
Abstract
Background
Fecal calprotectin (FC) is a marker of mucosal inflammation in inflammatory bowel disease (IBD). We aimed to assess the effect of anti-tumor necrosis factor alpha (TNFα) therapy on FC levels in children with IBD.
Methods
The medical records of pediatric patients treated with anti-TNFα agents (2015–2020) were reviewed retrospectively. 63 patients had FC levels measured prior to anti TNFα induction with sequential measurements during follow-up. The main outcome measures were time to FC response according to cutoffs of 250, 150, 100 and 50 µgr/gr.
Results
Mean age was 13.6 ± 3 years [females 28 (44.4%), Crohn’s 55 (87%)]. Outcomes of < 250, < 150, < 100 and < 50 µgr/gr were achieved by 52 (82%), 51 (81%), 44 (70%) and 32 (50%), respectively. The median time for achieving these cutoffs was 4.8 (1.8–15.6), 7.9 (2.6–16.4), 10.0 (3.5–20.5) and 18.5 (7.0–64.7) months, respectively. Shorter time from diagnosis to treatment was associated with achievement of FC < 50 µgr/gr (p = 0.03). There was no association between age, disease type, anti-TNFα type, inflammatory markers, disease activity indices at baseline and induction anti-TNFα trough concentration and FC response.
Conclusions
FC response was achieved by the majority of patients treated with anti-TNFα within a short period of time. FC normalization in responders required almost one year.
Impact
-
Fecal calprotectin response was achieved by the majority of pediatric patients within a relatively short period of time after anti-TNFα induction and maintenance therapy.
-
Fecal calprotectin normalization required an average period of approximately one year in responders.
-
The faster response of fecal calprotectin is associated with shorter time from diagnosis to anti-TNFα treatment.
-
Inflammatory bowel disease treating physicians should be aware of the relatively prolonged time to fecal calprotectin normalization and to allow enough time for anti-TNFα therapy to express its full potential prior to significant interventions
Similar content being viewed by others
Introduction
Inflammatory bowel disease (IBD) in both adults and children are increasingly managed with biologic agents, predominantly with anti-tumor necrosis factor alpha (TNFα). The current practice has gradually transformed and adopted treat to target strategies seeking for mucosal healing (MH) which was clearly shown to improve the odds for sustained clinical remission and results in better short- and long-term clinical outcomes in both Crohn’s disease (CD) and ulcerative colitis (UC).1,2 Colonoscopy has been considered as the most accurate diagnostic modality for evaluating MH in IBD; however, being an invasive, uncomfortable and sometimes risky procedure, especially in children, fecal calprotectin (FC) is frequently used as a surrogate marker to monitor mucosal response to treatment.3 FC levels are associated with endoscopic disease indices in patients with IBD, regardless of the type of disease4 and are able to discriminate between mild, moderate and severe disease.5,6
It was previously shown that FC levels ≤ 250 µgr/gr predicts endoscopic remission with relatively high sensitivity and moderate specificity3 but other cutoffs such as 150 µgr/gr have been suggested.7 Nevertheless, more than few studies have demonstrated that lower cutoff values in the range of 50–100 μgr/gr may be required for more accurately predicting complete absence of mucosal inflammatory activity8 or deep healing9 (defined as both mucosal and transmural healing).
It is not clear how rapidly FC responds to any treatment (including anti-TNFα) and thus when to expect FC response or normalization. In a recent pediatric cohort in which most patients were not treated with anti-TNFα agents, the median time-to-reach FC response was 37 weeks in patients with CD and 11 weeks in patients with UC.10
Therefore, our aim in this study was to assess the effect of anti-TNFα induction and maintenance therapy on FC levels in children with IBD and to evaluate potential variables affecting FC response during anti-TNFα treatment.
