
Abstract
Background
Premature adrenarche is a condition of childhood adrenal androgen excess (AAE) in the absence of gonadotropin-dependent puberty, and has been linked to insulin resistance and progression to metabolic syndrome. Microbial dysbiosis is associated with progression of inflammatory states and chronic diseases. Here, we aimed to examine the salivary microbiomes of children with AAE and assess the relationship with adrenal androgens and metabolic parameters.
Methods
In a prospective cross-sectional study of children with AAE and healthy controls, adrenal and metabolic parameters were characterized and salivary microbiome was profiled using V3–V4 16S rDNA gene amplicon sequencing.
Results
There was increased α-diversity in AAE (5 M, 15 F) compared to controls (3 M, 8 F), with positive correlation of 11OHA4, 11KA4, testosterone, androstenedione, DHEA, and DHEAS. Subanalyses showed increased α-diversity in both overweight/obese AAE and normal weight AAE compared to normal weight controls. Genus Peptostreptococcus, Veillonella, and Streptococcus salivarius were increased in normal weight AAE. Genus Prevotella, Abiotrophia, and Neisseria were increased in overweight/obese AAE.
Conclusion
These pilot data demonstrate differences in salivary microbiome profiles of children with and without AAE. Further studies are needed to assess the causal relationships between adrenal androgens, metabolic dysfunction, and salivary microbiome composition.
Impact
-
This study is the first to report the salivary microbiome of prepubertal children with adrenal androgen excess (AAE).
-
α-Diversity is increased in the salivary microbiome of children with AAE independent of weight status, and in this study cohort several serum androgens are positively associated with α-diversity.
-
Several taxa that have been associated with periodontal disease and inflammation are found to be significantly increased in AAE.
Similar content being viewed by others


Introduction
Premature adrenarche (PA) is the early maturation of the adrenal zona reticularis and rise of 19-carbon steroids, predominantly dehydroepiandrosterone (DHEA) and DHEA sulfate (DHEAS). It is the most common cause of premature pubarche (PP), the early onset of pubic and/or axillary hair before the age of 8 years in girls and 9 years in boys1. PA is a diagnosis of exclusion, and can be made after ruling out other causes of hyperandrogenism such as congenital adrenal hyperplasia, androgen-secreting tumors, and exogenous androgen exposure. Laboratory data usually reflect increased levels of DHEA, DHEAS, and androstenedione; recent studies have correlated 11-oxygenated 19-carbon steroids (11-oxygenated androgens [11oAs]) with the clinical signs of pubarche independent of adrenarche2,3,4. PA has been associated with obesity, metabolic syndrome, and polycystic ovary syndrome (PCOS), and may represent an early hyperandrogenic state in girls who later present with PCOS, with hyperinsulinism playing a key role5,6,7,8,9.
The human gut microbiome is closely linked to the host’s physiology and metabolism, and can contribute to metabolic disease states including obesity, insulin resistance, diabetes, and PCOS10,11,12,13,14,15. There is a bidirectional relationship between steroid hormones and gut microbial communities16,17, with studies showing that prenatal and neonatal exposure to androgens can lead to gut dysbiosis in rats18,19,20. Several studies have shown that women with PCOS show taxonomical differences in their gut microbiomes and further signs of dysbiosis, including a reduced α-diversity that negatively correlates with serum testosterone levels in both healthy and obese PCOS subjects21,22,23,24. Imbalances in the gut microbiome can lead to the compromise of intestinal epithelial cell connections and a “leaky” gut, increasing the permeability of the gut lining to inflammatory mediators such as lipopolysaccharides. This inflammation can subsequently induce a state of insulin resistance and hyperinsulinemia, which has been shown to play a role in the etiology of hyperandrogenic states like PCOS25,26,27.
Associations between salivary microbiome dysbiosis, systemic inflammation, and metabolic disease states have been described. These relationships may also have predictive value in the diagnosis of systemic disease early in childhood28,29. Studies have demonstrated unique salivary microbiome signatures in subjects (including children and adolescents) with obesity30,31, nonalcoholic fatty liver disease32, type 2 diabetes33, and PCOS34,35.
