
Abstract
Background
Studies have shown that infant temperament varies with maternal psychosocial factors, in utero illness, and environmental stressors. We predicted that the pandemic would shape infant temperament through maternal SARS-CoV-2 infection during pregnancy and/or maternal postnatal stress. To test this, we examined associations among infant temperament, maternal prenatal SARS-CoV-2 infection, maternal postnatal stress, and postnatal COVID-related life disruptions.
Methods
We tested 63 mother–infant dyads with prenatal maternal SARS-CoV-2 infections and a comparable group of 110 dyads without infections. To assess postnatal maternal stress, mothers completed the Perceived Stress Scale 4 months postpartum and an evaluation of COVID-related stress and life disruptions 6 months postpartum. Mothers reported on infant temperament when infants were 6-months-old using the Infant Behavior Questionnaire-Revised (IBQ-R) Very Short Form.
Results
Maternal SARS-CoV-2 infection during pregnancy was not associated with infant temperament or maternal postnatal stress. Mothers with higher self-reported postnatal stress rated their infants lower on the Positive Affectivity/Surgency and Orienting/Regulation IBQ-R subscales. Mothers who reported greater COVID-related life disruptions rated their infants higher on the Negative Emotionality IBQ-R subscale.
Conclusions
Despite no effect of prenatal maternal SARS-CoV-2 infection, stress and life disruptions incurred by the COVID-19 pandemic were associated with infant temperament at 6-months.
Impact
-
SARS-CoV-2 infection during pregnancy is not associated with postnatal ratings of COVID-related life disruptions, maternal stress, or infant temperament.
-
Postnatal ratings of maternal stress during the COVID-19 pandemic are associated with normative variation in maternal report of infant temperament at 6 months of age.
-
Higher postnatal ratings of maternal stress are associated with lower scores on infant Positive Affectivity/Surgency and Orienting/Regulation at 6 months of age.
-
Higher postnatal ratings of COVID-related life disruptions are associated with higher scores on infant Negative Emotionality at 6 months of age.
Similar content being viewed by others

Introduction
We focus this investigation on the impact of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic on pregnant women and their infants. New mothers were at risk for SARS-CoV-2 infection during pregnancy and a series of unexpected psychosocial stressors in the perinatal period.1,2,3,4 We report data from the COVID-19 Mother Baby Outcomes (COMBO) Initiative, (www.ps.columbia.edu/COMBO), which is a prospective study established at Columbia University Irving Medical Center (CUIMC) in New York City (NYC) in Spring 2020 to study the effects of in utero exposure to maternal SARS-CoV-2 infection on the health and wellbeing of both mothers and infants from the first U.S. pandemic epicenter. Specifically, here we examined the impact of SARS-CoV-2 infection during pregnancy, as well as maternal postnatal perceived stress and coronavirus disease (COVID)-related life disruptions during the pandemic, on mother-reported infant temperament at 6 months in a subset of COMBO participants.
Infant temperament refers to infants’ emerging ability to regulate their own behavior and emotions.5 A standard parent-report instrument for infant temperament is the Infant Behavior Questionnaire-Revised (IBQ-R).6 This instrument offers a reliable and valid index of three temperament dimensions: Negative Emotionality, positive affect referred to as Positive Affectivity/Surgency, and Orienting/Regulation capacity.7 The Positive Affectivity/Surgency dimension is thought to index infant experience of pleasure, vocal reactivity, and approach or activity level (note that the infant IBQ-R does not index impulsivity).6 The Negative Emotionality dimension captures early infant fear, fussiness, and distress to limitations. The Orienting/Regulation capacity dimension provides insight into infants’ capacity to orient attention to elements in their environment, as well as soothability, and has been shown to predict later effortful control over thoughts and actions.8,9,10
