
Abstract
Objectives
To evaluate the safety and efficacy transcatheter arterial chemoembolization (TACE) for the treatment of refractory gross hematuria (RGH) and urinary retention (UR) secondary to localized advanced prostate cancer (PCa).
Patients and methods
Thirty-two patients (mean age 72.5 years, range 60–89) with advanced PCa–related RGH that failed conventional therapy were included. Twenty-two of these patients had catheter-dependent due to PCa–related UR. TACE was performed with epirubicin (EPI)-eluting HepaSpheres (HS) plus intra-arterial (IA) infusion of docetaxel. Technical success, adverse events (AEs), overall survival (OS), control of RGH, removal of indwelling catheters, and local disease control, were evaluated.
Results
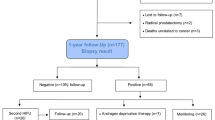
Technical success was achieved in 100% without major AEs. Mean follow up post-TACE was 27 months (range 8–56 months) with a mean OS of 30 months. GRH stopped within 5 days after TACE in all patients, 26 (86.7%) of these patients exhibited good bleeding control during a mean follow-up of 24 months; 17 (77.3%) of the 22 patients with UR had recovered spontaneous urination, 15 (88.2%) patients were catheter-free at their last follow-up with a mean of 24 months. BS was obtained in 73.3% (22/30) of patients at a mean follow-up of 29 months. At the last visit, 22 patients had a mean of 36 months follow-up and the mean percentage reduction in prostate volume was 55.5%, with a statistically different from baseline (P = 0.022). Negative biopsy results were obtained in 84.2% (16/19) of the patients at 12–47 months after TACE. Compared with baseline values, there was a significant improvements in IPSS, QoL, Qmax, and PVR (all P < 0.05).
Conclusions
TACE using EPI-eluting HS plus IA infusion of docetaxel is a safe and effective treatment option for the advanced PCa patients with GRH and UR, and it could be considered as an alternative if there was no other therapeutic choice.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout





Similar content being viewed by others


References
Gronberg H, Adolfsson J, Aly M, Nordström T, Wiklund P, Brandberg Y, et al. Prostate cancer screening in men aged 50–69 years (STHLM3): a prospective population-based diagnostic study. Lancet Oncol. 2015;16:1667–76. https://doi.org/10.1016/S1470-2045(15)00361-7.
Sanda MG, Cadeddu JA, Kirkby E, Chen RC, Crispino T, Fontanarosa J, et al. Clinically localized prostate cancer: AUA/ASTRO/SUO guideline. part i: risk stratification, shared decision making, and care options. J Urol. 2018;199:683–90. https://doi.org/10.1016/j.juro.2017.11.095.
van der Poel HG, van den Bergh RCN, Briers E, Cornford P, Govorov A, Henry AM, et al. Focal therapy in primary localised prostate cancer: The European Association of Urology Position in 2018. Eur Urol. 2018;74:84–91. https://doi.org/10.1016/j.eururo.2018.01.001.
Avellino GJ, Bose S, Wang DS. Diagnosis and management of hematuria. Surg Clin North Am. 2016;96:503–15. https://doi.org/10.1016/j.suc.2016.02.007.
Comploj E, Pycha A, Trenti E, Palermo S, Bonatti M, Krause P, et al. Transarterial embolization in the management of intractable haemorrhage. Urol Int. 2021;105:95–99. https://doi.org/10.1159/000511123.
Bilhim T, Pisco J, Pereira JA, Costa NV, Fernandes L, Campos Pinheiro L, et al. Predictors of clinical outcome after prostate artery embolization with spherical and nonspherical polyvinyl alcohol particles in patients with benign prostatic hyperplasia. Radiology. 2016;281:289–300. https://doi.org/10.1148/radiol.2016152292.
Carnevale FC, Iscaife A, Yoshinaga EM, Moreira AM, Antunes AA, Srougi M. Transurethral resection of the prostate (TURP) versus original and PErFecTED prostate artery embolization (PAE) due to benign prostatic hyperplasia (BPH): preliminary results of a single center, prospective, urodynamic-controlled analysis. Cardiovasc Interv Radio. 2016;39:44–52. https://doi.org/10.1007/s00270-015-1202-4.
