
Abstract
Background
One pressing question in the field of pediatrics is whether a dose–response relation is observed between hours of screen time and child outcomes. This study examined the association between hours of screen time (≤1 vs 2 vs ≥3 h/day) and children’s developmental and behavioral outcomes.
Methods
This study included data from 1994 mothers and children in Calgary, Canada, drawn from the All Our Families cohort. At 36 months, children’s screen time (h/day), behavior problems, developmental milestones, and vocabulary acquisition were assessed via maternal report. Socio-demographic factors and baseline levels of performance at 24 months were included as covariates.
Results
Compared to ≤1 h/day (47%; n = 935), children using screens 2 h (36%; n = 725) or ≥3 h/day (17%; n = 333) had an increased likelihood of reported behavioral problems (adjusted odds ratio (AOR) 1.30–1.90), delayed achievement of developmental milestones (AOR 1.41–1.68), and poorer vocabulary acquisition (AOR 1.94).
Conclusions
At 36 months, an association was observed between screen time and children’s developmental, language, and behavioral outcomes, suggesting that duration of screen time is associated with poor child development outcomes. Findings provide support for screen time guidelines and emphasize the need for childcare professionals to discuss screen time guidelines with families.
Impact
-
International guidelines recommend that preschoolers spend no more than 1 h/day viewing screens.
-
Research is needed to determine if there is a relation between screen time levels and child developmental and behavioral outcomes.
-
Compared to ≤1 h/day, children viewing screens 2 or ≥3 h/day had an increased likelihood of behavioral problems, delayed achievement of developmental milestones, and poorer vocabulary acquisition.
-
Findings highlight the association between duration of screen time and factors of child development.
Similar content being viewed by others


Introduction
Children’s capacity for developmental learning is shaped or molded by the experiences they receive in early childhood.1 One rapidly evolving environmental experience for young children is exposure to digital media. Digital media and screen time are now pervasive in the lives of young children, and the rate of media accessibility and consumption is increasing.2 In 2017, 42% of children under the age of eight had their own media device, a substantial increase from 7% in 2013.2 Although the World Health Organization, as well as several national pediatric societies, has issued screen time guidelines3,4,5 suggesting that preschoolers receive no more than 1 h of screen time per day, only a small minority of families in North America meet these recommendations.3,6 For example, in a sample of 151 preschoolers, Lee et al. found that only 15% were meeting the screen time guidelines.7
Although the quality of screen use, specifically the context (i.e., co-viewing) and content (i.e., educational programming) of use, may differentially impact development,8,9,10 research in preschool-aged children demonstrates that duration of screen time is likely consequential for children’s developmental health. For example, Carson et al. showed that exceeding screen time guidelines at 36 months of age related to increased behavior problems.11 Madigan et al. also confirmed the directional association from duration of screen time to child developmental outcomes: increased screen time at 24 and 36 months of age was associated with delays in achieving developmental milestones at 36 and 54 months, respectively.12 Nonetheless, the screen time guideline of ≤1 h/day continues to be publicly critiqued for not being sufficiently evidence-based, which in turn may lower adherence in disseminating this information.13 One pressing question in the field of pediatrics is whether a dose–response relation is observed between hours of screen time and child outcomes, in a manner consistent with the screen time guidelines of no more than 1 h/day for children aged 2–5 years.5 This work is particularly important to conduct in preschoolers, as research shows that once patterns of screen time habits are established, they tend to solidify over time.14,15
Past research has generally examined screen time as a continuous measure or dichotomized as meeting/exceeding guidelines.11,12,16 However, there is a need to attain a clearer understanding of the child development outcomes associated with > or ≤1 h/day of screen time to support or refute current guidelines and to increase the dissemination and uptake of screen time guidelines. Recent research suggests that mean daily screen time for preschool children (1–3 years) in North America ranges from 0 min to 3.3 h/day.14
The aim of the current study of 1994 preschoolers was to examine whether ≤1 vs 2 h/day or ≥3 h/day of screen time (i.e., TV, computer, video games) exposure was associated with poor performance on a broad range of developmental outcomes, including child behavior problems (e.g., hyperactivity, inattention, low mood, anxiety), achievement of developmental milestones (e.g., age-appropriate language, fine motor, gross motor, and social skills), and language acquisition (e.g., vocabulary use) at 36 months. In addition, we sought to examine whether significant differences exist between children viewing 1, 2, or ≥3 h/day in order to further support, or refute, current screen time guidelines. We hypothesized that children exposed to screen time above the recommended 1 h/day threshold would exhibit poor performance on measures assessing behavior, developmental milestones, and language acquisition. In addition, in line with studies examining screen time as a continuous predictor and showing that increased duration relates to poorer outcomes,12 we hypothesized that children viewing ≥3 h/day would have significantly poorer child development outcomes when compared to children viewing 2 h/day.