To our knowledge, there are currently no studies on the microbiome of children with adrenal androgen excess (AAE), including PA or PP. The collection of a salivary sample is a convenient, noninvasive way to evaluate microbial dysbiosis in pediatric populations, with virtually no discomfort to the patient36. As children with PA are at elevated risk for progression to metabolic syndrome and related diseases such as PCOS, the study of their microbiomes may reveal early signs of aberrant dysbiosis, and may provide insight into the connections between PA and metabolic disease states. The aims of this study were to describe the salivary microbiome in children with AAE (PA or PP), and to investigate the potential of specific taxa and measures of bacterial diversity to distinguish between children with AAE and controls. Additionally, we sought to determine if features of childhood AAE (elevated adrenal androgens including 11oAs) and common co-occurring features (elevated body mass index (BMI) and signs of insulin resistance and metabolic syndrome) are correlated with microbial dysbiosis in children with AAE compared to healthy controls.
Methods
Study subjects
This was a cross-sectional prospective cohort study of children (cases and controls) at a tertiary university hospital medical center. Approval was obtained from the Institutional Review Board at Columbia University Irving Medical Center (CUIMC). Prepubertal children aged 3–8 (girls) and 3–9 years (boys) were recruited from the pediatric endocrinology practices of CUIMC, affiliated general pediatric practices, and in response to community flyers and the CUIMC RecruitMe website. Among the subjects recruited, inclusion criteria for the case group were clinical signs of adrenarche, including axillary odor, axillary hair, and/or pubic hair, in the absence of true puberty (Tanner I breast in girls and testicular volume ≤3 mL in boys); the remaining children were in the control group. Exclusion criteria were a history of chronic illness or other known endocrinopathies, evidence of adrenal enzyme defect, elevated inflammatory marker (C-reactive protein), history of hormone exposure, chronic glucocorticoid use, psychostimulant use, use of antibiotics in the prior 3 months, or use of probiotics in the last 1 month. The case group was previously subdivided into PA and PP subgroups based on elevation of adrenal androgen serum DHEAS in a prior study;4 however, as described in our publication, there did not appear to be any significant anthropometric or biochemical differences in this population (notably in 11oAs). Therefore, the PA and PP subgroups were treated as one case cohort (referred to in this study as the AAE group) for analysis of salivary microbiome measures.
Study visit and measurements
After obtaining appropriate parental consent and subject assent (7 years of age and older), subjects underwent a 1-day early morning study visit at the Clinical Research Resource at Columbia Irving Institute for Clinical and Translational Research (UL1TR001873) after an overnight fast of at least 8 h (only water prior to saliva sampling). A complete medical history was obtained using a standardized history template, in the language each participant/parent preferred (English or Spanish). A complete physical examination by a pediatric endocrinologist was performed including Tanner staging of puberty and measurements of blood pressure, height, weight, and waist circumference. The subject was asked to chew a paraffin tablet (Orion Diagnostica) until sufficient accumulation of saliva in the oral cavity, and then spit into a 50 mL sterile DNA-free conical tube (Falcon) repeatedly until 5 mL of saliva was collected. Saliva samples were immediately cooled on ice and within 30 min were frozen at −80 °C until analysis. Fasting blood samples were obtained, centrifuged for 20 min at 3000 r.p.m., and frozen at −80 °C until analysis.
Gestational size was calculated using the PediTools Electronic Growth Chart Calculator;37 small for gestational age status was defined as birth weight less than 10th percentile for gestational age. BMI was calculated from the weight and height measurements. Subjects were classified as underweight (<5th percentile), normal weight (5th to <85th percentile), overweight (85th to <95th percentile), and obese (≥95th percentile), using cut-off criteria based on the sex-specific 2000 Centers for Disease Control and Prevention (CDC) BMI-for-age growth curves. In light of unique salivary microbiome signatures reported in prior studies30,31, the study cohort was subdivided into four groups for microbiome subanalyses: cases and controls with BMI < 85th percentile (“normal weight AAE” and “normal weight controls”) and with BMI ≥ 85th percentile (“overweight/obese AAE” and “overweight/obese controls”). Height age was defined as the age at which the measured height plots at the 50th percentile on the CDC stature-for-age sex-specific growth curves. Age-, sex-, and height-specific blood pressure percentiles and z-scores were determined using a pediatric blood pressure reference chart (Children’s Nutrition Research Center, Baylor College of Medicine, Houston, TX)38. Age- and sex-specific waist circumference percentiles were determined using data from the Third National Health and Nutrition Examination Survey (NHANES III)39.