Here we examined the association between infant temperament at 6 months and maternal SARS-CoV-2 infection during pregnancy. Although data have shown that SARS-CoV-2 rarely passes from mothers to infants,11,12,13 maternal viruses have been shown to impact infant development through mechanisms of general maternal immune activation (MIA) independent of viral transmission.14 Specifically, maternal viral infection during pregnancy is associated with increased levels of interleukin 6, a protein generated by immune response that may increase fetal inflammation and thus disrupt development.14 For example, mothers who experienced illness or infection during pregnancy rated their 6-month-olds higher on fussy/difficult, dullness, and needs attention temperamental indices.15 A cohort of Finnish dyads demonstrated an association between maternal report of fever and infant distress to novelty.16 A mechanistic possibility for these associations comes from animal research that suggests that chemical abnormalities related to MIA may impact temperament indirectly through infant physical development, as maternal illness is associated with fetal growth restriction, which correlates with temperament development.15,17 Other work links human coronaviruses to birth complications—in utero exposure to SARS-CoV-2, Middle East Respiratory Syndrome, and Severe Acute Respiratory Syndrome associated with greater risk of preterm birth, preeclampsia, cesarean, and perinatal death.18,19
We also examined, in the same dyads, maternal postnatal perceived stress and COVID-related life disruptions at 4- and 6-months postpartum, respectively. The stress incurred by the sudden escalation of SARS-CoV-2, from virus to pandemic in a matter of weeks, cannot be understated. Lives changed overnight and most Americans experienced an influx of unexpected hardships including illness, loss of jobs and income, death of family and friends, and significant disruptions to daily life. The impact of these stressors on health and disease will be an area of significant study for years to come. Longitudinal studies have previously demonstrated elevated risks for poorer mental and physical health as a consequence of stress and adversity.20 Using the IBQ-R, studies have found associations between pre- and postnatal stress and infant temperament.6,21,22 Prenatal exposure to traumatic events such as natural disasters and intimate partner violence associate with higher maternal ratings of infant Negative Affectivity and lower ratings of Effortful Control/Regulation and Positive Affectivity.23 Perhaps most relevant, previous work in a cohort of Italian infants showed that maternal retrospective report of prenatal stress during the COVID-19 pandemic was associated with infant (but not maternal) postnatal epigenetic markers of stress, which in turn were negatively associated with 3-month-old infants’ Positive Affectivity/Surgency.24 Other work in the same Italian cohort linked infant regulatory capacity at 3 months with maternal prenatal anxiety.25 Postnatal stress has also been shown to shape infant temperament. A study of mothers who gave birth in the wake of Hurricane Sandy revealed that storm-related stressors (e.g. loss of electricity, financial hardship), evaluated at 6-months post-partum, correlated with higher scores on negative affect and lower scores on emotional regulation.22 However, the effects of postnatal stress specifically related to the COVID-19 pandemic remain unknown. Our analysis fills this gap, contributing to a larger framework of the differential impacts of pre- and postnatal pandemic stress across cohorts.
Our analysis includes dyads from the COMBO Initiative in NYC, which enrolls mother–infant dyads wherein the mother contracted SARS-CoV-2 during pregnancy (exposed group) and an age-matched group of infants whose mothers also experienced the COVID-19 pandemic, but were not themselves infected (unexposed group). Our predictions were as follows: if prenatal SARS-CoV-2 infection impacts fetal development, ostensibly through MIA, we would expect infants in the exposed group to have higher scores on the Negative Emotionality temperament dimension and lower scores on the Positive Affectivity/Surgency and Orienting/Regulation capacity temperament dimensions than infants in the unexposed group. Alternatively, the mechanism of impact may be through maternal stress levels, here assessed postpartum. Drawing from developmental literature on maternal stress, we would expect infant temperament scores to vary in association with mothers’ pandemic stress ratings independent of maternal SARS-CoV-2 infection status. In particular, mothers with higher postnatal stress will rate their infants as having lower Positive Affectivity/Surgency and Orienting/Regulation capacity and higher Negative Emotionality. Finally, if SARS-CoV-2 infection results in an additional stressor for mothers, we would expect higher perceived stress ratings in exposed relative to unexposed mothers, with this stress explaining any association between infection status and infant temperament.