Methods
Study design and population
Participants were from All Our Families, a pregnancy cohort of mothers and children from Calgary, Canada.17 Women were recruited between August 2008 and December 2010 through primary health care offices, community advertising, and laboratories. Inclusion criteria were: (1) ≥18 years, (2) fluent in English, (3) gestational age <25 weeks, and (4) receiving community-based prenatal care. Mothers completed two questionnaires during pregnancy and at 4, 12, 24, and 36 months postpartum. The 36-month time point (N = 1994; April 2012–October 2014) was the focus of this analysis as screen time and the outcome variables of interest were collected. Baseline levels of performance at 24 months (October 2011–October 2013) were included as covariates. A detailed description of the study sample can be found in Table 1. All participants provided written informed consent to participate. Procedures were approved by the institutional ethics board.
Exposure
Screen time
A single item from the Nutrition Screening Tool for Every Preschooler (NutriSTEPTM)18 was used to measure hours of screen time. Mothers indicated the time their child spent “watching TV, using the computer, and playing video games” on a typical day. Response options ranged from 1 h or less a day (1) to 5 h or more a day (5). Because a low number of participants endorsed 4 h (n = 67) and 5 h or more a day (n = 25), these response options were collapsed into ≤1, 2, or ≥3 h/day.
Outcomes
Child behavior
Internalizing and externalizing behavior was measured using the National Longitudinal Survey of Children and Youth behavior scales,19 which uses adapted questions from the Child Behavior Checklist (CBCL; ref. 20) Four domains of child behavior were assessed at 36 months: Hyperactivity/Inattention; Physical Aggression; Emotional Disorder/Anxiety; and Separation Anxiety. The former two subscales comprise externalizing behaviors (raw score range 0–28) and the latter two comprise internalizing behaviors (raw score range 0–20), with higher scores indicating greater problem behavior. Chronbach’s αs in our sample range from 0.58 (Separation Anxiety) to 0.80 (Hyperactivity/Inattention). At 24 months, mothers completed the Brief Infant Toddler Social Emotional Assessment (BITSEA; ref. 21) providing a measure of baseline levels of child problem behaviors. The problem subscale from the BITSEA has shown high concurrent and predictive validity with the CBCL.21 The problem subscale showed adequate reliability in the current sample (α = 0.70).
Developmental screener
At 24 and 36 months of age, mothers completed the Ages and Stages Questionnaire, Third Edition (ASQ-3; ref. 22) The ASQ-3 is a parent-report screening measure used to evaluate developmental progress in five domains: communication, gross motor, fine motor, problem solving, and personal-social. Consistent with previous research,12,23 a summed ASQ-3 score across all domains was used (lower raw scores indicate poorer development). The ASQ-3 has good psychometric properties and is commonly used as a pediatric screening tool.22 When testing for delays in achievement of developmental milestones at 36 months, the acquisition of developmental milestones at 24 months was controlled.
Language acquisition
The MacArthur–Bates Communicative Development Inventory (CDI; ref. 24) was used to assess language acquisition at 24 months (Words and Sentences version) and 36 months of age (CDI-III version). When testing for language outcomes at 36 months, the proportion of words/sentences endorsed at 24 months was controlled. Lower scores indicate poorer language development. The CDI is a well-validated measure used with healthy and impaired language learners.25
Covariates
Analyses controlled for mother and child age (years and months, respectively), child sex (1 [female]; 0 [male]), maternal education (1 [some elementary or high school] to 6 [completed graduate school]), maternal stress (Perceived Stress Scale (PSS); ref. 26) and household income (1 [≤29,999 CAD$] to 11 [≥$150,000 CAD$]). Dual language learner (DLL) was added when modeling language acquisition (Yes [1; ≥12 h/day/7 days a week of other language spoken in the home]; No [0]) to account for differences in language outcomes by DLL status. The demographic covariates were chosen because they are known to be associated with both screen time and child development outcomes.