Materials and methods
Patients
Data were retrieved retrospectively from structured computerized medical records of pediatric patients (aged 0–18 years) diagnosed with IBD, treated with infliximab (IFX) or adalimumab (ADL) and were followed between 2015 - 2020 at the Schneider Children’s Medical Center. Pediatric IBD diagnosis was based on clinical, endoscopic radiologic, and histologic criteria.11 We included patients with CD and UC who initiated anti-TNFα induction and maintenance prior to 18 years of age, completed at least 3 induction doses of IFX or 2 induction doses of ADL, continued maintenance anti-TNFα therapy and had a baseline FC level prior (up to 30 days) or at time of anti-TNFα initiation. Patients were either naïve to anti-TNFα therapy or switched from anti-TNFα to a subsequent anti-TNFα. The standard IFX induction protocol consisted of 3 infusions of 5 mg/kg/dose at weeks 0, 2, and 6, followed by maintenance infusions every 8 weeks in responders, while ADL was administered as subcutaneous injections every 2 weeks as follows: patients weighing ≥ 40 kg received 2 induction doses of 160 mg and 80 mg with a maintenance dose of 40 mg thereafter, whereas patients < 40 kg received 100 mg/m2 of body surface area (BSA) and 50 mg/m2 BSA as 2 doses of induction treatment and 25 mg/m2 BSA as maintenance.
Description of variables
For each patient demographic characteristic, type of disease, Paris classification, extra-intestinal manifestations, albumin levels, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), Pediatric Crohn’s disease activity index (PCDAI) and Pediatric ulcerative colitis activity index (PUCAI) were retrieved at baseline. FC level, Anti-TNFα trough concentrations (TC), CRP, and disease activity indices during maintenance therapy were assessed during each visit. PCDAI and PUCAI were analyzed together for convenience because of the small sample size of patients with UC and due to the fact that clinical remission is defined by the same threshold (< 10 points) for both indices. Visits were scheduled for each infusion in IFX treated patients and for week 0, 4, 8 and every 8 weeks for ADL treated patients. Patients were requested to collect FC fecal samples for each visit. Induction was defined as 3 infusions of IFX or 2 injections of ADL. Anti-TNF response was defined as an achievement of clinical remission (PCDAI or PUCAI < 10 points) during follow up. The main outcome was time to FC response according to cutoffs of 250,150 µgr/gr and normalization cutoffs of 100 and 50 µgr/gr. Time of follow-up was defined as time until achievement of the stricter cutoff of 50 µgr/gr or end of follow-up if this outcome was not achieved. The end of the follow-up period for patients who did not achieve FC of < 50 mcg/ml was defined as the time of last FC measurement following anti-TNFα initiation.
Fecal samples for calprotectin were analyzed using chemiluminescent immunoassay (CLIA) (Liaison® Calprotectin - Diasorin®, Saluggia, Italy). Up to December 2017, IFX and ADL trough concentrations (TCs) were performed at a central laboratory (Sheba Gastroenterology Laboratory, Ramat-Gan, Israel) using enzyme-linked immunosorbent assay (ELISA).12 From January 2018, IFX and ADL TCs were analyzed using a commercial assay by Theradiag Beaubourg, France, at the Rabin Medical Center laboratory. Drug TC values at both labs are measured by the same scale.
Statistical analysis
Continuous variables were displayed as mean and standard deviation or as a median and interquartile range depending on their normal distribution. Categorical variables were described using frequency incidence. Kaplan-Meier curves were used to describe the time dependent response of FC. The variables were compared using Mann-Whitney tests or T-test for continuous variables and using Chi-square or Fisher exact tests for categorical variables. Association of different variables and changes of FC were analyzed using Cox regression analysis. P-values < 0.05 were considered significant. Data were analyzed using SPSS (IBM SPSS statistics, version 25.0, IBM Corp., Armonk, NY).
Ethical considerations
The study protocol was approved by the local Internal Review Board at the Rabin/Schneider Medical Center (RMC0320-10).
Results
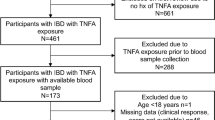
Out of 135 patients with IBD treated with anti-TNFα agents during the study period, 63 patients were eligible for analysis according to the study inclusion criteria and had subsequent measurements of FC at the defined scheduled visits. The mean age of the cohort was 13.6 ± 3.0 years [females 28 (44%), CD 55 (87%)]. Thirty-two patients (51%) were treated with IFX and 27 (43%) were on concomitant therapy with immunomodulators. Out of these 27 patients, only 3 (4.7%) were on concomitant therapy of an immunomodulator and ADL. Two patients were included following a switch within the anti-TNFα class: One switch from IFX to ADL due to acute infusion reaction and one switch from ADL to IFX due to primary non-response. Only the second anti-TNFα term was eligible for inclusion in both patients. The median follow-up time (interquartile range, IQR) was 2.2 years (0.9–3.1) and the cohort yielded a total of 463 measurements of FC (a mean of 7.3 ± 1.8 FC measurements per patient). The median (IQR) FC at baseline was 715 µgr/gr (312–1700). Out of the 63 patients, 61 (96%) were anti-TNFα naïve and 40 (63%) patients were in top-down anti-TNFα therapy with no prior treatment. The demographic characteristics of the cohort at baseline were summarized in Table 1.