Methods
Participants
We report data from N = 173 COMBO-enrolled mother–infant dyads who gave birth at the CUIMC-affiliated NewYork–Presbyterian (NYP) Morgan Stanley Children’s Hospital (MSCH) or NYP Allen Pavilion Hospital between March and December of 2020. COMBO enrollment occurs on the basis of electronic health record (EHR) screening of all pregnant and delivering mothers at the two participating hospitals (combined >6000 births/year). All mothers with a documented history of SARS-CoV-2 during pregnancy or at delivery and who delivered during the study period were approached for participation in COMBO (exposed group). Each exposed dyad enrolled into COMBO was then matched to 1–3 dyads with comparable infant sex, gestational age at birth, mode of delivery, and date of birth within a 2-week window of the exposed dyad but where the mother tested negative for SARS-CoV-2 at the time of delivery and had no documented or suspected history of COVID-19 at any point during pregnancy (unexposed group). Dyads were approached for initial enrollment during pregnancy or first few months after birth. For the reported study period, 1706 dyads were approached for participation, and 596 were enrolled into COMBO. Here, only COMBO-enrolled dyads with complete data on both the IBQ-R and the maternal stress indices (collected at 4 and 6 months postpartum) were included (Supplemental Fig. 1), which comprised 63 exposed and 110 unexposed dyads (Table 1). To check for selection bias, included dyads were compared to the 423 dyads enrolled in COMBO during the same study period but who did not complete one or both of the 4- and 6-month surveys. No significant differences were identified (Supplemental Table 1). The CUIMC Institutional Review Board reviewed and approved all study procedures, and all mothers provided consent prior to participation.
Determination of maternal SARS-CoV-2 infection status
Maternal infection status was determined through electronic health records (EHR). The labor and delivery (L&D) units of the NYP hospital system implemented universal SARS-CoV-2 testing of all delivering patients by nasopharyngeal PCR beginning on 3/22/2020 and by serological testing for antibodies beginning on 7/20/2020. Additional symptom-based testing occurred throughout pregnancy and test results obtained from external testing sites were recorded in the EHR when possible.
Procedures
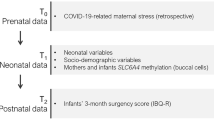
Surveys were administered in English or Spanish via secure REDCap questionnaires. Mothers completed the Perceived Stress Scale (PSS) when infants were 4 months old and the COVID-19 and Perinatal Experiences (COPE) Study survey (www.covgen.org) and IBQ-R when infants were 6 months old.
Survey instruments
The PSS26 is a widely-used 14-question survey designed to capture the prevalence of stress and regulation strategies in participants’ lives during the month prior to evaluation. Participants reported how often they experienced feelings related to generalized stress (e.g., irritability, nerves, lack of control) on a 5-point Likert scale (0—never, 1—almost never, 2—sometimes, 3—fairly often, and 4—very often). The scale has historically strong internal and test-retest reliability.26 The Cronbach’s alpha in our study sample was 0.82, which is in the similar range reported in prior studies.27 Scores range from 0 to 56, with a higher score indicating more perceived stress.
The COPE survey was developed in March 2020 by a multidisciplinary group of researchers to evaluate the influence of COVID-19 on mothers’ lives (www.covgen.org). COPE asks several questions about maternal stress specifically related to the COVID-19 pandemic. The questions included in our analyses here specifically target maternal stress levels:
-
A.
COVID-19 Change in Stress: How has the COVID-19 outbreak changed your stress levels or mental health? 1, Worsened them significantly | 2, Worsened them moderately | 3, No change | 4, Improved them moderately | 5, Improved them significantly.
-
B.
COVID-19 Valence & Impact: Please indicate the extent to which you view the COVID-19 outbreak as having either a positive or negative impact on your life. 1, Extremely Negative | 2, Moderate Negative | 3, Somewhat Negative | 4, No Impact | 5, Slightly Positive | 6, Moderately Positive | 7, Extremely Positive.
-
C.
COVID-19 Stress Level: Overall level of stress related to the COVID-19 outbreak. 1 None–7 Extreme.