Statistical analysis
The screen time variable was dummy coded to allow for comparison between children who view screens ≤1 (reference group), 2, or ≥3 h/day. Using multiple logistic regression, we examined the association between screen time and relative “at-risk” scores (dichotomized; yes/no) for all outcome variables. For the CBCL and CDI, relative at-risk cut-off classifications (yes/no) were created using a cut-point of one standard deviation above (internalizing, externalizing) or below (language) the sample mean. This method was used for the modified CBCL because the standardized cut-off scores for the original measure cannot be used for a modified version, as is the case herein. Similarly, this method was used for the CDI because clear at-risk cut-off scores have not been established for this measure. For achievement of developmental milestones, the standardized ASQ cut-off score for each domain was used.22 Consistent with the scoring manual,22 if a child scored within the “further assessment with a professional” (two standard deviations below the mean) or the “provide learning activities and monitor” (one standard deviation below the mean) range for any domain, they were considered at risk for the purpose of this study (1 [delay in one or more developmental domain]; 0 [no delays]). Odds ratios (ORs) with 95% confidence intervals (CIs) were used, with significance set at p < 0.05. All analyses were conducted in Mplus, version 8.1.27
Missing data
From the initial pregnancy cohort (N = 3388), 95% (N = 3223) agreed to be contacted for follow-up research. Of those who agreed to follow-up and were eligible at the time of questionnaire completion, 69% completed the 36-month questionnaire (N = 1994) and screen time data were available for 99.9% of these participants (n = 1993). Attrition rates observed in the current study are similar to other prospective birth cohorts.28 Predictors of drop out were younger mothers (t (3279) = 3.94, p < 0.001), lower income (t (3248) = 7.91, p < 0.001), lower maternal education (t (3352) = 6.26, p < 0.001), and minoritized ethnicities (χ2(1) =38.25, p < 0.001). In order to account for missing data, models were run with robust maximum likelihood and Monte Carlo integration.29 Findings were considered significant at the p < 0.05, two-tailed level.
Results
Descriptive statistics
On a typical day, 47% (n = 935) of children were viewing screens ≤1 h/day, 36% (n = 725) 2 h/day, and 17% (n = 333) ≥3 h/day. There were no significant differences by sex for reported screen time. Of those who completed all items of the questionnaire at 36 months, 25% of children were in the at-risk range for externalizing difficulties (n = 489) and internalizing (n = 478) difficulties, 17% (n = 327) for language delays, and 32% (n = 567) for delays in achieving developmental milestones.
Screen time and behavior problems
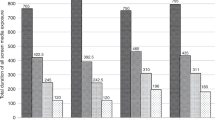
When comparing the screen time categories of ≤1 vs 2 vs ≥3 h/day and relative at-risk status (yes/no), there was an overall effect of screen time (internalizing: Wald χ2(2) = 22.15, p < 0.001; externalizing: Wald χ2(2) = 11.89, p = 0.003; Fig. 1 and Table 2). After adjusting for all covariates, children exposed to 2 vs ≤1 h/day of screen time were more likely to score in the at-risk range for internalizing (OR 1.36, 95% CI 1.06–1.73) and externalizing (OR 1.30, 95% CI 1.02–1.65) problems. Children exposed to ≥3 vs ≤1 h/day of screen time were more likely to score in the at-risk range for internalizing (OR 1.90, 95% CI 1.41–2.55) and externalizing problems (OR 1.66, 95% CI 1.23–2.23). Further, the effect of 2 h/day of screen time significantly differed from ≥3 h/day for internalizing (Wald χ2(1) = 6.82, p = 0.009) problems, but not for externalizing (Wald χ2(1) = 3.44, p = 0.064) problems.

Notes. Error bars represent 95% confidence intervals. Columns that share subscripts are not significantly different from each other. Models presented include covariates. Overall effect of screen time viewing on: a. internalizing at-risk status; b. externalizing; c. developmental milestone achievement; and d. language acquisition.
