
Abstract
Background
Life course studies are designed to “collect once, use multiple times” for observational and, increasingly, interventional research. Core Outcome Sets (COS) are minimum sets developed for clinical trials by multi-stakeholder consensus methodologies. We aimed to synthesize published COS that might guide outcomes selection for early life cohorts with an interventional focus.
Methods
We searched PubMed, Medline, COMET, and CROWN for COS published before January 2021 relevant to four life stages (pregnancy, newborns, children <8 years, and parents (adults aged 18–50 years)). We synthesized core outcomes into overarching constructs.
Results
From 46 COS we synthesized 414 core outcomes into 118 constructs. “Quality of life”, “adverse events”, “medication use”, “hospitalization”, and “mortality” were consistent across all stages. For pregnancy, common constructs included “preterm birth”, “delivery mode”, “pre-eclampsia”, “gestational weight gain”, “gestational diabetes”, and “hemorrhage”; for newborns, “birthweight”, “small for gestational age”, “neurological damage”, and “morbidity” and “infection/sepsis”; for pediatrics, “pain”, “gastrointestinal morbidity”, “growth/weight”, “breastfeeding”, “feeding problems”, “hearing”, “neurodevelopmental morbidity”, and “social development”; and for adults, “disease burden”, “mental health”, “neurological function/stroke”, and “cardiovascular health/morbidity”.
Conclusion
This COS synthesis generated outcome constructs that are of high value to stakeholders (participants, health providers, services), relevant to life course research, and could position cohorts for trial capabilities.
Impact
-
We synthesized existing Core Outcome Sets as a transparent methodology that could prioritize outcomes for lifecourse cohorts with an interventional focus.
-
“Quality of life”, “adverse events”, “medication use”, “hospitalization”, and “mortality” are important outcomes across pregnancy, newborns, childhood, and early-to-mid-adulthood (the age range relevant to parents). Other common outcomes (such as “birthweight”, “cognitive function/ability”, “psychological health”) are also highly relevant to lifecourse research.
-
This synthesis could assist new early life cohorts to pre-select outcomes that are of high value to stakeholders (participants, health providers, services), are relevant to lifecourse research, and could position them for future trials and interventional capability.
Similar content being viewed by others


Introduction
Life course studies are longitudinal population cohort studies that take an interdisciplinary and holistic view of overall health and social wellbeing, and aim to capture antecedents, characteristics. and events on the path to key health outcomes.1 Designed to “collect once, use multiple times”, they are increasingly intended to support interventional as well as observational research and to increase the return on investment in research.2 A strength is their ability to address multiple hypotheses as they arise—meaning that outcomes must effectively be specified “sight unseen”. Therefore, if life course studies are to support the most impactful research across multiple fields, they need to capture the highest-utility outcomes with the greatest translational potential. However, no systematic methodology exists to prioritize outcomes selection for life course studies. This may be particularly important for new cohorts designing for an interventional capability because trials require clear-cut primary and secondary outcomes that often encompass life course constructs such as quality of life.
This problem has been addressed for clinical trials with the advent of Core Outcome Sets (COS). COS are agreed-upon, standardized minimum sets of outcomes that should be reported in all trials in a particular field.3 COS aim to: (1) increase the relevance and consistency of reported outcomes; (2) facilitate efficient research synthesis and reduce research waste; and (3) reduce selection bias in reported outcomes.3 COS are developed using transparent and rigorous consensus methods typically involving multiple stakeholder groups, usually drawn from multiple countries for maximal international applicability.4 Stakeholders include patients, parents, family members, clinicians, and allied healthcare professionals as well as researchers to ensure that outcomes are meaningful to the end-users of the research.3 While designed to improve the reporting of clinical trial outcomes and enable evidence synthesis, COS are increasingly being used in other types of research including observational studies.5,6 COS could also provide a rigorous and transparent approach to prioritizing and selecting outcomes for life course cohorts planning to embed capabilities for trials.
This review explored the potential of systematically reviewing and synthesizing COS as a means to prioritize and select outcomes for new interventional cohorts in planning. Internationally important cohorts commencing in the last 5 years, notably Born in Bradford Better Start7 and ORIGINS,8 have already demonstrated the appetite for and feasibility of embedding trials in life course cohorts. This review was conducted ahead of Generation Victoria (GenV), a whole-of-state cross-generational cohort in advanced planning in Victoria (population 6.5 million in 20199), Australia. GenV intends to target all 150,000 Victorian newborns and their parents over two full years, from late 2021, with the primary purpose of creating large, parallel whole-of-state birth and parent cohorts for discovery and interventional research (see refs. 10,11 for purpose, design, and procedures). The process of prioritizing and selecting measures12 for GenV begins with identifying important domains and constructs that align with GenV’s life course frameworks,1 are not present in administrative and clinical datasets,13 and could support interventional as well as observational research.
