
Abstract
Adipose tissue is a type of connective tissue composed of closely packed adipocytes with collagenous and elastic fibers. These adipocytes store triglycerides at a high percentage and the estimate of this amount is important for the calculation of body fat mass. For example, magnetic resonance imaging (MRI) measures adipose tissue volume, but adipose tissue density (fat content percentage and density) is required to calculate fat mass. However, in previously published studies, the conversion factor for white adipose tissue density varies from study to study. This paper aimed to investigate the different adipose tissue densities used as conversion factors to clarify differences between studies. Furthermore, we include a new proposal for adipose tissue density and fat content of infants based on the results of recent water–fat MRI studies.
Impact
-
Magnetic resonance imaging (MRI) is one of the methods used to measure body composition in infants and the inherent density of tissue/organs is needed in order to calculate the mass of target organs and tissues.
-
The conversion factor used for white adipose tissue density currently varies from study to study.
-
This article includes a new recommendation for the adipose tissue density and fat content of infants based on the results of recent water–fat MRI studies.
Similar content being viewed by others

Introduction
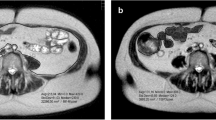
Magnetic resonance imaging (MRI) is one of the methods used to measure body composition in vivo regardless of age. Even in neonates, MRI has been reported as an accurate and highly repeatable way to quantify body composition at the tissue–organ level.1,2 This imaging technique measures the volume (cm3) of a target by continuously summing the cross-sectional areas (cm2) of organs and tissues that are captured in a cross-sectional image. The inherent density of these tissue/organs is then used to calculate the masses of target organs and tissues.
Adipose tissue is a type of connective tissue made up of closely packed adipocytes (i.e., fat cells) with collagenous and elastic fibers. Recently, MRI using chemical shift water–fat separation provided fat fraction percentages of white adipose tissue in healthy humans in vivo3 and in fetuses and infants.4,5 For example, Hu et al.5 reported that the mean fat fraction percentage of white adipose tissue in infants aged 57 days was about 78%. Similar values for the fat fraction percentage have been reported from other infant studies.6,7 In contrast, there is a large difference in the value of fat fraction percentage in white adipose tissue using water–fat MRI when compared with a classical biopsy study. For example, Baker8 reported that the percentage of fat content in adipose tissue was 47% when using biopsy samples obtained from neonates who died (i.e., intracranial hemorrhage) shortly after their birth (within 48 h) or who were stillborn. The value reported by Baker has been used to convert the volume measured by MRI into a mass unit.9 The fat (i.e., triglyceride) density is already known as 0.9 g/cm3. Thus, once the fat fraction percentage in white adipose tissue is determined, it can be used as a conversion factor for calculating fat mass (Formula #1).
Interestingly, the water–fat MRI studies reported that the fat fraction percentage in white adipose tissue of healthy fetuses was 24% at 34 weeks of gestational age4 and about 78% within 6 days of birth.7 These results suggest that the fat fraction percentage of white adipose tissue increases rapidly from the late gestational age to birth.4 It is expected that the samples used in the biopsy study may have reported a low fat fraction percentage of adipose tissue at birth due to the poor development of adipose tissue fat cells late in gestation. In addition to the data from the biopsy study still being used for calculating fat mass, the conversion factor for white adipose tissue density varies from study to study.10,11,12 This is of importance given that this density value is necessary to estimate organ/tissue mass. In order to ensure that the estimate is valid, the appropriate density value must be used. Therefore, the purpose of this manuscript was to investigate the different adipose tissue densities used as conversion factors, to clarify differences between studies, and to make a new proposal for adipose tissue density of infants based on the results of recent MRI studies.
Adipose tissue density determined by three different studies
Rat study by Ross et al.13
In the study by Ross et al.,13 adipose tissue mass was calculated by assuming that the average adipose tissue density was 0.9 g/cm3 (Formula #2). It is known that the density of fat (triglyceride) is 0.9 g/cm3. Thus this formula indicates that all adipose tissue is composed of fat (i.e., 100% fat fraction). The authors described the fat content of adipose tissue in rats using previous studies, but it was not possible to sufficiently distinguish between the fat fraction percentage and the density of adipose tissue. This formula has been used to convert MRI-measured adipose tissue volume to body fat mass in previous human studies.9,11,14,15 One of the human studies9 calculated the adipose tissue mass by multiplying the adipose tissue volume by 0.9 g/cm3 (i.e., density of adipose tissue) and then estimated the fat mass by using the fat fraction percentage that was reported by Baker.8 In reference adult men, adipose tissue is composed of approximately 80% fat, 5% protein, and 15% water, which results in a density of 0.916 g/cm3.16 If the neonate’s adipose tissue contains more water (density, 1.0 g/cm3) than fat (density, 0.9 g/cm3) when compared to adults, then the density of the adipose tissue is likely to be higher than that of the adults (0.916 g/cm3). Thus it may not be appropriate to use 0.9 g/cm3 as the adipose tissue density.