Laboratory analysis
The following serum analytes were evaluated in the Biomarkers Core Laboratory of the Irving Institute for Clinical and Translational Research (Columbia University, New York, NY): insulin-like growth factor 1 (IGF-1), insulin (Immulite 1000, Siemens), blood glucose, hemoglobin A1c (HbA1c), total cholesterol, triglycerides, high-density lipoprotein cholesterol (HDL-C), and high-sensitivity C-reactive protein (Cobas Integra 400, Roche Diagnostics). Adrenal androgens including DHEA, DHEAS, androstenedione, and total testosterone were assessed by commercial laboratory (Esoterix, Inc., Calabasas Hills, CA) by high-performance liquid chromatography/tandem mass spectrometry (LC-MS/MS). Sera for 11oAs including 11β-hydroxyandrostenedione (11OHA4), 11β-hydroxytestosterone (11OHT), 11-ketoandrostenedione (11KA4), and 11-ketotestosterone (11KT) were analyzed by LC-MS/MS as previously described by Wright et al.40 (University of Michigan, Ann Arbor, MI). The lower limit of quantification (LLOQ), defined as the minimum concentration achieving an extrapolated signal-to-noise ratio of 3, ranged from 3 ng/dL (0.1 nmol/L) (11OHT, 11KA4, 11KT) to 10 ng/dL (0.3 nmol/L) (11OHA4). Intra-assay coefficients of variability for the 11oAs were all less than 12%. Laboratory values that were below the LLOQ for the assay were recorded as the LLOQ cut-off value for the respective assay.
Low-density lipoprotein cholesterol (LDL-C) was calculated from total cholesterol, HDL-C, and triglycerides using the Friedewald formula. Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated using the formula (fasting glucose [mmol/L] × fasting insulin [mU/L]/22.5). Subjects were classified as having childhood metabolic syndrome using de Ferranti et al.41 definition of three or more of the following criteria: waist circumference >75th percentile for age and sex, fasting blood glucose ≥110 mg/dL (≥6.1 mmol/L), triglycerides ≥100 mg/dL (≥1.3 mmol/L), HDL-C ≤ 40 mg/dL (1.03 mmol/L), and blood pressure ≥90th percentile for age, sex, and height.
Microbiome analysis
DNA isolation and sequencing
DNA was extracted using the Qiagen MagAttract PowerSoil DNA kit (Qiagen, Hilden, Germany). Samples were homogenized with garnet beads in 750 µl of Powerbead solution by bead-beating and further extracted on an Eppendorf epMotion 5705 automated system (Eppendorf, Hamburg, Germany) for extraction following the manufacturer’s protocol. Extracted DNA was stored in elution buffer at −20 °C.
16S rRNA gene amplification for detection of the bacterial 16S rRNA gene, PCR amplification of the V3–V4 region was performed using gene‐specific sequences with Illumina adapter overhang nucleotide sequences. Libraries were multiplexed by using Illumina Nextera XT Index kits; the calculated equimolar pools were sequenced on the Illumina MiSeq platform using paired-end 300 cycle MiSeq Reagent Kit V3 (Illumina).
16S rRNA microbiome analysis
16S rRNA sequences were processed and applied using the DADA2 pipeline42 and R v3.3.0. Taxonomic classification was performed using a Naïve Bayes classifier trained using the GreenGenes 97% clustered sequences (version 13.8), downloaded from https://benjjneb.github.io/dada2/training.html 43. The table was imported into R v3.6.1 to analyze for α-diversity (Shannon, Chao) and β-diversity (UniFrac), and analyses were performed using a function of the phyloseq v1.28.0 package44. Based on α-diversity rarefaction, we applied a minimum cut-off of 10,000 read counts for inclusion in the analysis.
Univariate linear regression models (lm in R) of α-diversity were used for testing with clinical and laboratory measurements. Case status (AAE or control) was applied for this analysis as well. β-Diversity was analyzed using permutational multivariate analysis of variance (PERMANOVA): a non-parametric method to conduct multivariate ANOVA and determine if the centroids of sample clusters differ. The test statistic is calculated from the comparison of dissimilarities among inter-class objects to those among intra-class objects. Differential abundance testing of bacterial amplicon sequence variant (ASV)s between groups was also performed using DESeq2 (ref. 45).
Remaining statistical calculations were conducted using SAS software (version 9.4, Cary, NC, USA) to compare case and control groups: non-parametric Mann–Whitney U test for continuous data and Fischer’s exact test for categorical data. A stepdown bootstrap with replacement adjustment was used for multiple comparisons of between-group differences for variables of interest within laboratory metabolic data and steroid data46. A P value of <0.05 was considered statistically significant.