Lacking a clear methodology to achieve this, we designed and undertook the novel conceptualization and systematic review presented in this paper. We reasoned firstly that drawing on COS as one tool for outcomes selection could strengthen causal inference from cohort studies. This could occur not only via embedded trials and other intervention evaluation methodologies but also by enhancing the value of epidemiological techniques such as causal modeling, strengthening the ability of life course cohorts to further knowledge of causation, and solutions.14 Secondly, we reasoned that, although the driver for any given COS is a specific condition, the outcomes that families and services value most would largely not be condition-specific and indeed would show both commonality across COS and relevance to life course research. Thirdly, we believed that this work could be of value to others planning major new birth cohorts internationally, particularly where an international focus is envisaged.
This paper seeks to systematically review COS relevant to life course cohorts, with an initial focus on pregnancy, newborns, early childhood, and adults 18–50 years (the usual age range for parents of young children). It aims to synthesize the core outcomes from existing COS within and across these four life stages, and to identify common, important, and recurring outcomes to be considered for selection in life course studies.
Methods
Where they were applicable to the literature and data, we conducted the review in accordance with the 2020 PRISMA guidelines15 (see Supplementary Material 1 for PRISMA checklist).
Eligibility criteria
Papers eligible for inclusion in this review were completed COS for conditions relevant to four life stages: pregnancy, newborns, children <8 years of age (pediatric), and adults aged 18–50 (the MESH age range relevant to parents of young children, who are often independent participants whose own health and circumstances are tracked in birth cohorts).
Studies were excluded during the title and abstract screening stage if they were preliminary COS research articles or commentary papers, were not in English, or if a full text article could not be sourced. During full text review, we excluded COS that lacked patient/participant involvement, as this is a key component of robust COS development as per the Core Outcome Set-STAnDards for Development (COS-STAD) guidelines.4 We also excluded studies that did not use the Delphi consensus method, a standardized consensus method commonly utilized in COS development. The Delphi method ensures anonymity of stakeholders’ preferences, avoiding stifling of opinion by loud or expert voices, and provides an iterative decision-making process to generate by consensus a final set of priorities that truly represents the priorities of the group.16,17 Lastly, we excluded COS for conditions with an incidence or prevalence of <0.1%, as they would likely affect a very small number of participants in life course studies, which generally aim to create a representative sample of the whole population.
Information sources and search strategy
A search for relevant papers listed in Medline, PubMed, Core Outcome Measures in Effectiveness Trials (COMET),18 and Core Outcomes in Women’s and Newborn Health (CROWN)19 databases was conducted on January 14, 2021. Full search strategies for Medline and PubMed are available in Supplementary Material 2. The 45 COS listed on the CROWN website were manually screened for eligibility. In the COMET database we used the search function to identify published COS applicable to ages 0–50 to capture all relevant life stages.
Selection process
All articles retrieved from the searches were imported into EndNote and duplicates were removed. One author (E.M. or K.M.) independently screened the remaining papers by title and abstract for inclusion, and then conducted a full text review for methodological reasons for exclusion, as per the eligibility criteria. Studies excluded at full text review are provided, with justifications, in Supplementary Material 3.
Data collection
For each COS, a single reviewer (E.M. or K.M.) extracted the specific condition, its prevalence or incidence, the consensus method used, stakeholders involved, countries involved, the number of core outcomes, and core domains (if applicable). These data are displayed in Table 1.
Synthesis methods
To our knowledge, no systematic review of COS has previously been undertaken, and thus we endeavored to create a process that enabled synthesis across multiple COS. Firstly, we identified an existing taxonomic framework for outcomes by Dodd et al.20 to guide our synthesis process. This framework was chosen as it was designed to be comprehensive, bridge gaps in existing classification systems, and to cover “all potential outcomes from clinical trials”.20 We found no other pre-existing framework to compete with this. Moreover, the authors tested this taxonomy by applying it to COS from the COMET database, and thus it was directly applicable to our intended COS synthesis. This taxonomy outlines five key domains for outcomes: (1) Death, (2) Physiological and Clinical, (3) Life Impact, (4) Adverse Events, and (5) Resource Use.
The synthesis process (undertaken by E.M. and K.M.) began by mapping all core outcomes against all the COS in which they appear. Where we deemed necessary, we collapsed terms referring to the same construct into a single category. For example, “activities of daily living” and “ability to perform normal activities” were termed “activities of daily living”; “spontaneous preterm labor”, “extremely preterm birth <28 weeks”, and “iatrogenic preterm birth” were all labeled “preterm birth”; and core outcomes relating to specific location or features of pain became the overarching construct “pain”.
Once synthesis was completed, we classified each overarching construct under one of the five taxonomic domains. A table displaying the individual core outcomes that were synthesized to produce each overarching construct is available as Supplementary Material 4.
