
Abstract
Introduction
Focal therapy (FT) ablates areas of prostate cancer rather than treating the whole gland. We compared oncological outcomes of FT to radical prostatectomy (RP).
Methods
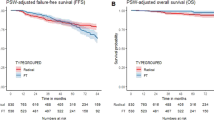
Using prospective multicentre databases of 761 FT and 572 RP cases (November/2005-September/2018), patients with PSA < 20 ng/ml, Gleason </= 4 + 3 and stage </= T2c were 1–1 propensity score-matched for treatment year, age, PSA, Gleason, T-stage, cancer core length and use of neoadjuvant hormones. FT included 1–2 sessions. Primary outcome was failure-free survival (FFS) defined by need for salvage local or systemic therapy or metastases. Differences in FFS were determined using Kaplan–Meier analysis with log-rank test.
Results
335 radical prostatectomy and 501 focal therapy patients were eligible for matching. For focal therapy, 420 had HIFU and 81 cryotherapy. Cryotherapy was used predominantly for anterior cancer. After matching, 246 RP and 246 FT cases were identified. For radical prostatectomy, mean (SD) age was 63.4 (5.6) years, median (IQR) PSA 7.9 g/ml (6–10) and median (IQR) follow-up 64 (30–89) months. For focal therapy, these were 63.3 (6.9) years, 7.9 ng/ml (5.5–10.6) and 49 [34–67] months, respectively. At 3, 5 and 8 years, FFS (95%CI) was 86% (81–91%), 82% (77–88%) and 79% (73–86%) for radical prostatectomy compared to 91% (87–95%), 86% (81–92%) and 83% (76–90%) following focal therapy (p = 0.12).
Conclusions
In patients with non-metastatic low- intermediate prostate cancer, oncological outcomes over 8 years were similar between focal therapy and radical prostatectomy.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others


References
Hamdy FC, Donovan JL, Lane JA, Mason M, Metcalfe C, Holding P, et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N. Engl J Med. 2016;375:1415–24.
Bill-Axelson A, Holmberg L, Garmo H, Rider JR, Taari K, Busch C, et al. Radical prostatectomy or watchful waiting in early prostate cancer. N Engl J Med. 2014;370:932–42.
Wilt TJ, Jones KM, Barry MJ, Andriole GL, Culkin D, Wheeler T, et al. Follow-up of prostatectomy versus observation for early prostate cancer. N Engl J Med. 2017;377:132–42.
Veronesi UCN, Mariani L, Greco M, Saccozzi R, Luini A, Aguilar M, et al. Twenty- year follow-up of a randomized study comparing breast- conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 2002;347:1227–32.
Cao C, Chandrakumar D, Gupta S, Yan TD, Tian DH. Could less be more?-A systematic review and meta-analysis of sublobar resections versus lobectomy for non-small cell lung cancer according to patient selection. Lung Cancer. 2015;89:121–32.
Pierorazio PM, Johnson MH, Patel HD, Sozio SM, Sharma R, Iyoha E, et al. Management of renal masses and localized renal cancer: systematic review and meta-analysis. J Urol. 2016;196:989–99.
Shah TT, Peters M, Eldred-Evans D, Miah S, Yap T, Faure-Walker NA, et al. Early-medium-term outcomes of primary focal cryotherapy to treat nonmetastatic clinically significant prostate cancer from a prospective multicentre registry. Eur Urol. 2019;76:98–105.
Guillaumier S, Peters M, Arya M, Afzal N, Charman S, Dudderidge T, et al. A multicentre study of 5-year outcomes following focal therapy in treating clinically significant nonmetastatic prostate cancer. Eur Urol. 2018;74:422–9.
Kuru TH, van Essen J, Pfister D, Porres D. Role of focal therapy with high-intensity focused ultrasound in the management of clinically localized prostate cancer. Oncol Res Treat. 2015;38:634–8.
Ahdoot M, Lebastchi AH, Turkbey B, Wood B, Pinto PA. Contemporary treatments in prostate cancer focal therapy. Curr Opin Oncol. 2019;31:200–6.
Valerio M, Cerantola Y, Eggener SE, Lepor H, Polascik TJ, Villers A, et al. New and established technology in focal ablation of the prostate: a systematic review. Eur Urol. 2017;71:17–34.