The IBQ-R Very Short Form is a condensed version of the IBQ-R6 evaluating 3 domains of infant temperament: Positive Affectivity/Surgency, Negative Emotionality, and Orienting/Regulation. Mothers rated the prevalence of 37 behaviors relevant to each domain on a 7-point scale (1—never, 2—very rarely, 3—less than half the time, 4—about half the time, 5—more than half the time, 6—almost always, 7—always). Sample questions from the IBQ-R are shown in Supplemental Table 2. Scores on each domain range from 1 to 7. IBQ-R Very Short Form scores have been shown to correlate with scores from the long form questionnaire and have strong internal and test-retest reliability.28 Cronbach’s alpha in our study sample was 0.87, consistent with previous reports.29 The temperament dimensions derived from the short versions of the IBQ-R have been shown to be similar to those measured using fine-grained temperament assessments in older children and adults.8,30
Study population characteristics
Table 1 shows study population characteristic for SARS-CoV-2-exposed and unexposed mothers and their infants included in this analysis. There were group-level differences in both maternal income: F(1, 171) = 6.20, p = 0.01, and maternal education, F(1, 171) = 10.95, p = 0.001. Mothers in the unexposed group had higher socioeconomic status (income, education) than mothers in the exposed group. There were no other significant measured differences between groups. Maternal education and income are highly-correlated, r(173) = 0.64, p < 0.001. To avoid multi-collinearity, only maternal education was adjusted for in subsequent analyses.
Analysis plan
We first examined characteristics of mothers in the exposed and unexposed groups for differences that might bear on subsequent analyses. To assess whether SARS-CoV-2 infection was an added stressor, i.e., whether exposed mothers had higher self-reported stress scores than unexposed mothers, we used generalized linear regression models to examine the association between maternal SARS-CoV-2 infection status during pregnancy (independent variable) and maternal postnatal stress measures (dependent variables), specifically: COVID-19 Valence & Impact, COVID-19 Stress Level, COVID-19 Change in Stress Level, and Perceived Stress Scale scores. All models were adjusted for infant sex, infant age at assessment of temperament, maternal education, and maternal age (see Table 2 for full correlations).
Next, we examined the association between infant temperament and (a) SARS-CoV-2 infection, and (b) maternal self-reported stress in the same models. Models were used for each of the three unique temperament-dependent variables: Positive Affectivity/Surgency, Negative Emotionality, Orienting/Regulation. Each model included the four stress measures (COVID-19 Valence & Impact, Stress Level, Change in Stress Level, and Perceived Stress Scale scores) and maternal SARS-CoV-2 infection status as independent variables. All models were adjusted for infant sex, infant age at assessment of temperament, maternal education, and maternal age.
Results
SARS-CoV-2 infection during pregnancy and maternal stress
Table 3 shows means and standard deviations for relevant variables. Maternal SARS-CoV-2 infection status was not significantly associated with COVID-19 Valence & Impact scores [F(1,166) = 0.01, p = 0.92, ηp2 < 0.001], COVID-19 Change in Stress scores [F(1,166) = 0.43, p = 0.51, ηp2 = 0.003], COVID-19 Stress Level [F(1,166) = 0.01, p = .94, ηp2 < 0.001] or PSS scores [F(1,166) = 2.36, p = 0.13, ηp2 = 0.014]. These data indicate that maternal postnatal experience of pandemic stress was similar regardless of SARS-CoV-2 infection status during pregnancy.
SARS-CoV-2 infection, COVID-19 postnatal pandemic stress, and infant temperament
Table 4 reports the associations between maternal SARS-CoV-2 infection and postnatal pandemic stress and infant temperament scores. Maternal SARS-CoV-2 infection was not associated with any temperament dimension. In contrast, the COVID-19 Valence & Impact score significantly predicted infant Negative Emotionality [F(1,162) = 5.67, p < 0.05, ηp2 = 0.03]. With each unit increase in COVID-19 Valence & Impact scores (scale of 1–7, 1 is Extremely Positive and 7 is Extremely Negative) there was 0.14 increase (95% CI: 0.02, 0.25) in mother-reported infant Negative Emotionality. Figure 1a shows predicted mean values of the Negative Emotionality dependent variable as a function of maternal ratings of COVID-19 Valence & Impact. After adjusting for influences of mothers’ age and education, infants’ age and sex, and SARS-CoV-2 infection, higher values of reported maternal COVID-19 Valence & Impact were associated with higher maternal report of infants’ Negative Emotionality.

The figure illustrates the relationship between a COVID-19 Valence & Impact score and Negative Emotionality at 6-months. b, c Relationship between maternal Perceived Stress Score and infant 6-month Positive Affectivity/Surgency (b) and Orienting/Regulation scores (c). Y-axis values are predicted (not raw) scores for the dependent variable generated from GLMs and adjusted for maternal education, maternal age, infant age, and infant sex.