The outcomes of FC levels < 250, < 150, < 100 and < 50 µgr/gr were achieved by 52 (84%), 51 (81%), 44 (70%) and 32 (50%) patients, respectively. The median time (IQR) for achieving these cutoffs was 4.8 (1.8–15.6), 7.9 (2.6–16.4), 10.0 (3.5–20.5) and 18.5 (7.0–64.7) months, respectively (Fig. 1a–d demonstrate the Kaplan-Meier curves of time to FC response). Only 5 (8%) patients did not normalize their CRP level during follow-up while the median (IQR) time to CRP normalization was 0.65 (0.1–1.4) months. There was no statistically significant association between age at diagnosis, sex, type of disease, type of anti-TNFα agent, Paris classification, extra-intestinal manifestations, albumin levels, ESR, CRP and the pediatric disease activity indices at baseline and subsequent FC response (Table 2). Shorter time from diagnosis to initiation of anti-TNFα was associated with the achievement of FC < 50 µgr/gr (p = 0.03). Baseline FC did not correlate with time to FC response. Patients with baseline FC of > 1000 µgr/gr showed no difference in time to the defined FC targets compared with patients with lower baseline FC (p-value of 0.7–0.9 for all FC targets). Analyses of different thresholds of baseline FC did not yield significant differences (data not shown).

The cutoff of a 250 μgr/gr, b 150 μgr/gr, c 100 μgr/gr, d 50 μgr/gr.
Eight patients had never achieved clinical remission during follow-up. Out of these, 6 (75%) never had an FC response. Out of 63 patients, 18 (29%) patients underwent dose increase or interval shortening during follow-up. More patients in the escalation group did not achieve FC response of < 250 µgr/gr (7/18, 39% in the treatment escalation group and 3/45, 7% in the non-escalation group, p = 0.002). Eleven patients (61%) in the escalation group achieved FC response following treatment adjustment. In patients who required treatment escalation, the achievement of the <250 µgr/gr target trended towards a longer period of time [median 5.1 months (IQR 2.2–23.0) vs. 2.5 (IQR 1.3–7.5)] but without statistical significance (p = 0.09).
Out of the 52 patients who achieved the outcome of FC <250 µgr/gr, 21 (40%) increased their FC levels above 250 µgr/gr after a median of 2.7 (IQR 1.4–37) months. For those patients, the median time for reduction of FC < 250 µgr/gr was 4.5 months (IQR 1.5–15.6), p = 0.49. Re-reduction of FC was observed either spontaneously or following treatment escalation in all patients. None of the analyzed variables predicted re-elevation of FC levels.
Six out of 21 (28.5%) who had worsening FC ( > 250 µcg/gr) had clinical loss of response and all underwent anti-TNFα escalation as a result of FC increase.
Mean anti-TNFα TC at the end of induction (prior to the 4th IFX infusion and 3rd ADL injection) was 11.2 ± 7.8 µgr/ml. Neither concomitant immunomodulatory (IM) drugs use nor anti-TNFα trough concentration during induction and maintenance therapy showed any statistically significant associations with FC response [(p = 0.26, 0.81, 0.09 and 0.50) or (p = 0.90, 0.27, 0.44 and 0.94), respectively according to the defined cutoffs of <250 < 150, < 100 and < 50 µgr/gr].
FC normalization (<100 µgr/gr) at the end of induction was associated with shorter time from diagnosis to initiation of anti-TNFα therapy (4.3 ± 4.7 months vs. 15.8 ± 16.7 months, p = 0.04 for responders and non-responders, respectively). In contrast, FC response or normalization at the end of induction was not associated with any of the other analyzed variables at baseline. Anti-TNFα TC at the end of induction did not differ between those who did or did not achieve the < 250 µgr/gr and < 100 µgr/gr outcomes (9.7 ± 6.0 µgr/ml vs. 11.4 ± 11.7 µgr/ml, p = 0.61 and 9.4 ± 5.0 µgr/ml vs 8.2 ± 5.5 µgr/ml, p = 0.58), respectively.