Screen time and developmental milestones
When comparing the screen time categories of ≤1 vs 2 vs ≥3 h/day and at-risk status (yes/no) for delayed achievement of developmental milestones, there was an overall effect of screen time (Wald χ2(2) = 11.79, p = 0.003; Fig. 1 and Table 2). After adjusting for all covariates, compared to ≤1 h/day, children exposed to 2 h/day of screen time were more likely to score at-risk for delayed achievement of developmental milestones (OR 1.41, 95% CI 1.10–1.79). Further, children exposed to ≥3 vs ≤1 h/day of screen time were more likely to score at-risk for delayed achievement of developmental milestones (OR 1.68, 95% CI 1.23–2.30). Lastly in this model, the effect of 2 h/day of screen time was not significantly different from ≥3 h/day (Wald χ2(1) = 1.39, p = 0.238).
Screen time and language acquisition
When comparing the screen time categories of ≤1 vs 2 vs ≥3 h/day and relative at-risk status (yes/no) for delayed language acquisition, there was an overall effect of screen time (Wald χ2(2) = 11.76, p = 0.003; Fig. 1 and Table 2). After adjusting for all covariates, children exposed to 2 h/day of screen time did not significantly differ from children who viewed screens ≤1 h/day (OR 1.16, 95% CI 0.84–1.62), but children exposed to ≥3 h/day of screen time were more likely to score at risk for delayed language acquisition when compared to children who viewed screens ≤1 h/day (OR 1.94, 95% CI 1.29–2.91). Lastly in this model, the effect of 2 h/day of screen time was significantly different from ≥3 h/day (Wald χ2(1) = 7.26, p = 0.007).
Discussion
As the digital landscape is rapidly changing, children are becoming more enmeshed in a technological world. With these changes comes a critical need for evidence-based research to establish the associations between levels of screen time duration and child developmental outcomes. Results of the current study establish that different levels of screen time relate to a variety of preschool outcomes. Specifically, we found that consistent with the World Health Organization screen time guidelines5 of no more than 1 h/day of screen time for preschoolers, screen time above the recommended 1 h guideline was associated with increased odds of at-risk internalizing and externalizing problems and at-risk delays in achievement of developmental milestones. In addition, screen time duration >2 h/day was associated with at-risk delays in language acquisition. Overall, the strongest associations observed were between the longest threshold of screen time (≥3 h/day) and internalizing problems and at-risk delays in language acquisition, respectively.
One mechanism that may explain the relation between increased levels of screen time and poor developmental outcomes may be the displacement of these learning opportunities. Outside the educational content or shared screen time experiences (i.e., co-viewing; ref. 8), when children are engaging in long durations of screen time, they may be missing out on opportunities to practice skills important for developmental tasks (e.g., language acquisition, motor skills, behavioral regulation). While there is support for the impact of screen time and displacement of parent–child interactions on child behavior problem outcomes,30 additional research is needed to elucidate the direct relation between displacement of day-to-day learning opportunities by the use of screens and child development outcomes. While this is a viable explanation for the current findings, it is also important to consider that the direction of the observed relations cannot be established based on the current study design. It is possible, for example, that children with poor developmental outcomes or behavioral problems received longer durations of screen time to help modulate challenging behaviors. A recent test of the bi-directional associations between screen time and achievement of developmental milestones across early childhood suggests that screen use leads to delayed achievement of developmental milestones;12 however, research on directionality of associations between screen time and internalizing an externalizing behavior in children has been mixed.31,32 Future research is also needed to examine the role of buffering, or protective factors (e.g., physical activity, parent–child interactions, sleep, etc.), when determining the direction and magnitude of the associations between screen time and child development outcomes.
Although the magnitude of the associations found in the current study vary, the pattern of the association between increased duration of screen time and poor measures of child development was consistent across multiple domains. These findings align with past studies examining screen time as a continuous predictor of child outcomes and when examining screen time based on meeting or exceeding the 1 hr/day guideline.11,12 Also consistent with past research in the field of digital media use in children, the effect sizes observed herein are significant, but small.33
Internalizing behaviors and language acquisition exhibited a dose–response relation where ≥3 h/day of screen time related to poorer developmental outcomes when compared to 2 h/day. For externalizing behaviors and at-risk delays in achievement of developmental milestones, there was no significant difference for children viewing 2 vs ≥3 h/day. After controlling for confounds (e.g., previous levels of behavior, parent education, family income, etc.), the results suggest that after the 1 h/day threshold, the association between screen time and delayed achievement of developmental milestones, and screen time and externalizing problems, respectively, were comparable. Thus, signaling the potential for a plateau effect where achievement of developmental milestones and externalizing problems are equally impacted after a particular threshold (in this case >1 h/day).