Albisinni S, Aoun F, Bellucci S, Biaou I, Limani K, Hawaux E, et al. Comparing high-intensity focal ultrasound hemiablation to robotic radical prostatectomy in the management of unilateral prostate cancer: a matched-pair analysis. J Endourol. 2017;31:14–9.
Hamdy FC, Steffi le Conte DE, Davies LC, Burns RM, Thomson C, Gray R, et al. Partial ablation versus radical prostatectomy in intermediate-risk prostate cancer: the PART feasibility RCT. Health Technol Assess. 2018;22:1–96.
Ahmed HU, Berge V, Bottomley D, Cross W, Heer R, Kaplan R, et al. Can we deliver randomized trials of focal therapy in prostate cancer? Nat Rev Clin Oncol. 2014;11:482–91.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370:1453–7.
Parker C, Clarke NW, Cook A, Kynaston HG, Meidahl Petersen P, Cross W, et al. Timing of radiotherapy (RT) after radical prostatectomy (RP): first results from the RADICALS RT randomised controlled trial (RCT) [NCT00541047]. Ann Oncol. 2019;30:v883–v4. (abstract LBA49_PR)
Austin PC. The use of propensity score methods with survival or time-to-event outcomes: reporting measures of effect similar to those used in randomized experiments. Stat Med. 2014;33:1242–58.
Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat. 2011;10:150–61.
Garcia-Barreras S, Sanchez-Salas R, Sivaraman A, Barret E, Secin F, Nunes-Silva I. Comparative analysis of partial gland ablation and radical prostatectomy to treat low and intermediate risk prostate cancer: oncologic and functional outcomes. J Urol. 2018;199:140–6.
Scheltema MJ, Chang JI, Bohm M, van den Bos W, Blazevski A, Gielchinsky I, et al. Pair-matched patient-reported quality of life and early oncological control following focal irreversible electroporation versus robot-assisted radical prostatectomy. World J Urol. 2018;36:1383–9.
Tay KJ, Polascik TJ, Elshafei A, Tsivian E, Jones JS. Propensity score-matched comparison of partial to whole-gland cryotherapy for intermediate-risk prostate cancer: an analysis of the cryo on-line data registry data. J Endourol. 2017;31:564–71.
Huber, PM, Afzal, N, Arya, M, Boxler, S, Dudderidge, T, Emberton, M, et al. Prostate specific antigen criteria to diagnose failure of cancer control following focal therapy of nonmetastatic prostate cancer using high intensity focused ultrasound. J Urol. 2020;203:734–42.
Azzouzi A-R, Vincendeau S, Barret E, Cicco A, Kleinclauss F, van der Poel HG, et al. Padeliporfin vascular-targeted photodynamic therapy versus active surveillance in men with low-risk prostate cancer (CLIN1001 PCM301): an open-label, phase 3, randomised controlled trial. Lancet Oncol. 2017;18:181–91.
Taneja SS. Re: padeliporfin vascular-targeted photodynamic therapy versus active surveillance in men with low-risk prostate cancer (CLIN1001 PCM301): an open-label, phase 3, randomised controlled trial. J Urol. 2017;198:255–7.
Sivaraman A, Barret E. Focal therapy for prostate cancer: an “A la Carte” approach. Eur Urol. 2016;69:973–5.
Reddy D, Shah TT, Dudderidge T, McCracken S, Arya M, Dobbs C, et al. Comparative Healthcare Research Outcomes of Novel Surgery in prostate cancer (IP4-CHRONOS): a prospective, multi-centre therapeutic phase II parallel Randomised Control Trial. Contemp Clin Trials. 2020;93:105999.
Ahmed HU, Hu Y, Carter T, Arumainayagam N, Lecornet E, Freeman A, et al. Characterizing clinically significant prostate cancer using template prostate mapping biopsy. J Urol. 2011;186:458–64.
Coughlin GD, Yaxley JW, Chambers SK, Occhipinti S, Samaratunga H, Zajdlewicz L, et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: 24-month outcomes from a randomised controlled study. Lancet Oncol. 2018;19:1051–60.