Results
Literature search
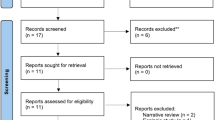
Database searches identified 145 articles in Medline, 160 in PubMed, 25 in CROWN, and 59 in COMET. After removing duplicates, we screened 252 records by title and abstract and excluded a further 174. The remaining 78 studies underwent full-text review for eligibility, and a final 46 COS studies were included in the core outcome mapping. This search strategy is displayed in a PRISMA diagram (see Fig. 1).

From Page et al.15. For more information, visit: http://www.prisma-statement.org/.
Of the included COS, 12 related to conditions of pre-pregnancy, pregnancy, or birth; 5 related to neonates; 15 were relevant to children <8 years old; and 14 addressed conditions affecting adults aged 18–50 years. Table 1 summarizes the characteristics of each COS, including study-specific limitations that could introduce bias.
Outcome synthesis
We identified a total of 414 unique core outcomes from 46 COS. We grouped these outcomes into 118 overarching constructs. We ordered the overarching constructs within the life stages by the total number of COS in which each outcome appeared, as shown in Table 2.
The overarching constructs relating to “quality of life”, “adverse events”, “hospitalization”, “medication/treatment use”, and “death/mortality” were the most common across all four life stages. These constructs align closely with four of the five domains from Dodd’s outcomes taxonomy utilized for our synthesis process, namely Life Impact, Adverse Events, Resource Use, and Death.20 Meanwhile, the constructs in the Physiological and Clinical domain were more varied according to the diseases addressed by the COS relevant to that life stage. We note that COS that were excluded due to very low prevalence (<0.1%) of conditions such as Hirschsprung’s disease21 often contained general (e.g., psychological distress, quality of life) as well as highly specific (e.g., need for a permanent stoma) core outcomes, supporting our belief that even rare conditions would show commonalities in the outcomes valued by stakeholders.
Pregnancy outcomes
In the pregnancy life stage, 34 overarching constructs were drawn from 14 COS (12 pregnancy COS, plus the adult endometriosis and polycystic ovarian syndrome, PCOS, COS). The two most frequently identified constructs were “fetal or neonatal loss” including miscarriage, termination of pregnancy or stillbirth, and “maternal mortality”. Other frequently identified constructs were “preterm birth”, “medication or treatment required”, “hospital or ICU admission”, “live birth”, “mode of delivery”, “adverse effects from intervention”, “pre-eclampsia and its complications”, “gestational diabetes” and “other complications” of pregnancy, labor or the puerperium. In addition to quality of life, mental health was reflected in the constructs of “postnatal depression” and “other mental health”.
Neonatal outcomes
For neonates, 20 overarching constructs were derived from 17 COS, which included pediatric, pregnancy, adult and a dedicated neonatology COS.22 The single most identified construct was “neonatal mortality”. This was followed by “birthweight” including low birthweight, “hospitalization or NICU admission”, and “gestational age at birth”. Other common neonatal constructs, representing the Physiological and Clinical, Adverse Events, and Resource Use domains included “neonatal seizures”, “small for gestational age”, “neurological damage”, “harm from delivery/pregnancy intervention”, “neonatal morbidity”, “neonatal infection/sepsis”, “medical or surgical intervention”, “congenital anomalies”, “respiratory support”, and “neonatal hypoglycemia”.
Pediatric outcomes
For children <8 years old, 40 overarching constructs from 29 COS related both to pregnancy and pediatrics. The most common constructs were “adverse events” following either a condition or treatment and “quality of life”. These were followed by “pain”, “gastrointestinal morbidity”, “hospitalization”, “growth and weight”, “neurodevelopmental morbidity”, “physical function/disability”, “mortality”, “physical health”, and “treatment failure/escalation”. Furthermore, the Life Impact domain was represented by constructs such as “cognitive function/ability”, “breastfeeding” encompassing maternal confidence and duration, “feeding problems/behavior”, “school performance and attendance”, “hearing”, “speech and language”, “mental health and wellbeing”, “sleep quality and duration”, and “social development”. Other seldom-identified constructs that may be notable to life course studies were “quality of family life” and food-related constructs including “types of foods consumed”, “foods offered”, and “eating behaviors and environments”.
Adult outcomes
From the 14 COS addressing adults aged 18–50 (the relevant age range for most parents of young children), we derived 24 overarching constructs. The most consistently identified constructs were “quality of life” (with “psychological health” in a further three COS) “symptoms & disease burden”, and “mortality”. The next tier encompassed “adverse events”, “hospitalization and/or surgery”, and “cardiovascular health/morbidity”. Following this were “neurological function/stroke”, “activities of daily living”, and “general health parameters”, such as body mass index (BMI).
