. From delivery to adoption of physical activity guidelines: realist synthesis. Int J Environ Res Public Health. 2017;14:1–19.
Straus SE, Tetroe J, Graham ID. Knowledge translation in health care. Moving from evidence to practice. West Sussex, UK: John Wiley & Sons; 2013.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010;182:E839–42.
Arbour-Nicitopoulos KP, Martin Ginis KA, Latimer-Cheung AE, Bourne C, Campbell D, Cappe S, et al. Development of an evidence-informed leisure time physical activity resource for adults with spinal cord injury: the SCI Get Fit Toolkit. Spinal Cord. 2013;51:491–500.
Martin Ginis KA, Heisz J, Spence JC, Clark IB, Antflick J, Ardern CI, et al. Formulation of evidence-based messages to promote the use of physical activity to prevent and manage Alzheimer’s disease. BMC Public Health. 2017;17:209.
Latimer-Cheung AE, Rhodes RE, Kho ME, Tomasone JR, Gainforth HL, Kowalski K, et al. Evidence-informed recommendations for constructing and disseminating messages supplementing the new Canadian Physical Activity Guidelines. BMC Public Health. 2013;13:419.
Brouwers MC, Kerkvliet K, Spithoff K, Consortium ANS. The AGREE reporting checklist: a tool to improve reporting of clinical practice guidelines. BMJ. 2016;352:i1152.
Martin Ginis KA, Latimer AE, Arbour-Nicitopoulos KP, Buchholz AC, Bray SR, Craven BC et al. Leisure time physical activity in a population-based sample of people with spinal cord injury part I: demographic and injury-related correlates. Arch Phys Med Rehabil. 2010;91:722–8.
Martin Ginis KA, Arbour-Nicitopoulos KP, Latimer AE, Buchholz AC, Bray SR, Craven BC et al. Leisure time physical activity in a population-based sample of people with spinal cord injury part II: activity types, intensities, and durations. Arch Phys Med Rehabil. 2010;91:729–33.
Best KL, Arbour-Nicitopoulos KP, Sweet SN. Community-based physical activity and wheelchair mobility programs for individuals with spinal cord injury in Canada: Current reflections and future directions. J Spinal Cord Med. 2017;40:777–82.
van der Scheer JW, Martin Ginis KA, Ditor DS, Goosey-Tolfrey VL, Hicks AL, West CR et al. Effects of exercise on fitness and health of adults with spinal cord injury: A systematic review. Neurology. 2017;89:736–45.
Foulon BL, Lemay V, Ainsworth V, Martin Ginis KA. Enhancing physical activity guidelines: a needs survey of adults with spinal cord injury and health care professionals. Adapt Phys Act Q. 2012;29:329–45.
Clegg D, Barker R. Case Method Fast-Track: A RAD Approach, Addison-Wesley, Boston, MA, United States, 1994.
Hoekstra F, Ginis KM. Physical activity guidelines for adults with spinal cord injury. OSF. 2019. https://doi.org/10.17605/OSF.IO/RYP8E.
Gagliardi AR, Marshall C, Huckson S, James R, Moore V. Developing a checklist for guideline implementation planning: review and synthesis of guideline development and implementation advice. Implement Sci. 2015;10:19.
Escoffery C, Lebow-Skelley E, Udelson H, Boing EA, Wood R, Fernandez ME, et al. A scoping study of frameworks for adapting public health evidence-based interventions. Transl Behav Med. 2019;9:1–10.
Moore AE, Straus SE, Kasperavicius D, Bell NR, Dickinson JA, Grad R, et al. Knowledge translation tools in preventive health care. Can Fam Phys. 2017;63:853–8.
Brouwers M, Stacey D, O’Connor A. Knowledge creation: synthesis, tools and products. CMAJ. 2010;182:E68–72.
Hoekstra F, Martin Ginis KA, Allan V, Kothari A, Gainforth HL. Evaluating the impact of a network of research partnerships: a longitudinal multiple case study protocol. Health Res Policy Syst. 2018;16:107.
Camden C, Shikako-Thomas K, Nguyen T, Graham E, Thomas A, Sprung J, et al. Engaging stakeholders in rehabilitation research: a scoping review of strategies used in partnerships and evaluation of impacts. Disabil Rehabil. 2015;37:1390–400. https://doi.org/10.3109/09638288.2014.963705.
Acknowledgements
We would like to thank Toni Williams for making notes during the consensus meeting, Sue Grono for assisting in the development of the online resource, Adrienne Sinden for assisting with data collection, and all participants who provided feedback on the translated guidelines and supporting resource.
Funding
This study is supported by Rick Hansen Institute (since 2019 named as Praxis Spinal Cord Institute) and by Social Sciences and Humanities Research Council of Canada (grant no. 895-2013-1021).
Author information
Authors and Affiliations
Contributions
FH participated in conceptualization of the study, coordination of the study, data collection, data analyses, developing and editing drafts of the guidelines and supporting resource, writing the original draft of the manuscript, and editing drafts. CBM participated in funding acquisition, the conceptualization of the study, coordination of the study, and reviewing and editing drafts of the translated guidelines, the supporting resource, and the manuscript. SP participated in data collection, reviewing and editing drafts of the translated guidelines, the supporting resource, and the manuscript. AELC participated in funding acquisition, and reviewing and editing drafts of the translated guidelines, the supporting resource, and the manuscript. JB, MJF, JKM, JM, LM, CRW, and RW participated in reviewing and editing drafts of the translated guidelines, the supporting resource, and the manuscript. KMG participated in funding acquisition, conceptualization of the study, coordination of the study, data collection, developing and editing drafts of the guidelines and supporting resource, and writing and editing drafts of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest. Two co-authors (CMB, MJF) are members of the consumer committee of Rick Hansen Institute (since 2019 named as Praxis Spinal Cord Institute).
Ethical approval
In accordance with the regulations of the Tri-Council Policy Statement (TCPS2) governing research ethics in Canada, this study did not undergo a full ethical review as this study was not classified as research. In Canada, program evaluation and qualitative improvements studies do not fall under the auspices of the TCPS or institutional Research Ethics Boards. We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this project.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hoekstra, F., McBride, C.B., Borisoff, J. et al. Translating the international scientific spinal cord injury exercise guidelines into community and clinical practice guidelines: a Canadian evidence-informed resource. Spinal Cord 58, 647–657 (2020). https://doi.org/10.1038/s41393-019-0410-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-019-0410-1
This article is cited by
-
Implementation of the spinal cord injury exercise guidelines in the hospital and community settings: Protocol for a type II hybrid trial
Spinal Cord (2022)
-
Rethinking aerobic exercise intensity prescription in adults with spinal cord injury: time to end the use of “moderate to vigorous” intensity?
Spinal Cord (2022)
-
Facilitators and barriers to clinical practice guideline-consistent supportive care at pediatric oncology institutions: a Children’s Oncology Group study
Implementation Science Communications (2021)
-
A pragmatic randomized controlled trial testing the effects of the international scientific SCI exercise guidelines on SCI chronic pain: protocol for the EPIC-SCI trial
Spinal Cord (2020)