Taken together, the results from this study highlight that different levels of screen time duration differentially relate to a variety of child development outcomes. Consistent with past commentaries10 and recent calls for more nuanced data examining screen use for young children and the family media ecology,34 there is a need for a greater understanding of the differential impact of varying levels of screen time for children, as some children are likely to be more affected by screen-based media exposure than others.33 Moreover, screen time is likely one of many environmental determinants that can create disparities in children’s developmental trajectories.12 Without intervention, it has been shown that gaps in early childhood development can widen over time.35 This study supports a relation between screen time and developmental outcomes at 36 months of age, which reveals that many children who are being exposed to >1 h/day of screen time are also performing below their same-age peers; thus, setting the stage or adding to the disparities that are observed as children develop.
Findings from this study support the need for practitioners to review the importance of limiting the duration of screen time for preschoolers. Encouraging and supporting parents to use a Family Media Plan36 to help manage and monitor how, when, and where screens are used in the home, may be particularly helpful. In addition to these screen time-specific strategies, families should also be supported to engage in the day-to-day activities that have been consistently shown to promote healthy child development (e.g., reading, free time play, outdoor exploration, etc.37,38).
Limitations
The findings from this study must be interpreted with the following limitations in mind. First, the method of measurement used for screen time did not capture families who abstained from media use. Future research may explore the differences, if any, between non-screen viewing children and those who receive ≤1 h/day. In addition, data collection for this study was completed in 2014 and did not include mobile device use (e.g., tablets). Second, while parents are arguably the best informants of child outcomes at 36 months, single informant measurement introduces the potential for bias. Specific to screen time, self-report and passive sensing of screen time have not been highly correlated and a majority of parents underreport screen time.39 The findings from this study would be strengthened if replicated with passive sensing measures as well as objective measures of developmental outcomes. Third, the current sample was socio-demographically homogeneous. While this is representative of the region of data collection, it limits the generalizability of the study findings. Also, participants lost to follow-up were young mothers with lower levels of income and education and were more likely to identify as part of a minoritized ethnic/racial group. Given that many of these factors have previously been related to poorer child development outcomes and higher durations of screen time,14,15 the current results may be an underestimation of the association between screen time and preschool children’s developmental and behavioral outcomes. In addition, the at-risk cut-offs for the analyses were based on the sample and are not considered clinically at risk. Lastly, although consistent with longitudinal research,12,40,41,42 the current study presents cross-sectional findings and directional associations cannot be assumed. The strength of the statistical design is improved by controlling for baseline levels of the child development outcomes, but this does not rule out the possibility that a third confounding variable (e.g., family or parenting factors) impacts both screen time and developmental outcomes, or that children with poorer behavioral or developmental status may receive more screen time.
Conclusions
We are living in a high digital consumption era with a continuously changing digital landscape where children are easily and frequently exposed to media devices. Given this unchartered digital territory, there is a critical need to understand the association between screen time and children’s developmental outcomes. This study demonstrates that for preschool children, a relation exists between screen time and measures of behavior, development, and language. When compared to children exposed to screens ≤1 h/day, children viewing 2 and ≥3 h/day have increased odds of at-risk behavior problems and delayed achievement of developmental milestones and language acquisition. This study can be used to inform practitioners, policy makers, and families of the association between levels of screen time and measures of child development. The findings support family-focused media recommendations to encourage engagement with technology in an age-appropriate way during a sensitive period of child development.
References
Son, S. H. & Morrison, F. J. The nature and impact of changes in home learning environment on development of language and academic skills in preschool children. Dev. Psychol. 46, 1103–1118 (2010).
Rideout, V. The Common Sense Census: Media Use by Kids Zero to Eight (Common Sense Media, 2017).
American Academy of Pediatrics Council on Communications and Media. Media and young minds. Pediatrics 138, e20162591 (2016).
Ponti, M. et al. Screen time and young children: promoting health and development in a digital world. Paediatr. Child Health 22, 461–468 (2017).