Results
Description of cohort
Over a 21-month period, 32 participants were enrolled into the study and completed screening with exam and laboratory work; one of these participants was subsequently excluded from analysis due to an abnormally elevated C-reactive protein laboratory value. Baseline characteristics and laboratory data were collected for 20 children with AAE (5 M, 15 F) and 11 healthy controls (3 M, 8 F) (Table 1). While children with AAE were older than controls (P = 0.016) and had greater height age (P = 0.002), there was no difference in height age to chronological age (HA/CA) ratio, and all children were confirmed on physical exam to be prepubertal. Preterm gestations were higher in AAE (7/20) compared to controls (0/11) (P = 0.033), but there was no difference in small for gestational age status between groups (0/20 cases and 2/11 controls; P = 0.120). There were no other significant differences between groups for sex, BMI, birth history, or other demographic or clinical data (Table 1). Criteria for childhood metabolic syndrome were met in three cases (15%) and one control (9%).
Both serum insulin and HOMA-IR were elevated in the AAE cohort compared to controls, though these differences were not statistically significant after adjustment of metabolic data for multiple comparisons (Table 1). Serum blood glucose, HbA1c, HDL-C, triglycerides, cholesterol, LDL-C, and C-reactive protein were similar between groups.
Serum concentrations of testosterone and androstenedione were higher in subjects with AAE, though the laboratory value differences were not clinically significant and in the expected range for the subjects’ Tanner stage for pubic hair. Serum levels of IGF-1 (P = 0.001), DHEA (P = 0.002), and DHEAS (P < 0.001) were elevated in AAE compared to controls, and serum 11oAs were significantly higher in subjects with AAE including 11OHT (P = 0.001), 11KT, 11OHA4, and 11KA4 (P < 0.001).
Microbiome data
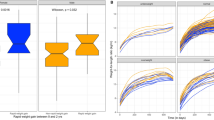
We then aimed to compare differences in saliva microbiota between AAE and controls. Compared to controls, the participants with AAE had significantly higher α-diversity as measured by richness (P = 0.021, Chao1) and richness and evenness (P = 0.0072, Shannon) (Fig. 1). Increased α-diversity was observed in overweight/obese AAE (P = 0.088, Chao1; P = 0.05, Shannon) and normal weight AAE (P = 0.015, Chao1; P = 0.0069, Shannon) compared to normal weight controls. α-Diversity was increased in preterm compared to term gestations (P = 0.032, Chao1; P = 0.048, Shannon). There were no differences in α-diversity observed for age, sex, race, ethnicity, children meeting criteria for childhood metabolic syndrome, or children with acanthosis nigricans on exam.

α-Diversity in AAE and controls by a Chao1 estimator and b Shannon index. c Principal coordinates analysis (PCoA) shows β-diversity based on the UniFrac distance metrics in AAE.
In univariate regression analysis, several serum analytes were positively associated with α-diversity: 11OHA4, 11KA4, testosterone, androstenedione (Chao1), DHEA, and DHEAS (Chao1, Shannon) (Table 2). Markers of metabolic dysfunction (glucose, insulin, HOMA-IR) were not found to have statistically significant association with α-diversity.
We then compared microbial community composition using β-diversity. There were no differences in clustering of UniFrac distance matrices for β-diversity between AAE and control groups (Fig. 1). To further determine if groups had differential abundance of ASVs, we performed differential abundance testing with DESeq2. There were no significant differentially abundant taxa between AAE and control groups. However, in subgroup analyses for normal weight and overweight/obese AAE and control groups, we found multiple differentially abundant taxa that were increased (Fig. 2). This included increased genus Peptostreptococcus, Veillonella, and Streptococcus salivarius in the normal weight AAE group compared to normal weight controls. Prevotella nanceiensis, genus Abiotrophia, and Neisseria were increased in normal weight controls compared to overweight/obese controls. These taxa were also increased in the overweight/obese AAE group compared to overweight/obese controls.

Comparisons are shown between (a) normal weight control and normal weight AAE, (b) normal weight control and overweight/obese AAE, (c) normal weight control and overweight/obese control, and (d) overweight/obese control and overweight/obese AAE in differential abundance of ASV. ASV in blue indicate increased abundance in the control group, whereas ASV in red show increased ASV in the respective case groups. The depicted taxa had a minimum differential abundance magnitude of change (fold change) > 0 with a P value of <0.05.