Discussion
Principal findings
From 46 published COS addressing pregnancy, newborns, children <8 years old, and younger adults (aged 18–50 years), we synthesized 118 overarching constructs from 414 unique core outcomes. The prioritized outcomes were typically broad, spanning all aspects of functioning—physical, mental, social, cognitive, participation—with commonalities across multiple COS even when the condition generating an individual COS was rare. The most common overarching constructs across all four life stages were “quality of life”, “adverse events”, “medication use”, “hospitalization“, and “mortality”, which aligned with the taxonomic domains that guided our synthesis. We believe that our synthesis and methodology may be helpful to others in prioritizing outcomes for early life course studies, especially those desiring interventional and strong causal reasoning capabilities.
Strengths
To our knowledge, this systematic approach to synthesizing COS is unique. We collated core outcomes from multiple published COS across the age ranges most relevant to new birth cohorts, and utilized a robust existing taxonomic framework from Dodd et al.20 to guide our classification process. The identified constructs reflect widely prioritized outcomes across life stages most relevant to birth cohorts. Many of these constructs span the spectrum of good and poor health and well-being, are measurable, and could be modifiable with intervention. This emphasizes the importance of life course studies taking a holistic, strength-based approach to outcomes, rather than over-focusing on deficits—anecdotally, a common complaint of participants. We clearly describe our synthesis process so it could be adapted to identify outcomes for other populations (e.g., adolescents, older adults). Beyond identifying outcomes for an individual cohort, the COS synthesis approach could assist life course studies to standardize outcomes with each other and with clinical trials to support harmonized meta-analysis and to triangulate causal inference.
Limitations
Despite the breadth of physical, mental, social, cognitive, and participation outcomes identified, the COS focus on outcomes relevant to trials in the health sector may undervalue or miss entirely some antecedents or outcomes important to observational life course research. For example, while our overarching constructs aligned with Dodd’s taxonomy,20 the latter additionally suggested some outcomes that appear important for consideration in life course studies (e.g., “Economic” and “Societal/Carer Burden” under the Resource Use domain.20) Further, it is not known whether stakeholders would prioritize outcomes differently for life course research than for trials. Some fields are currently more active in COS research than others, including rheumatology,5 nephrology,23 and women’s and newborn health.19 This can result in certain constructs, such as the pediatric construct “gastrointestinal morbidity”, appearing more frequently in the final list of constructs than morbidity in other organ systems; as more COS are completed, we expect this bias to reduce. Despite this bias, it was striking that our highly prioritized outcomes were overwhelmingly not condition-specific, again indicating the universality of the outcomes that children, parents, and services value most regardless of their individual challenges or conditions. A further source of bias is that COS often disproportionately involve stakeholders from English-speaking, high-income countries; while some constructs may therefore be missing, those we identified seem universal in their applicability.
Finally, there are some limitations relating to our methodology. COS typically specify constructs so that, even with this systematic methodology, choices of scales or metrics will still need to be made; however, we posit that harmonizing by construct is the critical first step towards harmonization by measure. As this was a rapid rather than a full systematic review, the methods were rigorous and well-documented, but it was not pre-registered and we did not undertake dual abstract screening or data extraction. Future work could also formalize criteria for synthesizing outcomes and assess their reliability.
Interpretation in the context of life course research
The population-specific overarching constructs we identified are also largely congruent with major morbidities and prominent causal theories for each life stage, which further supports their importance and inclusion in life course studies. For example, a common pregnancy construct was “preterm birth”, which is associated with numerous perinatal, early childhood, and long-term adverse outcomes such as adult hypertension, hyperglycemia, and mental health problems.24 In newborns, the construct of “birthweight” reflects its importance in relation to key non-communicable health outcomes such as cardiovascular disease, diabetes, and obesity, as described by the Developmental Origins of Health and Disease (DOHaD) theory.25 The overarching constructs for young children prioritized their development and participation, regardless of their medical condition(s), through constructs such as “growth and development”, “school attendance/performance”, and “social development”. This is concordant with the work of Sinha et al.26, which identified certain outcomes as particularly important for children, such as quality of life and functional status. Finally, the adult constructs, including “disease burden”, “mental health”, and “cardiovascular health/morbidity”, reflect the impacts of classic life course diseases of ageing. For all of these issues, major gaps remain in understanding of causal pathways and effective interventions, suggesting that these measures synthesized by examining COS are highly relevant to life course cohorts.
Implications
Our approach of COS synthesis offers a transparent method of outcome selection for life course studies and provides a high-level list of constructs for consideration. This approach could help minimize selection bias, taking into account the views of very large numbers of stakeholders (children and families from many walks of life, multiple sectors and disciplines, diverse countries) with a depth and breadth not replicable in any one cohort. It could also help life course studies to better contribute to outcomes research across many fields, fulfilling the “collect once, use multiple times” paradigm. Capturing such outcomes over the long term could greatly extend the value of embedded trials or health services research, for which questions regarding lasting harms and benefits are typically out of reach due to short trial funding windows. This approach would also enable large multi-use life course cohorts to have an increased focus on causation and solutions than is typically possible through observational research alone.