During maintenance there was a positive association between FC response and changes in CRP and disease activity indices. At the median time for FC response (< 250 µgr/gr) mean CRP in non-responders was 2.86 ± 3.3 mg/dl vs. 0.18 ± 0.28 mg/dl in responders (p < 0.001). A similar association was observed for all cutoffs (2.3 ± 2.9 mg/dl vs. 0.16 ± 0.25 mg/dl for FC < 150 µgr/gr, p < 0.001; 1.5 ± 2.5 mg/dl vs. 0.33 ± 0.32 mg/dl for FC < 100 µgr/gr, p = 0.003 and 1.5 ± 2.9 mg/dl vs. 0.1 ± 0.1 mg/dl for FC < 50 µgr/gr, p = 0.009). Overall, there was a significant association between CRP levels and FC levels (P = 0.01). Mean disease activity index differed significantly between responders and non-responders for all cutoffs (p < 0.001 at all time points). There was no difference in anti-TNFα TC between responders and non-responders for all cutoffs at all time points with an overall mean trough concentrations of 10.8 ± 5.9, 11.1 ± 6.1, 10.0 ± 6.1 and 10.5 ± 6.0 µgr/ml for FC < 250, < 150, < 100 and < 50 µgr/gr.
Discussion
In this study, we aimed to assess the effect of anti-TNFα induction and maintenance therapy on FC levels in children with IBD. We observed that FC response from baseline, defined by the less stringent cutoff of < 250 µgr/gr, was achieved by the majority of patients within a relatively short period of time following anti-TNFα initiation (approximately 5 months), though much later than normalization of CRP (approximately 3 weeks) emphasizing that the resolution of systemic inflammation precedes mucosal response and that mucosal inflammation frequently persists despite resolution of systemic inflammation. We also demonstrated that 70% of patients gradually normalized their FC levels (defined as < 100 µgr/gr) but this process lasted almost one year. There are only scarce data on the evolution of FC response in anti-TNFα treated patients. Several adult studies have reported a rapid decline in FC following anti-TNFα induction. Sipponen et al. showed that at week 12 of IFX therapy in patients with CD, median FC fell from 1173 µgr/gr to 130 µgr/gr.13 Molander et al. reported normalization of FC ( < 100 μgr/gr) in 52% of patients with CD at the end of IFX induction.6 In UC, De Vos et al. demonstrated a decrease in FC from 1260 µgr/gr at baseline to 72.5 µgr/gr at week 10 while in 58% of patients, calprotectin fell to < 50 µgr/gr or at least dropped by 80% from baseline level.14
In a recent pediatric cohort of 76 newly diagnosed patients10 mostly treated with corticosteroids/exclusive enteral nutrition followed by immunomodulators for CD and aminosalicylic acid with or without thiopurines for UC, the median time-to-reach FC of ≤ 250 µgr/gr was 37 weeks in patients with CD and 11 weeks in patients with UC. Very few patients in this cohort were treated with anti-TNFα agents. Based on our findings, it may be implied not only that anti-TNFα agents are much more efficacious than other induction agents (a well-established finding) but that anti-TNFα responders achieve mucosal response and healing much faster than other “step-up” induction strategies despite the more severe and refractory status of anti-TNFα treated patients at treatment initiation. IBD treating physicians should be aware of the relatively prolonged time to FC normalization allowing enough time for anti-TNFα therapy to express its full potential prior to significant interventions. Unlike the study by Haisma et al. we did not find a difference in time to FC response between patients with CD and UC. This discrepancy could be attributed to the fact that the eight patients with UC in our cohort were with severe disease compared to mild to moderate disease in the majority of patients in Haisma’s cohort.