Taken together, these findings suggest that alterations in bacterial diversity may be mediated in part by elevated adrenal androgens, and this may be independent of other metabolic health factors associated with AAE. However, subanalyses suggest overweight/obese status may influence the differential abundance of taxa observed.
Discussion
To our knowledge, this is the first study to describe the salivary microbiome in children with AAE (either PA or PP). We found that our participants with AAE had a significantly higher α-diversity as measured by richness and evenness. Additionally, there was increased α-diversity in overweight/obese AAE and normal weight AAE compared to normal weight controls, suggesting that this increase in α-diversity relates to AAE, not weight, status. This result affirms the knowledge that oral and gut communities are quite distinct: decreased α-diversity is observed in studies of the gut microbiome in metabolic disease, including obesity47,48 and PCOS16,22. Previous studies of the salivary microbiome in children demonstrate increased bacterial diversity in obesity; a recent study by Mameli et al. reported increased α-diversity in the salivary microbiome of obese children and adolescents30, and another pediatric study found that α-diversity tended to be higher in obese children as compared to children with type 2 diabetes and controls—although not significantly so33. Future studies in larger cohorts are needed to investigate the potential relationship between early androgen excess and salivary microbial diversity.
In addition, our study showed that several androgens, including 11OHA4, 11KA4, testosterone, androstenedione, DHEA, and DHEAS, were positively associated with salivary microbiome α-diversity as measured by richness and evenness. This finding suggests that correlations between androgen levels and salivary dysbiosis exist. In contrast, a pilot study by Lindheim et al.34 assessed the salivary microbiome profile of women with PCOS and showed no significant difference in α-diversity between cases and controls. In this study population, the authors described that the study cohort had, on average, a mild PCOS diagnosis; this study should not rule out the possibility that more severe hyperandrogenic states may associate with significant differences in salivary microbial diversity.
A possible confounder to our findings was that α-diversity was also significantly higher in preterm gestations compared to term gestations. As we found that preterm gestations were higher in AAE, a larger cohort is needed to perform subanalyses and further describe the relationship between AAE, preterm gestational status, and salivary microbial diversity. The finding that α-diversity correlates positively with several adrenal androgens as described above suggests that α-diversity may be more dependent on adrenal androgen levels than preterm gestational status, and that the increase in α-diversity in the preterm group is in part due to the overlap of this group with the AAE cohort.
In this study, genus Peptostreptococcus, Veillonella, and Streptococcus salivarius were significantly increased in the normal weight children with AAE compared to normal weight controls. Peptostreptococcus has been found to be significantly increased in an obese adult cohort31 and associated with periodontal infections49. Veillonella and Streptococcus salivarius have been shown in several studies to be associated with dental caries in both adults and children29,50,51. We also found that compared to overweight/obese controls, overweight/obese children with AAE showed significantly increased Prevotella nanceiensis, genus Abiotrophia, and Neisseria. Prevotella have been shown to predominate in periodontal diseases, systemic inflammation, and metabolic disease52,53,54. One study found that in women with PCOS and gingivitis, Prevotella intermedia levels were significantly higher compared to systemically or periodontally healthy women35. Overall, several of the taxa found to be elevated in our case cohort, compared to weight equivalent controls, have been associated with periodontal disease and oral inflammation.
A significant limitation of our study was lack of oral health histories for the study participants. Further studies are needed in a larger cohort that accounts for oral hygiene and disease to determine whether there are any associations between childhood androgen excess and oral inflammation. As the prevalence of periodontal disease has been shown to be higher in PCOS55,56, it would be of interest to explore whether children with AAE are more likely to exhibit a poorer oral health profile. This study was further limited in its cross-sectional nature; future longitudinal studies that monitor children before and after onset of AAE could better assess the presence of causal relationships between adrenal androgens and salivary microbiome composition.
A major strength of our study was that our cohort was a well-defined group of both boys and girls with AAE, diagnosed by biochemical and clinical signs and based on exclusion of other causes of androgen excess. Additionally, we applied strict criteria to exclude any participants who had taken antibiotics within 3 months or probiotics within 1 month prior to saliva sample collection, greatly reducing the possible impact of antibiotics on their oral microbiome profiles. Furthermore, we collected samples at a consistent time of day, early in the morning after a midnight fast, controlling for the possible impact of eating in the hours before saliva sample collection. With the small sample size, this study serves as a pilot to initially investigate and describe the salivary microbiome in children with AAE; further understanding of the relationship between early androgen excess and the salivary microbiome warrants additional investigation with larger population studies that control for age and oral health status.