We propose that life course studies could incorporate these highly prioritized domains and constructs into their process for selecting measures, supplementing it with other approaches to address the gaps in the current COS literature and ensure comprehensive and robust measurement. For example, GenV is also drawing from its life course frameworks1 and consulting with stakeholders via methods including focus groups, an open focus area survey27 and group prioritization activities with researchers.28 Once a study has developed their outcome constructs, a standardized and reproducible measure must be identified for each. Given the generalizability-by-design of COS, we believe that this approach will allow life course studies like GenV to harmonize not only with other life course cohorts but with trials, registries, and health services research internationally.
Future research
Future life course studies might choose to use these findings, update this study with new COS, or reproduce its methodology for older children, adolescents, and/or ageing adults. Doing so would increase confidence that the most important constructs for different life stages are captured and that the cohort will support wide-ranging interventional as well as observational research. Future research could further explore outcome classification frameworks such as that by Dodd et al.20 and also focus on developing population health COS to capture important outcomes relevant to the wider community, including outcomes (e.g., economic, carer burden) that are under-represented in COS but important to life course studies. Identifying such gaps could motivate the creation of COS in additional research areas, or prompt researchers to identify methods to supplement the COS synthesis approach for outcome selection. Finally, ongoing efforts by regulators, funders, researchers, and journals are required to disseminate and utilize COS and ensure that agreed-upon stakeholder-driven outcomes are considered in all studies.
Conclusion
This COS synthesis generated a breadth of constructs relevant to birth cohort outcomes selection. Some constructs appeared in multiple COS spanning all four life stages examined (such as quality of life, hospitalization), while others appeared in multiple COS for individual life stages (such as pre-eclampsia, birthweight, social development, cardiovascular health/morbidity). The rigor and in-built stakeholder and trials perspectives of a COS-shaped outcomes selection approach could help position future cohorts to include life course interventions and stronger causal inferencing. This review’s synthesized COS data are guiding outcome measures selection for the early years of a large new birth and parent cohort (GenV) and appear relevant to longitudinal population studies more generally.
References
Wang, J., Hu, Y. J., Clifford, S. A. & Wake, M. Selecting life course frameworks to guide and communicate large new cohort studies: Generation Victoria (GenV) case study. J. Dev. Orig. Health Dis. 1–20, https://doi.org/10.1017/S2040174420001245 (2021).
Tomlinson, M., Fearon, P., Christodoulou, J. & Rotheram-Borus, M. J. Editorial perspective: stop describing and start fixing—the promise of longitudinal intervention cohorts. J. Child Psychol. Psychiatry 61, 1388–1390 (2020).
Webbe, J., Sinha, I. & Gale, C. Core outcome sets. Arch. Dis. Child Educ. Pract. Ed. 103, 163–166 (2017).
Kirkham, J. J. et al. Core outcome set-STAndards for development: The COS-STAD recommendations. PLoS Med. 14, e1002447 (2017).
Beaton, D. et al. Chapter 4 - Developing Core Domain Sets. The OMERACT Handbook. OMERACT. Version 2.1 (2021). https://omeracthandbook.org/handbook.
Lopez-Olivo, M. A. et al. Core outcome sets specifically for longterm observational studies: Omeract special interest group update in rheumatoid arthritis. J. Rheumatol. 46, 1164–1167 (2019).
Dickerson, J. et al. Born in Bradford’s better start: an experimental birth cohort study to evaluate the impact of early life interventions. BMC Public Health 15, 711 (2016).
Silva, D. T. et al. Introducing the ORIGINS project: a community-based interventional birth cohort. Rev. Environ. Health 35, 281–293 (2020).
2018–2020 Australian Population.com. Victoria—Australian Population 2021 (accessed 10 Sep. 2021). https://www.australian-population.com/states/victoria-population/.
Wake, M. et al. Integrating trials into a whole-population cohort of children and parents: statement of intent (trials) for the Generation Victoria (GenV) cohort. BMC Med. Res. Methodol. 20, 238 (2020).
Murdoch Children’s Research Institute (MCRI). Generation Victoria (accessed 3 Feb. 2021). https://mcri.figshare.com/projects/Generation_Victoria/35822.
Clifford, S. & Wake, M. GenV measures selection principles. Generation Victoria Working Paper 2020–21. https://doi.org/10.25374/MCRI.9750983 (2020).
Wake, M., Gasparini, L., Hourani, D. & Siero, W. The Victorian Child’s Lifecourse journey in data (Murdoch Children’s Research Institute. Journal contribution, accessed 22 Feb. 2021). https://doi.org/10.25374/MCRI.6741941.v3 (2018).
Davey Smith, G. Post-modern epidemiology: when methods meet matter. Am. J. Epidemiol. 188, 1410–1419 (2019).
Page, M. J. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, https://doi.org/10.1136/bmj.n71 (2021).