Table 4 also shows that maternal perceived stress (PSS) scores were significantly associated with Positive Affectivity/Surgency [F(1,162) = 8.60, p < 0.01, ηp2 = 0.05] and Orienting/Regulation [F(1,162) = 5.59, p < .05, ηp2 = 0.03]. With each unit increase in maternal perceived stress reported when infants were 4-months-old, there was a −0.03 (95% CI: −0.04, −0.01) decrease in Positive Affectivity/Surgency scores. Figure 1b shows predicted mean values of the Positive Affectivity/Surgency dependent variable on the y-axis and maternal ratings of perceived stress on the x-axis. After adjusting for influences of mother’s age and education, infants’ age and sex, and SARS-CoV-2 infection, higher values of reported maternal postnatal stress were associated with lower values for Positive Affectivity/Surgency (see Fig. 1b).
Maternal PSS scores were also significantly associated with infants’ Orienting/Regulation scores (Table 4). With each unit increase in maternal perceived stress, there was a −0.02 (95% CI: −0.03, 0.00) reduction in Orienting/Regulation scores (Table 4). Figure 1c illustrates the results showing that, after adjusting for influences of mother’s age and education, and infants’ age and sex, higher maternal perceived stress during the COVID-19 pandemic is associated with lower values for Orienting/Regulation. Similarly, the COVID-19 Stress Level score (Overall level of stress related to the COVID-19 outbreak. 1 None–7 Extreme) was also associated with a reduction in infant Orienting/Regulation scores [F(1,162) = 4.30, p < 0.05, ηp2 = 0.03]. With each unit increase in maternal COVID-19 Stress Level, there was a −0.08 (95% CI: −0.15, 0.00) decrease in Orienting/Regulation scores.
Discussion
Our data did not show any associations between maternal SARS-Cov2 infection during pregnancy and infant temperament at 6 months (Table 4). We also did not find any association between maternal prenatal infection and maternal postnatal stress. However, maternal postnatal experience of stress imposed by the pandemic was associated with variability in maternal report of infant temperament. Specifically, maternal ratings of the impact and valence of the COVID-19 pandemic on their lives (higher scores indicating more extreme negative impact) were associated with higher Negative Emotionality temperament scores in infants (Fig. 1a). Moreover, higher maternal ratings of stress, as measured by the PSS at 4 months postpartum, were associated with lower values for Positive Affectivity/Surgency and Orienting/Regulation capacity in 6-month-old infants (Fig. 1b, c). Finally, maternal report of COVID-19 pandemic stress level at 6 months postpartum was also associated with lower scores on infants’ Orienting/Regulation capacity at 6 months.
While we had predicted that maternal postnatal stress would shape infant temperament, we did not predict the variability seen in the COVID-19 Stress/PSS and COVID-19 Valence & Impact scores on specific temperament dimensions. We are cautious not to over-interpret these differences. For example, it is possible that mothers are able to dissociate feelings and emotions of stress around the pandemic (PSS, COVID-19 Stress Level) from finite tangible negative stressful impacts on their lives as a consequence of the pandemic (COVID-19 Valence & Impact). The Life Events Checklist,31 for example, routinely assessed both the stressor and its impact on the respondent in recognition of the possibility that the same event might impact perceived stress differently in two people separately based on their life experiences. A mother may experience high perceived stress because of the fear associated with a global pandemic, even if the pandemic does not directly increase adversity related to poverty or illness in her specific circumstances. A different mother might experience a change or increase in those adverse experiences but not report this as increased stress because she may have experienced and adapted to other similarly challenging circumstances in the past. Alternatively, or in addition, the results may be due to the sensitivity of the unique questions to detect variability in temperament scores.31 These are issues for future study.