In summary, this study uniquely describes the salivary microbiome of children with AAE. α-Diversity was increased in children with AAE, independent of weight status. Genus Peptostreptococcus, Veillonella, and Streptococcus salivarius were significantly increased in normal weight AAE compared to normal weight controls, and overweight/obese AAE showed significantly increased Prevotella nanceiensis, genus Abiotrophia, and Neisseria compared to overweight/obese controls; several of these taxa are associated with periodontal disease and inflammation. Studies with a larger cohort of AAE children with defined oral health status are necessary to illuminate the possible correlations between early androgenic states and oral microbial dysbiosis in children with AAE.
References
Witchel, S. F., Pinto, B., Burghard, A. C. & Oberfield, S. E. Update on adrenarche. Curr. Opin. Pediatr. 32, 574–581 (2020).
Turcu, A. F. & Auchus, R. J. Clinical significance of 11-oxygenated androgens. Curr. Opin. Endocrinol. Diabetes Obes. 24, 252–259 (2017).
Rege, J. et al. 11-Ketotestosterone is the dominant circulating bioactive androgen during normal and premature adrenarche. J. Clin. Endocrinol. Metab. 103, 4589–4598 (2018).
Wise-Oringer, B. K. et al. The unique tole of 11-oxygenated C19 steroids in both premature adrenarche and premature pubarche. Horm. Res Paediatr. 2, 1–10 (2021).
Voutilainen, R. & Jääskeläinen, J. Premature adrenarche: etiology, clinical findings, and consequences. J. Steroid Biochem. Mol. Biol. 145, 226–236 (2015).
Ribeiro, F. A. et al. Metabolic and hormonal assessment of adolescent and young adult women with prior premature adrenarche. Clinics (Sao Paulo) 74, e836 (2019).
Kaya, G. et al. Body mass index at the presentation of premature adrenarche is associated with components of metabolic syndrome at puberty. Eur. J. Pediatr. 177, 1593–1601 (2018).
Silfen, M. E. et al. Elevated free IGF-I levels in prepubertal Hispanic girls with premature adrenarche: relationship with hyperandrogenism and insulin sensitivity. J. Clin. Endocrinol. Metab. 87, 398–403 (2002).
Ibanez, L. et al. Hyperinsulinemia in postpubertal girls with a history of premature pubarche and functional ovarian hyperandrogenism. J. Clin. Endocrinol. Metab. 8, 1237–1243 (1996).
Bäckhed, F. et al. The gut microbiota as an environmental factor that regulates fat storage. Proc. Natl Acad. Sci. USA 101, 15718–15723 (2004).
Lee, C. J., Sears, C. L. & Maruthur, N. Gut microbiome and its role in obesity and insulin resistance. Ann. NY Acad. Sci. 1461, 37–52 (2020).
Turnbaugh, P. J. et al. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 444, 1027–1031 (2006).
Guo, Y. et al. Association between polycystic ovary syndrome and gut microbiota. PLoS ONE 11, e0153196 (2016).
Kelley, S. T., Skarra, D. V., Rivera, A. J. & Thackray, V. G. The gut microbiome is altered in a letrozole-induced mouse model of polycystic ovary syndrome. PLoS ONE 11, e0146509 (2016).
Yurtdaş, G. & Akdevelioğlu, Y. A new approach to polycystic ovary syndrome: the gut microbiota. J. Am. Coll. Nutr. 39, 371–382 (2020).
Insenser, M. et al. Gut microbiota and the polycystic ovary syndrome: influence of sex, sex hormones, and obesity. J. Clin. Endocrinol. Metab. 103, 2552–2562 (2018).
Tetel, M. J., de Vries, G. J., Melcangi, R. C., Panzica, G. & O’Mahony, S. M. Steroids, stress and the gut microbiome-brain axis. J. Neuroendocrinol. 30, https://doi.org/10.1111/jne.12548 (2018).
Sherman, S. B. et al. Prenatal androgen exposure causes hypertension and gut microbiota dysbiosis. Gut Microbes 9, 400–421 (2018).
