
Abstract
Background
Cixutumumab, a monoclonal antibody targeting insulin-like growth factor I receptor, did not improve undetectable prostate-specific antigen (PSA) rate at 28 weeks when combined with androgen deprivation in the randomized phase II SWOG S0925 trial for patients with new metastatic hormone-sensitive prostate cancer. We now present mature survival analyses, along with pre-specified secondary and exploratory endpoints.
Methods
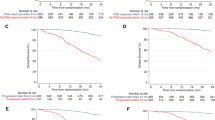
We randomized 210 patients to androgen deprivation with or without cixutumumab, 105 per treatment arm. We used Kaplan–Meier curves to analyze overall survival, radiographic progression-free survival, and castration resistance-free survival by treatment arm, disease volume, and risk group. We explored differences in survival by treatment arm via covariate-adjusted Cox proportional hazards models adjusted for disease volume and risk.
Results
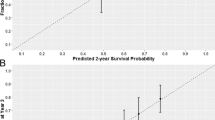
No difference was seen between treatment arms in overall survival (HR 1.01 [0.70–1.45]; p = 0.97), radiographic progression-free survival (HR 1.17 [0.85–1.60]; p = 0.35), or castration resistance-free survival (HR 1.02 [0.75–1.41]; p = 0.88). At baseline, 105/198 (53.0%) patients had high-risk features and 119/210 (56.7%) had high-volume disease; 16.7% of patients had discordant classifications of high or low category for risk and volume. Adjusting for risk or volume yielded no differences in overall survival between arms. Inferior survival was observed in high-risk (HR 1.89 [1.29–2.80]; p = 0.001) and high-volume (HR 2.75 [1.84–4.10]; p < 0.0001) disease. Disease volume was a better fit to survival data than risk group (AIC 878.3 vs. 889.2). Compared to patients achieving undetectable PSA at 28 weeks, inferior survival was observed in patients whose PSA was >0.2 to ≤4.0 ng/mL (HR 3.72 [1.99–6.95]; p < 0.0001) or >4.0 ng/mL (HR 7.13 [4.24–11.9]; p < 0.0001).
Conclusions
In new metastatic hormone-sensitive prostate cancer, addition of cixutumumab to androgen deprivation did not improve survival. Baseline risk and disease volume carried prognostic value for this distinct trial population, although disease volume added more prognostic information. PSA treatment response was a strong intermediate endpoint for survival.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Wu JD, Haugk K, Woodke L, Nelson P, Coleman I, Plymate SR. Interaction of IGF signaling and the androgen receptor in prostate cancer progression. J Cell Biochem. 2006;99:392–401.
Wu JD, Odman A, Higgins LM, Haugk K, Vessella R, Ludwig DL, et al. In vivo effects of the human type I insulin-like growth factor receptor antibody A12 on androgen-dependent and androgen-independent xenograft human prostate tumors. Clin Cancer Res. 2005;11:3065–74.
Higano CS, Alumkal J, Ryan CJ, Yu EY, Beer TM, Chandrawansa K, et al. A phase II study evaluating the efficacy and safety of single agent IMC A12, a monoclonal antibody, against the insulin-like growth factor-1 receptor, as monotherapy in patients with metastatic, asymptomatic castration-resistant prostate cancer. J Clin Oncol. 2009;27:269s. suppl; abstr 5142
Higano CS, Alumkal J, Ryan CJ, Yu EY, Beer TM, Fox FE et al. A phase II study of cixutumumab (IMC-A12), a monoclonal antibody against the insulin-like growth factor 1 receptor (IGF-IR), monotherapy in metastatic castration-resistant prostate cancer: feasibility of every 3-week dosing and updated results. Genitourinary Cancers Symposium, 2010; San Francisco, CA, USA. Abstr 189.
Dean JP, Sprenger CC, Wan J, Haugk K, Ellis WJ, Lin DW, et al. Response of the insulin-like growth factor (IGF) system to IGF-IR inhibition and androgen deprivation in a neoadjuvant prostate cancer trial: effects of obesity and androgen deprivation. J Clin Endocrinol Metab. 2013;98:E820–8.
Chi KN, Gleave ME, Fazli L, Goldenberg SL, So A, Kollsmannsberger C, et al. A phase II pharmacodynamic study of preoperative figitumumab in patients with localized prostate cancer. Clin Cancer Res. 2012;18:3407–13.
Yu EY, Li H, Higano CS, Agarwal N, Pal SK, Alva A, et al. SWOG S0925: a randomized phase II study of androgen deprivation combined with cixutumumab versus androgen deprivation alone in patients with new metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2015;33:1601–8.
Hussain M, Tangen CM, Higano C, Schelhammer PF, Faulkner J, Crawford ED, et al. Absolute prostate-specific antigen value after androgen deprivation is a strong independent predictor of survival in new metastatic prostate cancer: data from Southwest Oncology Group Trial 9346 (INT-0162). J Clin Oncol. 2006;24:3984–90.
Sweeney CJ, Chen YH, Carducci M, Liu G, Jarrard DF, Eisenberger M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N. Engl J Med. 2015;373:737–46.