Lee, A., Davies, A. & Young, A. E. Systematic review of international Delphi surveys for core outcome set development: representation of international patients. BMJ Open 10, e040223 (2020).
Jones, J. & Hunter, D. Consensus methods for medical and health services research. BMJ 311, 376–380 (1995).
The COMET Initiative (accessed 14 Jan. 2021). http://www.comet-initiative.org/.
The CROWN Initiative (accessed 14 Jan. 2021). http://www.crown-initiative.org/.
Dodd, S. et al. A taxonomy has been developed for outcomes in medical research to help improve knowledge discovery. J. Clin. Epidemiol. 96, 84–92 (2018).
Allin, B. S. R. et al. NETS 1HD study: development of a Hirschsprung’s disease core outcome set. Arch. Dis. Child. 102, 1143–1151 (2017).
Webbe, J. W. H. et al. Core outcomes in neonatology: development of a core outcome set for neonatal research. Arch. Dis. Child Fetal Neonatal Ed. 105, 425–431 (2020).
The SONG Initiative (accessed 13 Oct. 2020). https://songinitiative.org/.
Duffy, J. et al. A core outcome set for pre-eclampsia research: an international consensus development study. BJOG 127, 1516–1526 (2020).
Eriksson, J. G. Developmental Origins of Health and Disease—from a small body size at birth to epigenetics. Ann. Med. 48, 456–467 (2016).
Sinha, I. P. et al. Standard 5: Selection, measurement, and reporting of outcomes in clinical trials in children. Pediatrics 129(Suppl 3), S146–S152 (2012).
Davenport, L. et al. GenV focus area survey final report. Generation Victoria Working Paper 2020–21. https://doi.org/10.25374/MCRI.13003985.v4 (2020).
Davies, S., Davenport, L., Lamb, K. & Wake, M. Developing GenV’s research methodologies: brainstorming sessions and survey 2018. Generation Victoria Working Paper 2020-03. https://doi.org/10.25374/MCRI.8234006 (2020).
Al Wattar, B. H. et al. Development of a core outcome set for epilepsy in pregnancy (E-CORE): a national multi-stakeholder modified Delphi consensus study. BJOG 124, 661–667 (2017).
Wang, J. Conditions & traits—prevalence (P), incidence (I), distribution (D) by GenV Focus Areas. In correspondence with Musgrove, E. GenV internal documents (2020).
Dos Santos, F. et al. Development of a core outcome set for trials on induction of labour: an international multistakeholder Delphi study. BJOG 125, 1673–1680 (2018).
Egan, A. M. et al. A core outcome set for studies of gestational diabetes mellitus prevention and treatment. Diabetologia 63, 1120–1127 (2020).
Australian Institute of Health and Welfare. Gestational Diabetes (accessed 1 March 2021). https://www.aihw.gov.au/reports/diabetes/diabetes/contents/how-many-australians-have-diabetes/gestational-diabetes.
Egan, A. M. et al. A core outcome set for studies evaluating the effectiveness of prepregnancy care for women with pregestational diabetes. Diabetologia 60, 1190–1196 (2017).
Healy, P. et al. A Core Outcome Set for the prevention and treatment of fetal GROwth restriction: deVeloping Endpoints: The COSGROVE study. Am. J. Obstet. Gynecol. 221, 339 e331–339 e310 (2019).
Malhotra, A. et al. Neonatal morbidities of fetal growth restriction: pathophysiology and impact. Front. Endocrinol. 10, 55 (2019).
Jansen, L. et al. A core outcome set for hyperemesis gravidarum research: an international consensus study. BJOG 127, 983–992 (2020).
Meher, S. et al. Core outcome sets for prevention and treatment of postpartum haemorrhage: an International Delphi Consensus Study. BJOG 126, 83–93 (2019).
Duffy, J. M. N. et al. Developing a core outcome set for future infertility research: an international consensus development study. Hum. Reprod. 35, 2725–2734 (2020).
Australian Government Department of Health. Infertility (accessed 14 Feb. 2021). https://www.healthdirect.gov.au/infertility.
Wu, N., O’Reilly, S., Nielsen, K. K., Maindal, H. T. & Dasgupta, K. Core outcome set for diabetes after pregnancy prevention across the life span: International Delphi study. BMJ Open Diabetes Res. Care 8, e001594 (2020).
Townsend, R. et al. Core outcome set for studies investigating management of selective fetal growth restriction in twins. Ultrasound Obstet. Gynecol. 55, 652–660 (2020).
Cordero, L., Franco, A., Joy, S. D. & O’Shaughnessy, R. W. Monochorionic diamniotic infants without twin-to-twin transfusion syndrome. J. Perinatol. 25, 753–758 (2005).
van ʼt Hooft, J. et al. A core outcome set for evaluation of interventions to prevent preterm birth. Obstet. Gynecol. 127, 49–58 (2016).