It was consistently shown that FC levels correlate with endoscopic disease activity in both CD and UC.15,16 It was also demonstrated that a calprotectin < 250 µgr/gr identified mucosal healing with 94% sensitivity and 62% specificity in patients with CD4 while a cutoff value of 150 µgr/gr yielded sensitivity and specificity of 79% and 75% for endoscopic remission, respectively, in UC.17 In recent years, lower cutoffs were associated with potentially new therapeutic targets combining mucosal and histologic healing or combining mucosal and transmural healing (particularly in CD). In a pediatric cohort of 151 patients with CD, a calprotectin cutoff value of 100 μgr/gr identified children with deep healing (defined as mucosal and transmural healing) with 71% sensitivity and 92% specificity.18 For UC, a cutoff of 100 μgr/gr, resulted in sensitivity and specificity of 82.4% and 60.9%, respectively, for deep mucosal remission (mucosal and histologic healing).19 In a mixed CD and UC cohort, FC below 56 µgr/gr was found to optimally predict absence of relapse during follow-up with 64% sensitivity, 100% specificity, 100% negative predictive value and 20% positive predictive value.9 It is thus suggested that striving for FC within the normal limit (generally < 100 µgr/gr) carries substantial long-term benefits. Nevertheless, we have demonstrated that achieving such FC target requires a much longer period of time under anti-TNFα treatment. Interestingly, 70% of our cohort achieved this stringent target, reflecting the efficacy of anti-TNFα treatment. Achieving the lowest cutoff of 50 µgr/gr, in our cohort, was associated with shorter time from diagnosis to anti-TNFα treatment. This finding is in accordance with studies that demonstrated that biologic therapy early in the course of disease results in better short- and long-term outcomes in both adults20,21 and children.22 Interestingly, higher FC prior to treatment initiation did not correlate with faster time of FC response. This finding may be attributed to the low specificity of FC3 and to the fact even patients with high inflammatory burden respond rapidly to anti-TNFα treatment.7,21
We also observed that no other variables at baseline were associated with FC response, such as age at diagnosis, age at treatment initiation, sex, type of disease, type of anti-TNFα agent, disease characteristics (location, behavior), the presence of perianal CD, extra-intestinal manifestations, serum biomarkers and disease activity indices. Prediction of mucosal healing at treatment initiation is difficult. In contrast to our findings, CRP at baselines was shown to be associated with maintenance endoscopic activity in CD23 while ileal disease location was suggested to be associated with lower mucosal healing rates.24
The reported association between CRP values, activity indices and FC levels during maintenance in the current cohort are expected and in line with previous studies.25,26
Data on the association between anti-TNFα TCs and decrease in FC is accumulating though conflicting. In a recent pharmacokinetic study which included 56 adult patients with CD, end of induction IFX TC of > 9.4 µg/mL (area under the receiver operating characteristic, AUROC, curve of 0.799) and > 11.5 µg/mL (AUROC curve of 0.835) were associated with a FC < 250 and FC < 100 µgr/gr, respectively.27 In contrast, in a pediatric randomized controlled trial, ADL TCs were not associated with FC values.25 In endoscopic based studies, anti-TNFα TC was shown to be directly associated with mucosal healing in both adults28 and children.29 Furthermore, it is well established that at least for IFX, combination with an immunomodulator increases the odds of better endoscopic outcomes.30 The absence of an effect of either anti-TNFα TCs or combination therapy on the study outcomes in our cohort could have been attributed to the standard of care in our center which is based on proactive therapeutic drug monitoring aiming for relatively high TC which is reflected by the high mean TC of more than 10 µgr/ml at all study’s time points. It was recently shown that optimized infliximab monotherapy, resulting in higher TCs, is as effective as combination therapy in adult patients with IBD.31 It is important to note that the most frequent reason for treatment intensification in our cohort was lack of FC response and that treatment adjustment resulted in 61% of patients achieving FC < 250 µgr/gr. This finding is in line with previous reports demonstrating similar response to treatment optimization.32 It is also worth noting that 40% of patients who achieved FC response had a relatively rapid re-elevation of FC, sometimes requiring further treatment adjustment, with re-reduction of FC either spontaneously or following intervention in all patients, reflecting both the variability of FC measurements and the efficacy of treatment optimization.