Gulan, T., Yeernuer, T., Sui, S. & Mayinuer, N. A rat model of maternal polycystic ovary syndrome shows that exposure to androgens in utero results in dysbiosis of the intestinal microbiota and metabolic disorders of the newborn rat. Med Sci. Monit. 25, 9377–9391 (2019).
Barroso, A. et al. Neonatal exposure to androgens dynamically alters gut microbiota architecture. J. Endocrinol. 247, 69–85 (2020).
Mammadova, G., Ozkul, C., Yilmaz Isikhan, S., Acikgoz, A. & Yildiz, B. O. Characterization of gut microbiota in polycystic ovary syndrome: findings from a lean population. Eur. J. Clin. Invest. 51, e13417 (2021).
Jobira, B. et al. Obese adolescents with PCOS have altered biodiversity and relative abundance in gastrointestinal microbiota. J. Clin. Endocrinol. Metab. 105, e2134–e2144 (2020).
Torres, P. J. et al. Gut microbial diversity in women with polycystic ovary syndrome correlates with hyperandrogenism. J. Clin. Endocrinol. Metab. 103, 1502–1511 (2018).
Liu, R. et al. Dysbiosis of gut microbiota associated with clinical parameters in polycystic ovary syndrome. Front. Microbiol. 8, 324 (2017).
Vrieze, A. et al. Transfer of intestinal microbiota from lean donors increases insulin sensitivity in individuals with metabolic syndrome. Gastroenterology 143, 913–6.e7 (2012). Erratum in: Gastroenterology. 144, 250 (2013).
Zeng, B. Structural and functional profiles of the gut microbial community in polycystic ovary syndrome with insulin resistance (IR-PCOS): a pilot study. Res. Microbiol. 170, 43–52 (2019).
He, F. F. & Li, Y. M. Role of gut microbiota in the development of insulin resistance and the mechanism underlying polycystic ovary syndrome: a review. J. Ovarian Res. 13, 73 (2020).
Belstrøm, D. The salivary microbiota in health and disease. J. Oral. Microbiol. 12, 1723975 (2020).
Xiao, J., Fiscella, K. A. & Gill, S. R. Oral microbiome: possible harbinger for children’s health. Int J. Oral. Sci. 12, 12 (2020).
Mameli, C. et al. Taste perception and oral microbiota are associated with obesity in children and adolescents. PLoS ONE 14, e0221656 (2019).
Wu, Y., Chi, X., Zhang, Q., Chen, F. & Deng, X. Characterization of the salivary microbiome in people with obesity. PeerJ 16, e4458 (2018).
Triosi, J. et al. Metabolomic salivary signature of pediatric obesity related liver disease and metabolic syndrome. Nutrients 11, 274 (2019).
Janem, W. F. et al. Salivary inflammatory markers and microbiome in normoglycemic lean and obese children compared to obese children with type 2 diabetes. PLoS ONE 12, e0172647 (2017).
Lindheim, L. et al. The salivary microbiome in polycystic ovary syndrome (PCOS) and its association with disease-related parameters: a pilot study. Front Microbiol 7, 1270 (2016).
Akcalı, A. et al. Association between polycystic ovary syndrome, oral microbiota and systemic antibody responses. PLoS ONE 9, e108074 (2014).
Pappa, E., Kousvelari, E. & Vastardis, H. Saliva in the “omics” era: a promising tool in paediatrics. Oral. Dis. 25, 16–25 (2019).
Chou, J. H., Roumiantsev, S. & Singh, R. PediTools electronic growth chart calculators: applications in clinical care, research, and quality improvement. J. Med. Internet Res. 22, e16204 (2020).
Shypailo, R. J. Age-Based Pediatric Blood Pressure Reference Charts. Baylor College of Medicine, Children’s Nutrition Research Center, Body Composition Laboratory, Houston, TX. https://www.bcm.edu/bodycomplab/BPappZjs/BPvAgeAPPz.html (2019).
Fernández, J. R., Redden, D. T., Pietrobelli, A. & Allison, D. B. Waist circumference percentiles in nationally representative samples of African-American, European-American, and Mexican-American children and adolescents. J. Pediatr. 145, 439–444 (2004).
Wright, C., O’Day, P., Alyamani, M., Sharifi, N. & Auchus, R. J. Abiraterone acetate treatment lowers 11-oxygenated androgens. Eur. J. Endocrinol. 182, 413–421 (2020).
de Ferranti, S. D. et al. Prevalence of the metabolic syndrome in American adolescents: findings from the Third National Health and Nutrition Examination Survey. Circulation 110, 2494–2497 (2004).