World Health Organization. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children Under 5 Years of Age (World Health Organization, 2019).
Chaput, J. P. et al. Proportion of preschool-aged children meeting the Canadian 24-Hour Movement Guidelines and associations with adiposity: results from the Canadian Health Measures Survey. BMC Public Health 17, 829 (2017).
Lee, E.-Y. et al. Meeting new Canadian 24-Hour Movement Guidelines for the Early Years and associations with adiposity among toddlers living in Edmonton, Canada. BMC Public Health 17, 155–165 (2017).
Madigan, S., McArthur, B., Anhorn, C., Eirich, R. & Christakis, D. A. Associations between screen use and child language skills. JAMA Pediatr. 174, 665–675 (2020).
Rasmussen, E. E. et al. Relation between active mediation, exposure toDaniel Tiger’s Neighborhood, and US preschoolers’ social and emotional development. J. Child. Media 10, 443–461 (2016).
Christakis, D. A. The effects of infant media usage: what do we know and what should we learn? Acta Paediatr. 98, 8–16 (2009).
Carson, V. et al. Associations between meeting the Canadian 24-Hour Movement Guidelines for the Early Years and behavioral and emotional problems among 3-year-olds. J. Sci. Med. Sport 22, 797–802 (2010).
Madigan, S., Browne, D., Racine, N., Mori, C. & Tough, S. Association between screen time and children’s performance on a developmental screening test. JAMA Pediatr. 173, 244–250 (2019).
Straker, L., Zabatiero, J., Danby, S., Thorpe, K. & Edwards, S. Conflicting guidelines on young children’s screen time and use of digital technology create policy and practice dilemmas. J. Pediatr. 202, 300–303 (2018).
Trinh, M.-H. et al. Association of trajectory and covariates of children’s screen media time. JAMA Pediatr. 174, 71–78 (2020).
McArthur, B., Browne, D., Tough, S. & Madigan, S. Trajectories of screen use during early childhood: predictors and associated behavior and learning outcomes. Comput. Hum. Behav. 113, 106501 (2020).
Zimmerman, F. J., Christakis, D. A. & Meltzoff, A. N. Associations between media viewing and language development in children under age 2 years. J. Pediatr. 151, 364–368 (2017).
Tough, S. C. Cohort Profile: the All Our Babies pregnancy cohort (AOB). Int. J. Epidemiol. 46, 1389–1390k (2017).
Randall Simpson, J. A., Keller, H. H., Rysdale, L. A. & Beyers, J. E. Nutrition Screening Tool for Every Preschooler (NutriSTEP™): validation and test–retest reliability of a parent-administered questionnaire assessing nutrition risk of preschoolers. Eur. J. Clin. Nutr. 62, 770–780 (2008).
Statistics Canada, Human Resources Canada. National Longitudinal Survey of Children NLSCY. Overview of Survey Instruments for 1994–1995 (Statistics Canada, 1995).
Achenbach, T. M. & Ruffle, T. M. The Child Behavior Checklist and related forms for assessing behavioral/emotional problems and competencies. Pediatr. Rev. 21, 265–271 (2000).
Briggs-Gowan, M. J. The brief infant-toddler social and emotional assessment: screening for social-emotional problems and delays in competence. J. Pediatr. Psychol. 29, 143–155 (2004).
Squires, J., Bricker, D. Ages & Stages Questionnaires®, Third Edition (ASQ- 3™). A Parent-Completed Child-Monitoring System (Paul H. Brookes Publishing Co., 2009).
Alvik, A. & Grøholt, B. Examination of the cut-off scores determined by the Ages and Stages Questionnaire in a population-based sample of 6 month-old Norwegian infants. BMC Pediatr. 11, 117 (2011).
Fenson, L. et al. The MacArthur-Bates Communicative Development Inventories: User’s Guide and Technical Manual, 2nd edn (Brookes, 2006).
Heilmann, J., Ellis Weismer, S., Evans, J. & Hollar, C. Utility of the MacArthur-Bates communicative development inventory in identifying language abilities of late-talking and typically developing toddlers. Am. J. Speech Lang. Pathol. 14, 40–51 (2005).
Cohen, S., Kamarck, T. & Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 24, 385–396 (1983).