Funding
Sonacare and support the HIFU UK national registry (called HEAT) through an unrestricted grant. Galil/BTG Ltd previously supported the cryotherapy UK registry (called ICE, previously known as EuCAP) through unrestricted grants. None of the funding sources had any role or input into the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
Author information
Authors and Affiliations
Contributions
TS and DR were responsible for data collection, analysis of the data. TS, DR and MP were responsible for production of the first draught and completed the data analysis. All authors were involved in data collection, manuscript preparation/draughting and approval of the final draught. HUA and MW had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. HUA and MW are guarantors of the study.
Corresponding author
Ethics declarations
Conflict of interest
HUA’s research is supported by core funding from the United Kingdom’s National Institute of Health Research (NIHR) Imperial Biomedical Research Centre. HUA currently receives funding from the Wellcome Trust, Medical Research Council (UK), Cancer Research UK, Prostate Cancer UK, The Urology Foundation, BMA Foundation, Imperial Health Charity, NIHR Imperial BRC, Sonacare Inc., Trod Medical and Sophiris Biocorp for trials in prostate cancer. HUA was a paid medical consultant for Sophiris Biocorp in the previous 3 years. ME’s research is supported by core funding from the United Kingdom’s National Institute of Health Research (NIHR) UCLH/UCL Biomedical Research Centre. He was awarded NIHR Senior Investigator in 2015. ME receives funding from NIHR-i4i, MRC (UK), Cancer Research UK, Sonacare Inc., Trod Medical, Cancer Vaccine Institute and Sophiris Biocorp for trials in prostate cancer. ME is a medical consultant to Sonacare Inc., Sophiris Biocorp, Steba Biotech, Exact Imaging and Profound Medical. CMM receives funding from the National Institute for Health Research, The European Association of Urology Research Foundation, MRC, Cancer Research UK, Prostate Cancer UK, Movember and the Cancer Vaccine Institute, for clinical prostate cancer research. She has received advisory board fees for Genomic Health. TTS receives funding from Prostate Cancer UK and the St Peters Trust for clinical research and has received funding for conference attendance from Astellis, Ferring and Galil Medical. HUA, ME, RH, CMM and MA are all proctors for HIFU and are paid for training other surgeons in this procedure. HUA and MA are proctors for cryotherapy and are paid for training other surgeons in this procedure. ME is a proctor for Irreversible Electroporation (Nanoknife) and is paid for training other surgeons in this procedure. HUA and RH are paid proctors for Rezum for the treatment of benign prostate hyperplasia. MW receives a travel grant and a loan of device from Zicom Biobot. DR is funded by a research grant from Prostate Cancer UK and receives travel grants from Imperial Health Charity. EE receives funding from the Urology Foundation, the BMA Foundation for Medical Research, Imperial Health Charity and the Royal College of Surgeons of England. None of the other authors have anything to declare.
Ethics approval and consent to participate
Prospective data collection was approved locally by Imperial College Healthcare NHS Trust Research and Development department for service and quality assurance, therefore the requirement of informed consent of patients was waived. The study was performed in accordance with the declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Shah, T.T., Reddy, D., Peters, M. et al. Focal therapy compared to radical prostatectomy for non-metastatic prostate cancer: a propensity score-matched study. Prostate Cancer Prostatic Dis 24, 567–574 (2021). https://doi.org/10.1038/s41391-020-00315-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41391-020-00315-y
This article is cited by
-
Transperineal Targeted Microwave Ablation (TMA) of localized prostate cancer guided by MRI-Ultrasound fusion and organ-based tracking: a pilot study
Prostate Cancer and Prostatic Diseases (2023)
-
The state of focal therapy in the treatment of prostate cancer: the university of California collaborative (UC-Squared) consensus statement
Prostate Cancer and Prostatic Diseases (2023)
-
Focal prostate cancer therapy in the era of multiparametric MRI: a review of options and outcomes
Prostate Cancer and Prostatic Diseases (2023)
-
Focal therapy in intermediate- and high-risk prostate cancer
memo - Magazine of European Medical Oncology (2023)
-
The use of advanced imaging in guiding the further investigation and treatment of primary prostate cancer
Cancer Imaging (2022)