We also showed that maternal report of perceived postnatal stress experienced during the COVID-19 pandemic is associated with infant temperament measures of Negative Emotionality and Positive Affectivity/Surgency. The stressful impact of the global COVID-19 pandemic on new mothers has been documented. Mothers who gave birth during 2020 were tasked with navigating that transition amidst the uncertainty and fear of a global health crisis.1,3 Even without maternal infection, COVID-19 related disruptions in schooling routines for other children, financial security, and social support placed a disproportionate burden on caregivers.4 A survey of new parents conducted between May and June 2020 revealed a unanimous increase in stress, uncertainty, and loneliness related to the pandemic that exacerbated existing mental health issues.1 Respondents were particularly affected by isolation, as they lacked the social support and caregiving aid typically available to new parents.1 In another sample of parents raising newborns during the pandemic, COVID-19 stressors were associated with higher parental stress and apprehension about raising an infant under crisis.3
The direct mechanisms by which postnatal COVID-19 stress and disruption on the lives of mothers impacts their infants’ temperament are not examined in this study. Early infant neurodevelopment is largely dependent on quality of caregiver interactions and well-being.32,33 We can speculate that disruptions imposed by the pandemic on an already challenging time in mothers’ lives may play a role in shaping mother–infant dyadic interactions, which in turn may shape infant temperament.32,33,34 In addition, it is possible that maternal stress is transferred to infants through cortisol in breastmilk.35 However, our stress measures were self-reported and may or may not have been associated with comparable changes in cortisol levels.
Our findings contribute to a broader body of work linking pre- and postnatal maternal stress to infant development in the context of a global crisis. We showed that maternal postnatal stress associated with lower infant positive affectivity and regulatory capacity. Similarly, recent analyses of maternal prenatal stress due to the COVID-19 pandemic in a cohort of Italian mother–infant dyads showed that prenatal stress associated directly with lower infant regulatory capacity25 and indirectly with lower infant positive affectivity.24 Together with these two papers, our work raises important questions about unique contributions of pre- and postnatal stress, and their likely overlap and continuity in the perinatal period, on how maternal stress bears on infant temperament. Establishing this association between maternal stress across the perinatal period and infant temperament in multiple cohorts is the first step for guiding practice in future instances of population-level stressors.
Infant temperament is a strong predictor of later neurodevelopmental outcomes. For example, behavioral inhibition is an extreme form of the negative temperament shown to have high predictive value, if not act as a prodrome, for later life social anxiety.36,37,38 Longitudinal assessments of child temperament between 4 and 13 years of age link maternal ratings of child conduct problems to infant fussiness, activity level, predictability, and positive affect.39 Having established these associations, we can pursue mechanisms in future studies with larger sample sizes. We stress that our data are within the range of normative variability and are best interpreted in the context of guidance for reductions in maternal stress during current and future population-level stressors.
Limitations
Our sample size was robust to variability in pandemic-related stress levels in new mothers. However, the sample size did not allow probing the precise sources of stress that might have been most impactful for mothers and valuable for shaping infant temperament (social deprivation, job loss, illness etc.). Moreover, our data do not include maternal or infant cortisol levels or prenatal stress levels. As such, we can only speculate about the mechanisms by which maternal stress impacts infant temperament. Finally, the temperament scale was based on maternal report, as in-person assessments were not possible. Hence, the associations reported here among maternal report measures may be influenced by shared method variance or a common informant. Previous studies examining correlations between laboratory-observation temperament measures and IBQ-R have found correlations between parent report of negative emotionality, but less so for positive affect.29,40 However, the authors interpreted their data to mean that certain temperament dimensions might be problematic for the observational rather than maternal-report methods. Such methods involve brief observation at a single point in time when infants are in a strange laboratory context. This scenario might actually be distressing for infants, thereby leading to difficulty in eliciting pleasure but ease of eliciting negative emotionality, the latter of which does indeed correlate with parent report.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Ollivier, R. et al. Mental health & parental concerns during Covid-19: the experiences of new mothers amidst social isolation. Midwifery 94, 102902 (2021).
Wastnedge, E. A. et al. Pregnancy and Covid-19. Physiol. Rev. 101, 303–318 (2021).
Taubman-Ben-Ari, O. & Ben-Yaakov, O. Distress and apprehension among new parents during the Covid-19 pandemic: the contribution of personal resources. Am. J. Orthopsychiatry 90, 810 (2020).
Prime, H., Wade, M. & Browne, D. T. Risk and resilience in family well-being during the Covid-19 pandemic. Am. Psychol. 75, 631 (2020).
Rothbart, M. K. Temperament, development, and personality. Curr. Direct. Psychol. Sci. 16, 207–212 (2007).
Gartstein, M. A. & Rothbart, M. K. Studying infant temperament via the Revised Infant Behavior Questionnaire. Infant Behav. Dev. 26, 64–86 (2003).