Kelly, L. E. et al. A core outcome set for neonatal opioid withdrawal syndrome. Pediatrics 146, 07 (2020).
Singendonk, M. M. J. et al. Development of a core outcome set for infant gastroesophageal reflux disease. J. Pediatr. Gastroenterol. Nutr. 68, 655–661 (2018).
Leung, A. K. & Hon, K. L. Gastroesophageal reflux in children: an updated review. Drugs Context 8, 212591 (2019).
Crudgington, H. et al. Core Health Outcomes in Childhood Epilepsy (CHOICE): development of a core outcome set using systematic review methods and a Delphi survey consensus. Epilepsia 60, 857–871 (2019).
Steutel, N. F. et al. Developing a core outcome set for infant colic for primary, secondary and tertiary care settings: a prospective study. BMJ Open 7, e015418 (2017).
Damhuis, S. E. et al. A Core Outcome Set and minimum reporting set for intervention studies in growth restriction in the NEwbOrN: The COSNEON study. Pediatr. Res. https://doi.org/10.1038/s41390-020-01119-5 (2020).
Harman, N. L. et al. The importance of integration of stakeholder views in core outcome set development: Otitis media with effusion in children with cleft palate. PLoS ONE 10, e0129514 (2015).
Gilchrist, F. J. et al. Developing a core outcome set for children with protracted bacterial bronchitis. ERJ Open Res. 6, 00344–02019 (2020).
Laird, P., Totterdell, J., Walker, R., Chang, A. B. & Schultz, A. Prevalence of chronic wet cough and protracted bacterial bronchitis in Aboriginal children. ERJ Open Res. 5, 00248–02019 (2019).
Horbach, S. E. R. et al. Development of an international core outcome set for peripheral vascular malformations: The OVAMA project. Br. J. Dermatol. 178, 473–481 (2018).
Cahill, A. M. & Nijs, E. L. Pediatric vascular malformations: Pathophysiology, diagnosis, and the role of interventional radiology. Cardiovasc. Interv. Radiol. 34, 691–704 (2011).
Karas, J. et al. A core outcome set for clinical trials in acute diarrhoea. Arch. Dis. Child 100, 359–363 (2015).
Webb, A. & Starr, M. Acute gastroenteritis in children. Aust. Fam. Physician (RACGP) 34, 227–231 (2005).
Kuizenga-Wessel, S. et al. Development of a core outcome set for clinical trials in childhood constipation: a study using a Delphi technique. BMJ Paediatr. Open 1, e000017 (2017).
Liu, P. Z. et al. A core outcome set for research on the management of otitis media with effusion in otherwise-healthy children. Int J. Pediatr. Otorhinolaryngol. 134, 110029 (2020).
Matvienko-Sikar, K. et al. A core outcome set for trials of infant-feeding interventions to prevent childhood obesity. Int. J. Obes. 44, 2035–2043 (2020).
Morgan, E. M. et al. Establishing an updated core domain set for studies in juvenile idiopathic arthritis: a report from the OMERACT 2018 JIA workshop. J. Rheumatol. 46, 1006–1013 (2019).
Murugupillai, R., Ranganathan, S. S., Wanigasinghe, J., Muniyandi, R. & Arambepola, C. Development of outcome criteria to measure effectiveness of antiepileptic therapy in children. Epilepsy Behav. 80, 56–60 (2018).
Sherratt, F. C. et al. Core outcome set for uncomplicated acute appendicitis in children and young people. Br. J. Surg. 107, 1013–1022 (2020).
Schneuer, F. J. et al. A population-based comparison of the post-operative outcomes of open and laparoscopic appendicectomy in children. Med J. Aust. 209, 80–85 (2018).
Zeevenhooven, J. et al. A core outcome set for clinical trials in pediatric functional abdominal pain disorders. J. Pediatr. 221, 115–122.e115 (2020).
Fink, E. L. et al. A core outcome set for pediatric critical care. Crit. Care Med. 48, 1819–1828 (2020).
Ibiebele, I., Algert, C. S., Bowen, J. R. & Roberts, C. L. Pediatric admissions that include intensive care: a population-based study. BMC Health Serv. Res. 18, 264 (2018).
Sinha, I. P., Gallagher, R., Williamson, P. R. & Smyth, R. L. Development of a core outcome set for clinical trials in childhood asthma: a survey of clinicians, parents, and young people. Trials 13, 103 (2012).
Topjian, A. A. et al. P-COSCA (Pediatric Core Outcome Set for Cardiac Arrest) in children: an advisory statement from the international liaison committee on resuscitation. Circulation 142, e246–e261 (2020).
Al Wattar, B. H. et al. Harmonising research outcomes for polycystic ovary syndrome: an international multi-stakeholder core outcome set. Hum. Reprod. 35, 404–412 (2020).
Benstoem, C. et al. A core outcome set for adult cardiac surgery trials: a consensus study. PLoS ONE 12, e0186772 (2017).