Muthén, L. & Muthén, B. Mplus Statistical Modeling Software: Release 8.0 (Muthén & Muthén, 2017).
Sontag-Padilla, L. et al. The Urban Child Institue CANDLE Study (Rand Corporation, 2015).
Graham, J. W. Missing data analysis: making it work in the real world. Annu. Rev. Psychol. 60, 549–576 (2009).
McDaniel, B. T. & Radesky, J. S. Technoference: parent distraction with technology and associations with child behavior problems. Child Dev. 89, 100–109 (2018).
Radesky, J. S., Peacock-Chambers, E., Zuckerman, B. & Silverstein, M. Use of mobile technology to calm upset children. JAMA Pediatr. 170, 397 (2016).
Suchert, V., Hanewinkel, R. & Isensee, B. Sedentary behavior and indicators of mental health in school-aged children and adolescents: a systematic review. Prev. Med. 76, 48–57 (2015).
Browne, D., Thompson, D. & Madigan, S. Digital media use in children: clinical versus scientific responsibilities. JAMA Pediatr. 174, 111 (2020).
Barr, R. Growing up in the digital age: early learning and family media ecology. Curr. Direct. Psychol. Sci. 28, 341–346 (2019).
Stanovich, K. E. Matthew effects in reading: some consequences of individual differences in the acquisition of literacy. Read. Res. Q. 21, 360–407 (1986).
American Academy of Pediatrics. Family Media Plan (American Academy of Pediatrics, 2019)
Bento, G. & Dias, G. The importance of outdoor play for young children’s healthy development. Porto Biomed. J. 2, 157–160 (2017).
Mendelsohn, A. L. et al. Reading aloud, play, and social-emotional development. Pediatrics 141, e20173393 (2018).
Yuan, N. et al. How much do parents actually use their smartphones? Pilot study comparing self-report to passive sensing. Pediatr. Res. 86, 416–418 (2019).
Parkes, A., Sweeting, H., Wight, D. & Henderson, M. Do television and electronic games predict children’s psychosocial adjustment? Longitudinal research using the UK Millennium Cohort Study. Arch. Dis. Child. 98, 341–348 (2013).
Allen, M. S. & Vella, S. A. Screen-based sedentary behaviour and psychosocial well-being in childhood: cross-sectional and longitudinal associations. Ment. Health Phys. Act. 9, 41–47 (2015).
Swing, E. L., Gentile, D. A., Anderson, C. A. & Walsh, D. A. Television and video game exposure and the development of attention problems. Pediatrics 126, 214–221 (2010).
Acknowledgements
We acknowledge the contributions of the All Our Families research team and thank the participants who took part in the study. The All Our Families study was supported by Alberta Innovates Health Solutions Interdisciplinary (Team grant 200700595), the Alberta Children’s Hospital Foundation, and the Max Bell Foundation to S.T. Research support was provided by the Canada Research Chairs program to S.M. Postdoctoral Fellowship support was provided by the Alberta Children’s Hospital Research Institute to B.M.
Author information
Authors and Affiliations
Contributions
B.M. and S.M. conceptualized and designed the study, conducted data analyses, drafted the manuscript, and reviewed and revised the manuscript. S.T. conceptualized the cohort study, designed the data collection instruments and study methodology, secured funding for data collection, and reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent statement
All participants provided written informed consent to participate.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
McArthur, B.A., Tough, S. & Madigan, S. Screen time and developmental and behavioral outcomes for preschool children. Pediatr Res 91, 1616–1621 (2022). https://doi.org/10.1038/s41390-021-01572-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-021-01572-w
This article is cited by
-
Mobile device screen time is associated with poorer language development among toddlers: results from a large-scale survey
BMC Public Health (2024)
-
Indirect effects of the COVID-19 pandemic on children relate to the child’s age and experience
Pediatric Research (2023)
-
Embracing Culturally Relevant Computational Thinking in the Preschool Classroom: Leveraging Familiar Contexts for New Learning
Early Childhood Education Journal (2023)
-
Associations of excessive screen time and early screen exposure with health-related quality of life and behavioral problems among children attending preschools
BMC Public Health (2022)
-
Family Factors Associated with Hands-On Play and Screen Time During the COVID-19 Pandemic
Child & Youth Care Forum (2022)