Wang M, Guo L, Duan F, Yuan K, Zhang G, Li K, et al. Prostatic arterial embolization for the treatment of lower urinary tract symptoms caused by benign prostatic hyperplasia: a comparative study of medium- and large-volume prostates. BJU Int. 2016;117:155–64. https://doi.org/10.1111/bju.13147.
Salem R, Hairston J, Hohlastos E, Riaz A, Kallini J, Gabr A, et al. Prostate artery embolization for lower urinary tract symptoms secondary to benign prostatic hyperplasia: results from a prospective FDA-approved investigational device exemption study. Urology. 2018;120:205–10. https://doi.org/10.1016/j.urology.2018.07.012.
Vigneswaran G, Maclean D, Hadi M, Maher B, Modi S, Bryant T, et al. Prostatic artery embolization (PAE) and transurethral resection of the prostate (TURP) have a differential impact on lower urinary tract symptoms (LUTS): retrospective analysis of the multicentre UK-ROPE (UK Register of Prostate Embolization) Study. Cardiovasc Interv Radio. 2021;44:1095–102. https://doi.org/10.1007/s00270-021-02821-5.
Pisco J, Bilhim T, Costa NV, Ribeiro MP, Fernandes L, Oliveira AG, et al. Safety and efficacy of prostatic artery chemoembolization for prostate cancer—initial experience. J Vasc Inter Radio. 2018;29:298–305. https://doi.org/10.1016/j.jvir.2017.10.013.
Mordasini L, Hechelhammer L, Diener PA, Diebold J, Mattei A, Engeler D, et al. Prostatic artery embolization in the treatment of localized prostate cancer: a bicentric prospective proof-of-concept study of 12 patients. J Vasc Inter Radio. 2018;29:589–97. https://doi.org/10.1016/j.jvir.2018.01.766.
Malling B, Røder MA, Lindh M, Frevert S, Brasso K, Lönn L. Palliative prostate artery embolization for prostate cancer: a case series. Cardiovasc Interv Radio. 2019;42:1405–12. https://doi.org/10.1007/s00270-019-02227-4.
Peacock J, Sikaria D, Maun-Garcia L, Javedan K, Yamoah K, Parikh N. A proof-of-concept study on the use of prostate artery embolization before definitive radiation therapy in prostate cancer. Adv Radiat Oncol. 2020;6:100619. https://doi.org/10.1016/j.adro.2020.11.004.
Frandon J, Bey E, Hamard A, Mohammad H, Gonzalez S, Greffier J, et al. Early results of unilateral prostatic artery embolization as a focal therapy in patients with prostate cancer under active surveillance: cancer prostate embolisation, a pilot study. J Vasc Inter Radio. 2021;32:247–55. https://doi.org/10.1016/j.jvir.2020.10.002.
Tian W, Zhou C, Leng B, Shi H, Liu S. Prostatic artery embolization for control of gross hematuria in patients with benign prostatic hyperplasia: a single-center retrospective study in 20 patients. J Vasc Inter Radio. 2019;30:661–7. https://doi.org/10.1016/j.jvir.2019.02.008.
Ayyagari R, Powell T, Staib L, Chapiro J, Perez-Lozada JC, Bhatia S, et al. Prostatic artery embolization in nonindex benign prostatic hyperplasia patients: single-center outcomes for urinary retention and gross prostatic hematuria. Urology. 2020;136:212–7. https://doi.org/10.1016/j.urology.2019.11.003.
Tapping CR, Crew J, Proteroe A, Boardman P. Prostatic artery embolization (PAE) for prostatic origin bleeding in the context of prostate malignancy. Acta Radio Open. 2019;8:2058460119846061 https://doi.org/10.1177/2058460119846061.
Chen JW, Shin JH, Tsao TF, Ko HG, Yoon HK, Han KC, et al. Prostatic arterial embolization for control of hematuria in patients with advanced prostate cancer. J Vasc Inter Radio. 2017;28:295–301. https://doi.org/10.1016/j.jvir.2016.10.010.