Gartstein, M. A., Knyazev, G. G. & Slobodskaya, H. R. Cross-cultural differences in the structure of infant temperament: United States of America (US) and Russia. Infant Behav. Dev. 28, 54–61 (2005).
Putnam, S. P., Ellis, L. K. & Rothbart, M. K. The structure of temperament from infancy through adolescence. Adv. Res. Temperam. 165, 182 (2001).
Putnam, S. P., Rothbart, M. K. & Gartstein, M. A. Homotypic and heterotypic continuity of fine‐grained temperament during infancy, toddlerhood, and early childhood. Infant Child Dev. 17, 387–405 (2008).
Rothbart, M. K., Ahadi, S. A. & Evans, D. E. Temperament and personality: origins and outcomes. J. Pers. Soc. Psychol. 78, 122 (2000).
Karimi-Zarchi, M. et al. Vertical transmission of coronavirus disease 19 (Covid-19) from infected pregnant mothers to neonates: a review. Fetal Pediatr. Pathol. 39, 246–250 (2020).
Kyle, M. H. et al. A review of newborn outcomes during the COVID-19 pandemic. Semin. Perinatol. 44, 151286 (2020).
Liu, W. et al. Clinical characteristics of 19 neonates born to mothers with Covid-19. Front. Med. 14, 193–198 (2020).
Boulanger-Bertolus, J., Pancaro, C. & Mashour, G. A. Increasing role of maternal immune activation in neurodevelopmental disorders. Front. Behav. Neurosci. 12, 230 (2018).
Laplante, D. P., Brunet, A. & King, S. The effects of maternal stress and illness during pregnancy on infant temperament: project ice storm. Pediatr. Res. 79, 107–113 (2016).
Dombrowski, S. C., Martin, R. P. & Huttunen, M. O. Association between maternal fever and psychological/behavior outcomes: a hypothesis. Birth Defects Res. Part A 67, 905–910 (2003).
Boksa, P. Effects of prenatal infection on brain development and behavior: a review of findings from animal models. Brain Behav. Immun. 24, 881–897 (2010).
Schwartz, D. A. & Graham, A. L. Potential maternal and infant outcomes from coronavirus 2019-Ncov (Sars-Cov-2) infecting pregnant women: lessons from SARS, MERS, and other human coronavirus infections. Viruses 12, 194 (2020).
Di Mascio, D. et al. Outcome of coronavirus spectrum infections (Sars, Mers, Covid-19) during pregnancy: a systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2, 100107 (2020).
Felitti, V. J. et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the Adverse Childhood Experiences (Ace) Study. Am. J. Prev. Med. 14, 245–258 (1998).
Pesonen, A.-K., Räikkönen, K., Strandberg, T. E. & Järvenpää, A.-L. Continuity of maternal stress from the pre-to the postnatal period: associations with infant’s positive, negative and overall temperamental reactivity. Infant Behav. Dev. 28, 36–47 (2005).
Bush, N. R. et al. Effects of pre-and postnatal maternal stress on infant temperament and autonomic nervous system reactivity and regulation in a diverse, low-income population. Dev. Psychopathol. 29, 1553–1571 (2017).
Rodríguez‐Soto, N. C. et al. The impact of prenatal maternal stress due to potentially traumatic events on child temperament: a systematic review. Dev. Psychobiol. 63, e22195 (2021).
Provenzi, L. et al. Hidden pandemic: Covid-19-related stress, SLC6A4 methylation and infants’ temperament at 3 months. Sci. Rep. 11, 15658 (2021).
Provenzi, L. et al. Prenatal maternal stress during the Covid-19 pandemic and infant regulatory capacity at 3 months: a longitudinal study. Dev. Psychopathol. https://doi.org/10.1017/S0954579421000766 (2021).
Cohen, S., Kamarck, T. & Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 24, 385–396 (1983).
Lee, E.-H. Review of the psychometric evidence of the Perceived Stress Scale. Asian Nurs. Res. 6, 121–127 (2012).
Putnam, S. P., Helbig, A. L., Gartstein, M. A., Rothbart, M. K. & Leerkes, E. Development and assessment of Short and Very Short Forms of the Infant Behavior Questionnaire–Revised. J. Pers. Assess. 96, 445–458 (2014).