The strengths of this study derive from the stringent scheduled measurement of FC and anti-TNFα TCs. The study is limited by its retrospective nature affecting the ability to retrieve complete comprehensive data and predominantly by the lack of endoscopic evaluation and/or cross-sectional imaging which could have enabled a more accurate interpretation of the study results. Moreover, it was consistently shown that FC has a low to moderate specificity and high variability, thus it cannot reflect accurately the mucosal response to treatment in some patients.
In conclusion, in pediatric patients with IBD, FC response (< 250 mg/kg) was achieved by the majority of patients within a relatively short period of time. Nevertheless, FC normalization (<100 mg/kg) required an average period of approximately one year in responders but was achieved, again, by most patients. Anti-TNFα TCs were not associated with FC response. Further studies with scheduled repeated FC measurements are required to explore variables associated with FC evolution over time.
References
Carvalho, P. B. & Cott, J. Mucosal healing in ulcerative colitis: A comprehensive review. Drugs 77, 159–173 (2017).
Schnitzler, F. et al. Mucosal healing predicts long-term outcome of maintenance therapy with infliximab in Crohn’s disease. Inflamm. Bowel Dis. 15, 1295–1301 (2009).
Koninckx, C. R. et al. The use of fecal calprotectin testing in paediatric disorders: A position paper of the European society for paediatric gastroenterology and nutrition gastroenterology committee. J. Pediatr. Gastroenterol. Nutr. 72, 617–640 (2021).
D’Haens, G. et al. Faecal calprotectin is a surrogate marker for endoscopic lesions in inflammatory bowel disease. Inflamm. Bowel Dis. 18, 2218–2224 (2012).
Schoepfer, A. M. et al. Fecal calprotectin more accurately reflects endoscopic activity of ulcerative colitis than the Lichtiger index, C-reactive protein, platelets, hemoglobin, and blood leukocytes. Inflamm. Bowel Dis. 19, 332–341 (2013).
Schoepfer, A. M. et al. Ulcerative colitis: Correlation of the Rachmilewitz endoscopic activity index with fecal calprotectin, clinical activity, C-reactive protein, and blood leukocytes. Inflamm. Bowel Dis. 15, 1851–1858 (2009).
Molander, P. et al. Faecal calprotectin concentration predicts outcome in inflammatory bowel disease after induction therapy with TNFα blocking agents. Inflamm. Bowel Dis. 18, 2011–2017 (2012).
Jusué, V., Chaparro, M. & Gisbert, J. P. Accuracy of fecal calprotectin for the prediction of endoscopic activity in patients with inflammatory bowel disease. Dig. Liver Dis. 50, 353–359 (2018).
Mooiweer, E. et al. Low fecal calprotectin predicts sustained clinical remission in inflammatory bowel disease patients: A plea for deep remission. J. Crohns Colitis 9, 50–55 (2015).
Haisma, S. M. et al. Time-to-reach target calprotectin level in newly diagnosed patients with inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 69, 466–473 (2019).
Levine, A. et al. Pediatric modification of the Montreal classification for inflammatory bowel disease: The Paris classification. Inflamm. Bowel Dis. 17, 1314–1321 (2011).
Ben-Horin, S. et al. The immunogenic part of infliximab is the F(ab’)2, but measuring antibodies to the intact infliximab molecule is more clinically useful. Gut 60, 41–48 (2011).
Sipponen, T. et al. Fecal calprotectin, lactoferrin and endoscopic disease activity in monitoring anti-TNF-alpha therapy for Crohn’s disease. Inflamm. Bowel Dis. 14, 1392–1398 (2008).
De Vos, M. et al. Fast and sharp decline in calprotectin predicts remission by infliximab in anti-TNF naïve patients with ulcerative colitis. J. Crohns Colitis 6, 557–562 (2012).
Schoepfer, A. M. et al. Fecal calprotectin correlates more closely with the Simple Endoscopic Score for Crohn’s disease (SES-CD) than CRP, leukocytes and the CDAI. Am. J. Gastroenterol. 105, 162–169 (2010).
Hart, L. et al. Faecal calprotectin predicts endoscopic and histological activity in clinically quiescent ulcerative colitis. J. Crohns Colitis 14, 46–52 (2020).
Sandborn, W. J. et al. Correlation between concentrations of fecal calprotectin and outcomes of patients with ulcerative colitis in a phase 2 trial. Gastroenterology 150, 96–102 (2016).