Heimbach JK, Kulik LM, Finn RS, Sirlin CB, Abecassis MM, Roberts LR, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67:358–80. https://doi.org/10.1002/hep.29086.
Karalli A, Ghaffarpour R, Axelsson R, Lundell L, Bozoki B, Brismar T, et al. Transarterial chemoembolization of renal cell carcinoma: a prospective controlled trial. J Vasc Inter Radio. 2017;28:1664–72. https://doi.org/10.1016/j.jvir.2017.08.001.
Malagari K, Pomoni M, Moschouris H, Kelekis A, Charokopakis A, Bouma E, et al. Chemoembolization of hepatocellular carcinoma with HepaSphere 30–60 μm. Safety and efficacy study. Cardiovasc Interv Radio. 2014;37:165–75. https://doi.org/10.1007/s00270-013-0777-x.
Pereira K, Halpern JA, McClure TD, Lewis NA, Kably I, Bhatia S, et al. Role of prostate artery embolization in the management of refractory haematuria of prostatic origin. BJU Int. 2016;118:359–65. https://doi.org/10.1111/bju.13524.
Consensus statement: guidelines for PSA following radiation therapy. American society for therapeutic radiology and oncology consensus panel. Int J Radiat Oncol Biol Phys. 1997;37:1035–41. PMID: 9169810.
Lencioni R, Montal R, Torres F, Park JW, Decaens T, Raoul JL, et al. Objective response by mRECIST as a predictor and potential surrogate end-point of overall survival in advanced HCC. J Hepatol. 2017;66:1166–72. https://doi.org/10.1016/j.jhep.2017.01.012.
Prasad V, Sacks BA, Kraus S, Clouse ME. Embolotherapy for lower urinary tract hemorrhage. J Vasc Inter Radio. 2009;20:965–70. https://doi.org/10.1016/j.jvir.2009.04.048.
Wang MQ, Zhang JL, Xin HN, Yuan K, Yan J, Wang Y, et al. Comparison of clinical outcomes of prostatic artery embolization with 50-μm plus 100-μm polyvinyl alcohol (PVA) particles versus 100-μm PVA particles alone: a prospective randomized trial. J Vasc Inter Radio. 2018;29:1694–702. https://doi.org/10.1016/j.jvir.2018.06.019.
Sandow TA, Arndt SE, Albar AA, DeVun DA, Kirsch DS, Gimenez JM, et al. Assessment of response to transcatheter arterial chemoembolization with doxorubicin-eluting microspheres: tumor biology and hepatocellular carcinoma recurrence in a 5-year transplant cohort. Radiology. 2018;286:1072–83. https://doi.org/10.1148/radiol.2017170731.
Acknowledgements
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis. We thank Xin Ma, MD., and Xu Zhang, MD., from the Department of Urology, Chinese PLA General Hospital, for their consultations; The authors also thank Dan Feng, PhD, from the Department of Medical Statistics, Chinese PLA General Hospital, for her excellent statistical support for the manuscript. The study was supported by grants from the National Natural Science Foundation of China (82072023, 81471769) and the Central Health Research Project (W2013BJ09).
Author information
Authors and Affiliations
Contributions
Concept and design: MQW, JLZ, FD, BY, HX. Collection and assembly of data: MQW, JLZ, JXF, HYY, HKY. Data analysis and interpretation: JLZ, HYY, KC, DPF, XJZ. Initial paper writing: MQW. Critical review and final approval of paper: all authors. Accountable for all aspects of the work: MQW.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wang, M.Q., Zhang, J.L., Duan, F. et al. Prostate arterial chemoembolization for treatment of refractory hematuria and urinary retention in patients with localized advanced prostate cancer. Prostate Cancer Prostatic Dis 26, 88–95 (2023). https://doi.org/10.1038/s41391-022-00516-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41391-022-00516-7
This article is cited by
-
Prostatic Artery Embolization in Patients with Advanced Prostate Cancer: A Prospective Single Center Pilot Study
CardioVascular and Interventional Radiology (2024)