Callahan, B. J. et al. DADA2: high-resolution sample inference from Illumina amplicon data. Nat. Methods 13, 581–583 (2016).
DeSantis, T. Z. et al. Greengenes, a chimera-checked 16S rRNA gene database and workbench compatible with ARB. Appl Environ. Microbiol. 72, 5069–5072 (2006).
McMurdie, P. J. & Phyloseq, H. S. An R package for reproducible interactive analysis and graphics of microbiome census data. PLoS ONE 8, e61217 (2013).
Love, M. I., Huber, W. & Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 15, 550 (2014).
Westfall P. H. & Young S. S. Resampling-Based Multiple Testing: Examples and Methods for P-Value Adjustment (Wiley, 1993).
Turnbaugh, P. J. et al. A core gut microbiome in obese and lean twins. Nature 457, 480–484 (2009).
Le Chatelier, E. et al. Richness of human gut microbiome correlates with metabolic markers. Nature 500, 541–546 (2013).
Riggio, M. P., Lennon, A. & Smith, A. Detection of peptostreptococcus micros DNA in clinical samples by PCR. J. Med. Microbiol. 50, 249–254 (2001).
Zhou, J. et al. Exploration of human salivary microbiomes—insights into the novel characteristics of microbial community structure in caries and caries-free subjects. PLoS ONE 11, e0147039 (2016).
Gross, E. L. et al. Beyond Streptococcus mutans: dental caries onset linked to multiple species by 16S rRNA community analysis. PLoS ONE 7, e47722 (2012).
Alauzet, C., Marchandin, H. & Lozniewski, A. New insights into Prevotella diversity and medical microbiology. Future Microbiol. 5, 1695–1718 (2010).
Larsen, J. M. The immune response to Prevotella bacteria in chronic inflammatory disease. Immunology 151, 363–374 (2017).
Zhu, C. et al. The predictive potentiality of salivary microbiome for the recurrence of early childhood caries. Front, Cell Infect. Microbiol. 8, 423 (2018).
Porwal, S., Tewari, S., Sharma, R. K., Singhal, S. R. & Narula, S. C. Periodontal status and high-sensitivity C-reactive protein levels in polycystic ovary syndrome with and without medical treatment. J. Periodontol. 85, 1380–1389 (2014).
Rahiminejad, M. E. et al. Comparison of prevalence of periodontal disease in women with polycystic ovary syndrome and healthy controls. Dent. Res J. (Isfahan) 12, 507–512 (2015).
Acknowledgements
We thank the members of the Division of Pediatric Endocrinology, Diabetes and Metabolism at Columbia University Irving Medical Center (New York, NY) for their referral of eligible subjects, and the subjects and their families for agreeing to participate. We thank the members of the Microbiome & Pathogen Genomics Collaborative Center for technical support. We thank Rachel Tao, B.A., for her initial help with patient recruitment and coordination of study visits. We also thank Ismael Castaneda, R.N. and the staff of the Clinical Research Resource at Columbia Irving Institute for Clinical and Translational Research (UL1TR001873) for their valuable help in conducting the study visits. With gratitude we acknowledge Esoterix Laboratory and the Columbia Biomarkers Core Laboratory for performing laboratory measurements for this study. This work was supported in part by the National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases Grant 5T32DK065522-14 (to B.K.W.-O. and S.E.O.) and by the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant Number UL1TR001873. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Author information
Authors and Affiliations
Contributions
B.K.W.-O., A.C.B., H.P., R.J.A., S.E.O., and A.-C.U. made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data. B.K.W.-O., A.C.B., H.P., S.E.O., and A.-C.U. were involved in drafting the article or revising it critically for important intellectual content. R.J.A., S.E.O., and A.-C.U. provided final approval of the version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent statement
Informed consent was obtained for all study subjects prior to enrollment. For patients less than 7 years of age, informed consent was obtained from the parent or legal guardian. For patients 7 years or older, informed consent and assent were obtained.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wise-Oringer, B.K., Burghard, A.C., Park, H. et al. Salivary microbiome differences in prepubertal children with and without adrenal androgen excess. Pediatr Res 91, 1797–1803 (2022). https://doi.org/10.1038/s41390-021-01661-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-021-01661-w