Weinstein-Nakar, I. et al. Associations among mucosal and transmural healing and faecal level of calprotectin in children with Crohn’s disease. Clin. Gastroenterol. Hepatol. 16, 1089–1097 (2018).
Malvão, L. D. R. et al. Fecal calprotectin as a noninvasive test to predict deep remission in patients with ulcerative colitis. Medicine (Baltimore). Dec 31. online ahead of print (2021).
Baert, F. et al. Mucosal healing predicts sustained clinical remission in patients with early-stage Crohn’s disease. Gastroenterology 138, 463–468 (2010).
Singh, H., Nguyen, T., Pho, C. & Giles, E. Early Infliximab in Crohn’s is associated with decreased intestinal surgery and similar health care costs. Scand. J. Gastroenterol. 56, 397–402 (2021).
Jongsma M., et al. First-line treatment with infliximab versus conventional treatment in children with newly diagnosed moderate-to-severe Crohn’s disease: An open-label multicentre randomised controlled trial. GUT 2020. Dec 31. Online ahead of print.
Naganuma, M. et al. Endoscopic severity predicts long-term prognosis in Crohn’s disease patients with clinical remission. Digestion 93, 66–71 (2016).
Rivière, P. et al. Location but not severity of endoscopic lesions influences endoscopic remission rates in Crohn’s disease: A post hoc analysis of TAILORIX. Am. J. Gastroenterol. 116, 134–141 (2021).
Assa, A. et al. Proactive monitoring of adalimumab trough concentration associated with increased clinical remission in children with Crohn’s disease compared with reactive monitoring. Gastroenterology 157, 985–996 (2019).
Reinisch, W. et al. Association of biomarker cutoffs and endoscopic outcomes in Crohn’s disease: A post hoc analysis from the CALM study. Inflamm. Bowel Dis. 26, 1562–1571 (2020).
Colman, R. J. et al. Achieving target infliximab drug concentrations improves blood and fecal neutrophil biomarkers in Crohn’s disease. Inflamm. Bowel Dis. 27, 1045–1051 (2021).
Papamichael, K., Rakowsky, S., Rivera, C., Cheifetz, A. S. & Osterman, M. T. Association between serum infliximab trough concentrations during maintenance therapy and biochemical, endoscopic, and histologic remission in Crohn’s disease. Inflamm. Bowel Dis. 24, 2266–2271 (2018).
Kang, B. et al. Infliximab Trough Levels Are Associated With Mucosal Healing During Maintenance Treatment With Infliximab in Paediatric Crohn’s Disease. J. Crohns Colitis 13, 189–197 (2019).
Colombel, J. F. et al. Infliximab, azathioprine, or combination therapy for Crohn’s disease. N. Engl. J. Med 362, 1383–1395 (2010).
Drobne, D. et al. Optimised infliximab monotherapy is as effective as optimised combination therapy, but is associated with higher drug consumption in inflammatory bowel disease. Aliment Pharm. Ther. 49, 880–889 (2019).
Paul, S. et al. Therapeutic drug monitoring of infliximab and mucosal healing in inflammatory bowel disease: a prospective study. Inflamm. Bowel Dis. 19, 2568–2576 (2013).
Acknowledgements
The statistical analysis was performed by Dr. Tomer Ziv (PhD), statistician, Tel-Aviv University, Tel-Aviv, Israel.
Author information
Authors and Affiliations
Contributions
M.M. and A.A. conceptualized and designed the study; R.L., M.Z., and R.S. participated in designing the study. M.M, R.L., and M.Z. participated in the acquisition of data and analysis and interpretation of data. A.A. and M.M. drafted the manuscript. All authors critically revised the manuscript and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent statement
The study protocol was approved by the local Institutional Review Board at the Rabin/Schneider Medical Center. Patient consent was not required.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This work is original, not previously published, and not submitted for publication or consideration elsewhere.
Rights and permissions
About this article

Cite this article
Matar, M., Levi, R., Zvuloni, M. et al. Pediatric inflammatory bowel disease: Fecal calprotectin response to Anti-tumor necrosis factor alpha. Pediatr Res 93, 131–136 (2023). https://doi.org/10.1038/s41390-022-02045-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-022-02045-4
This article is cited by
-
Adalimumab/infliximab
Reactions Weekly (2024)