Shi, W. Y., Oldfield, Z., Tam, R., Cochrane, A. D. & Smith, J. A. Cardiothoracic surgery training in Australia and New Zealand. J. Thorac. Cardiovasc. Surg. 156, 718–725 (2018).
Byrne, M. et al. A core outcomes set for clinical trials of interventions for young adults with type 1 diabetes: An international, multi-perspective Delphi consensus study. Trials 18, 602 (2017).
Evangelidis, N. et al. Developing a set of core outcomes for trials in hemodialysis: an international Delphi survey. Am. J. Kidney Dis. 70, 464–475 (2017).
Australian Institute of Health and Welfare. Chronic Kidney Disease. in Australia’s Health 2018, Ch. 3.9 (accessed 13 Oct. 2020). https://www.aihw.gov.au/getmedia/eed56699-8b66-4c0a-8d12-743a5fd8cbf1/aihw-aus-221-chapter-3-9.pdf.aspx.
Harman, N. L. et al. Selecting Core Outcomes for Randomised Effectiveness trials In Type 2 diabetes (SCORE-IT): a patient and healthcare professional consensus on a core outcome set for type 2 diabetes. BMJ Open Diabetes Res. Care 7, e000700 (2019).
Haywood, K. et al. COSCA (Core Outcome Set for Cardiac Arrest) in adults: an advisory statement from the international liaison committee on resuscitation. Resuscitation 127, 147–163 (2018).
NSW Health. Cardiac Arrest and Defibrillators: A Guide for Consumers (accessed 13 Oct, 2020). https://www.health.nsw.gov.au/cardiacarrest/Pages/consumers.aspx.
Hopkins, C. et al. CHronic Rhinosinusitis Outcome MEasures (CHROME), developing a core outcome set for trials of interventions in chronic rhinosinusitis. Rhinology 56, 22–32 (2018).
O’Lone, E. et al. Identifying critically important cardiovascular outcomes for trials in hemodialysis: an international survey with patients, caregivers and health professionals. Nephrol. Dial. Transpl. 35, 1761–1769 (2020).
Ramiro, S. et al. The OMERACT core domain set for clinical trials of shoulder disorders. J. Rheumatol. 46, 969–975 (2019).
Tong, A. et al. Core outcomes set for trials in people with coronavirus disease 2019. Crit. Care Med. 48, 1622–1635 (2020).
Tyler, N., Wright, N., Grundy, A. & Waring, J. Developing a core outcome set for interventions to improve discharge from mental health inpatient services: a survey, Delphi and consensus meeting with key stakeholder groups. BMJ Open 10, e034215 (2020).
Australian Institute of Health and Welfare. Mental health services in Australia: in brief 2019 (accessed 13 Oct. 2020). https://doi.org/10.25816/5ec5bac5ed175.
Retzer, A. et al. Development of a core outcome set for use in community-based bipolar trials-a qualitative study and modified delphi. PLoS ONE 15, e0240518 (2020).
Viecelli, A. K. et al. Identifying critically important vascular access outcomes for trials in haemodialysis: An international survey with patients, caregivers and health professionals. Nephrol. Dial. Transpl. 35, 657–668 (2020).
Duffy, J. et al. A core outcome set for future endometriosis research: an international consensus development study. BJOG 127, 967–974 (2020).
Parasar, P., Ozcan, P. & Terry, K. L. Endometriosis: epidemiology, diagnosis and clinical management. Curr. Obstet. Gynecol. Rep. 6, 34–41 (2017).
Acknowledgements
We would like to thank Dr. Jing Wang and Ms. Poh Chua for their generous support of and contribution to this review.
Funding
No specific funding was available for this study. Generation Victoria is supported by the Paul Ramsay Foundation, Victorian Government, Murdoch Children’s Research Institute (MCRI), and The Royal Children’s Hospital Foundation. Research at the MCRI is supported by the Victorian Government’s Operational Infrastructure Support Program. M.W. is supported by Australian National Health & Medical Research Council (NHMRC) Principal Research Fellowship 1160906. H.T. is supported by an NHMRC Practitioner Fellowship funded by the Australian Medical Research Future Fund. S.A. Carter is supported by NHMRC Post-graduate Scholarship 1168994.
Author information
Authors and Affiliations
Contributions
E.M., L.G., K.M., S.A. Clifford, S.A. Carter, and M.W. contributed to conception and design, acquisition of data, and/or analysis and interpretation of data; E.M., L.G., S.A. Clifford, and M.W. drafted the manuscript; all authors revised the manuscript critically for important intellectual content and approved the final version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent statement
Patient consent was not required for this study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Musgrove, E., Gasparini, L., McBain, K. et al. Synthesizing Core Outcome Sets for outcomes research in cohort studies: a systematic review. Pediatr Res 92, 936–945 (2022). https://doi.org/10.1038/s41390-021-01801-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-021-01801-2