Parade, S. H. & Leerkes, E. M. The reliability and validity of the Infant Behavior Questionnaire-Revised. Infant Behav. Dev. 31, 637–646 (2008).
Evans, D. E. & Rothbart, M. K. Developing a model for adult temperament. J. Res. Pers. 41, 868–888 (2007).
Weathers, F. W. et al. The Life Events Checklist for Dsm-5 (Lec-5)–Standard. [Measurement Instrument]. https://www.ptsd.va.gov/ (2013).
Mäntymaa, M., Puura, K., Luoma, I., Salmelin, R. K. & Tamminen, T. Mother’s early perception of her infant’s difficult temperament, parenting stress and early mother–infant interaction. Nord. J. Psychiatry 60, 379–386 (2006).
Krol, K. M., Moulder, R. G., Lillard, T. S., Grossmann, T. & Connelly, J. J. Epigenetic dynamics in infancy and the impact of maternal engagement. Sci. Adv. 5, eaay0680 (2019).
Leerkes, E. M. & Zhou, N. Maternal sensitivity to distress and attachment outcomes: interactions with sensitivity to nondistress and infant temperament. J. Fam. Psychol. 32, 753 (2018).
Grey, K. R., Davis, E. P., Sandman, C. A. & Glynn, L. M. Human milk cortisol is associated with infant temperament. Psychoneuroendocrinology 38, 1178–1185 (2013).
Chronis-Tuscano, A. et al. Stable early maternal report of behavioral inhibition predicts lifetime social anxiety disorder in adolescence. J. Am. Acad. Child Adolesc. Psychiatry 48, 928–935 (2009).
Clauss, J. A. & Blackford, J. U. Behavioral inhibition and risk for developing social anxiety disorder: a meta-analytic study. J. Am. Acad. Child Adolesc. Psychiatry 51, 1066–1075. e1061 (2012).
Henderson, H. A., Pine, D. S. & Fox, N. A. Behavioral inhibition and developmental risk: a dual-processing perspective. Neuropsychopharmacology 40, 207–224 (2015).
Lahey, B. B. et al. Temperament and parenting during the first year of life predict future child conduct problems. J. Abnorm. child Psychol. 36, 1139–1158 (2008).
Gartstein, M. A. & Marmion, J. Fear and positive affectivity in infancy: convergence/discrepancy between parent-report and laboratory-based indicators. Infant Behav. Dev. 31, 227–238 (2008).
Funding
This work is supported by R01MH126531 to D.D., C.M., and R.M. and NSF-2051819 to D.A. This work was also in part funded by gift funds from Einhorn Collaborative to the Nurture Science Program at Columbia University Irving Medical Center.
Author information
Authors and Affiliations
Contributions
Substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data: C.B., A.S., M.H.K., B.B., J.B., M.B., L.C., A.F., M.R.F., S.G., A.H., V.H., M.H., S.H., M.L., R.M., I.M., M.M., D.O., N.P., C.R., L.C.S., N.T., M.G.W., W.F., C.M., D.D., D.A. Drafting the article or revising it critically for important intellectual content: C.B., A.S., D.D., D.A. Approval of the version to be published: C.B., A.S., M.H.K., B.B., J.B., M.B., L.C., A.F., M.R.F., S.G., A.H., V.H., M.H., S.H., M.L., R.M., I.M., M.M., D.O., N.P., C.R., L.C.S., N.T., M.G.W., W.F., C.M., D.D., D.A.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
All study participants completed consent forms prior to participation following guidelines of the CUIMC Institutional Review Board.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Bianco, C., Sania, A., Kyle, M.H. et al. Pandemic beyond the virus: maternal COVID-related postnatal stress is associated with infant temperament. Pediatr Res 93, 253–259 (2023). https://doi.org/10.1038/s41390-022-02071-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-022-02071-2
This article is cited by
-
Temperament and adolescent suicide attempts: a case-control study with multi-ethnic Asian adolescents
BMC Psychiatry (2023)
-
Effects of prenatal psychosocial stress and COVID-19 infection on infant attention and socioemotional development
Pediatric Research (2023)
-
Maternal perceived stress and infant behavior during the COVID-19 pandemic
Pediatric Research (2023)