Kyriakopoulos CE, Chen YH, Carducci MA, Liu G, Jarrard DF, Hahn NM, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer: long-term survival analysis of the randomized phase III E3805 CHAARTED trial. J Clin Oncol. 2018;36:1080–7.
James ND, Sydes MR, Clarke NW, Mason MD, Dearnaley DP, Spears MR, et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet. 2016;387:1163–77.
Gravis G, Boher JM, Chen YH, Liu G, Fizazi K, Carducci MA, et al. Burden of metastatic castrate naive prostate cancer patients, to identify men more likely to benefit from early docetaxel: further analyses of CHAARTED and GETUG-AFU15 studies. Eur Urol. 2018;73:847–55.
Harshman LC, Chen YH, Liu G, Carducci MA, Jarrard D, Dreicer R, et al. Seven-month prostate-specific antigen is prognostic in metastatic hormone-sensitive prostate cancer treated with androgen deprivation with or without docetaxel. J Clin Oncol. 2018;36:376–82.
Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med. 2017;377:352–60.
Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, et al. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2019;20:686–700.
James ND, de Bono JS, Spears MR, Clarke NW, Mason MD, Dearnaley DP, et al. Abiraterone for prostate cancer not previously treated with hormone therapy. N. Engl J Med. 2017;377:338–51.
Hoyle AP, Ali SA, James ND, Parker CC, Cook AD, Attard G. et al. Effects of abiraterone acetate plus prednisone/prednisolone in high and low risk metastatic hormone sensitive prostate cancer. In: ESMO 2018 Congress, Munich, Germany, 21 October, 2018.
Pocock SJ, Simon R. Sequential treatment assignment with balancing for prognostic factors in the controlled clinical trial. Biometrics. 1975;31:103–15.
Davis ID, Martin AJ, Stockler MR, Begbie S, Chi KN, Chowdhury S, et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med. 2019;381:121–31.
Armstrong AJ, Szmulewitz RZ, Petrylak DP, Villers A, Azad A, Alcaraz A et al. Phase 3 study of androgen deprivation therapy (ADT) with enzalutamide (ENZA) or placebo (PBO) in metastatic hormone-sensitive prostate cancer (mHSPC): the ARCHES trial (abstract). J Clin Oncol. 2019;37(7_suppl):687.
Chi KN, Agarwal N, Bjartell A, Chung BH, Pereira de Santana Gomes AJ, Given R, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med. 2019;381:13–24.
Flaig TW, Plets M, Hussain MHA, Agarwal N, Mitsiades N, Deshpande HA, et al. Abiraterone acetate for metastatic prostate cancer in patients with suboptimal biochemical response to hormone induction. JAMA Oncol. 2017;3:e170231.
Crawford ED, Eisenberger MA, McLeod DG, Spaulding JT, Benson R, Dorr FA, et al. A controlled trial of leuprolide with and without flutamide in prostatic carcinoma. N Engl J Med. 1989;321:419–24.
Scher HI, Halabi S, Tannock I, Morris M, Sternberg CN, Carducci MA, et al. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group. J Clin Oncol. 2008;26:1148–59.
Acknowledgements
Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health, the Clinical Research Division of the Fred Hutchinson Cancer Research Center, and in part by ImClone Systems (subsidiary of Eli Lilly and Company). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Funding
Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under award numbers CA180888, CA180819, CA180818, CA180828, CA233328, CA46368, CA180801, CA180835, CA35421, CA180834, CA142559, CA35281, CA35090, CA37981, CA45807, CA46282, CA180846, CA180830, CA35431, CA58416, CA63848, CA63844, CA12644, CA11083, CA35178, CA67575, and CA45808, by the Clinical Research Division of the Fred Hutchinson Cancer Research Center, and in part by ImClone Systems (subsidiary of Eli Lilly and Company).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
EY has received research support from Dendreon, Merck, and Seattle Genetics and consulted for Bayer, Clovis, Dendreon, Janssen, and Merck. NA has consulted for Astellas, AstraZeneca, BMS, Bayer, Clovis, Eisai, Exelixis, EMD Serono, Eli Lilly, Foundation Medicine, Genentech, Janssen, Merck, Novartis, Nektar, Pfizer, and Pharmacyclics. HC has received research support from Clovis, Janssen, Medivation, and Sanofi. MH has received honoraria from Aptitude Health, Astellas, Epics, Genentech, PER, Research to Practice, and Sanofi/Genzyme, consulted for AstraZeneca, Bayer, and Pfizer, received research support from AstraZeneca, Bayer, Genentech, and Pfizer, and received travel and accommodation support from Astellas, AstraZeneca, Bayer, Genentech, and Pfizer. DQ has consulted for Astellas, Bayer, Janssen, Pfizer, Sanofi, and AstraZeneca. The other authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Wong, R.L., Duong, M.T., Tangen, C.M. et al. Survival outcomes and risk group validation from SWOG S0925: a randomized phase II study of cixutumumab in new metastatic hormone-sensitive prostate cancer. Prostate Cancer Prostatic Dis 23, 486–493 (2020). https://doi.org/10.1038/s41391-020-0210-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41391-020-0210-x