Infant biopsy study by Kabir and Forsum
Several studies1,2,10 used the conversion factor reported by Kabir and Forsum17 to calculate fat mass from adipose tissue volume measured by MRI (Formula #3). In that study,17 the authors measured the chemical compositions of infant adipose tissue using biopsy samples. They reported that adipose tissue contained 71% fat, 26% water, and 4% fat-free solids in infants aged 5.5 months (6.8 kg body mass and 63 cm body height). Assuming that adipose tissue only contains fat, water, and fat-free solids, the adipose tissue density was calculated from each of its component respective densities (fat 0.9 g/cm3; water 1.012 g/cm3; fat-free solids 1.4 g/cm3) and their proportions. The final calculated density by the Kabir and Forsum was 0.66 g/cm3. When calculating the fat fraction percentage, there are two processes, i.e., volume ratio and mass ratio. Since MRI measures the adipose tissue volume, it is desirable that the percentage of fat content should be the volume ratio of the adipose tissue. While water–fat MRI provides the quantitative ratio of signals (volume) from lipids and water in tissues, a biopsy measures the mass of each component to calculate the ratio.
Combination of adipose tissue density and percentage of fat content
In the study by Gale et al.,12 two conversion factors, i.e., adipose tissue density and fat content percentage were used to calculate subcutaneous and intra-abdominal fat mass from adipose tissue volume in infants (Formula #4). The density of adipose tissue obtained from unembalmed cadavers was 0.987 g/cm3,18 and the fat content percentage obtained from neonates who died at birth or during the first week of life was 42.9%.19 As mentioned earlier, biopsy samples of neonates, such as stillbirths, may have poorly developed adipose tissue fat cells late in gestation. It is not clear, but it seems that this fat fraction percentage needs to be treated with caution in the future. In addition, the authors used adipose tissue density (0.987 g/cm3) rather than fat density (0.9 g/cm3). As can be seen from Formula #4, the authors used adipose tissue density, and when multiplied by the fat content, the final calculation represented the amount of adipose tissue mass, not the amount of fat mass.
Our proposal and future task
Fat density is required to calculate the amount of fat mass from the volume of adipose tissue containing fat. Assuming that fat density (0.9 g/cm3) is constant during the growth process, the fat fraction percentage in adipose tissue is an important conversion factor for calculating fat mass (Formula #1). There are two methods, biopsy and water–fat MRI, to measure the fat fraction percentage of adipose tissue in neonates and infants. Water–fat MRI is considered to be suitable for obtaining the value of adipose tissue fat fraction percentage in healthy infants. We have calculated the mean value (72%) of adipose tissue fat fraction in infants within the first month of life using three previously reported studies.5,6,7 Thus the fat fraction percentage for converting the adipose tissue volume measured by MRI to fat mass is 72% for neonates who are within 1 month of birth. However, due to a lack of research, it is impossible to provide the change in fat fraction percentage of white adipose tissue after 1 month of birth. It is also unknown whether the adipose tissue fat fraction percentage differs between preterm and term infants or between breastfeeding and formula feeding.
There is no doubt that future research is needed, but one study is noteworthy. The study measured the adipose tissue fat fraction of the Bichat’s fat pad in infants between the ages of 1 day and 10 months.20 The masticatory fat pad is a unique adipose tissue that transforms from brown adipose tissue to white adipose tissue in early postnatal life. The authors reported that the fat fraction percentage in the masticatory fat pad increased from birth to 1 month old and then was maintained at a similar level until 10 months old.20 Assuming that the same phenomenon occurs in white adipose tissue, it is expected that the fat fraction percentage will reach the level of children (about 87%) around the first month of life.3 Overall, differences exist between neonates and adults, but clearer standards need to be used to accurately determine the fat mass in infants.
References
Harrington, T. A. M. et al. Fast and reproducible method for the direct quantitation of adipose tissue in newborn infants. Lipids 37, 95–100 (2002).
Olhager, E., Flinke, E., Hannerstad, U. & Forsum, E. Studies on human body composition during the first 4 months of life using magnetic resonance imaging and isotope dilution. Pediatr. Res. 54, 906–912 (2003).
Abe, T. et al. The water-fat separation method for determining the fat-free component of subcutaneous adipose tissue in humans: a brief review. J. Clin. Densitom. 23, 390–394 (2020).
Giza, S. A. et al. Measuring fetal adipose tissue using 3D water-fat magnetic resonance imaging: a feasibility study. J. Meter. Fetal Neonatal Med. 33, 831–837 (2020).
Hu, H. H. et al. Comparison of brown and white adipose tissues in infants and children with chemical-shift-encoded water-fat MRI. J. Magn. Reson. Imaging 38, 885–896 (2013).
Rasmussen, J. M. et al. Brown adipose tissue quantification in human neonates using water-fat separated MRI. PLoS ONE 8, e77907 (2013).
Hu, H. H. et al. MRI detection of brown adipose tissue with low fat content in newborns with hypothermia. Magn. Reson. Imaging 32, 107–117 (2014).
Baker, G. L. Human adipose tissue composition and age. Am. J. Clin. Nutr. 22, 829–835 (1969).
Harrington, T. A. M., Thomas, E. L., Frost, G., Modi, N. & Bell, J. D. Distribution of adipose tissue in the newborn. Pediatr. Res. 55, 437–441 (2004).
Olhager, E., Thuomas, K. A., Wigstrom, L. & Forsum, E. Description and evaluation of a method based on magnetic resonance imaging to estimate adipose tissue volume and total body fat in infants. Pediatr. Res. 44, 572–577 (1998).
Uthaya, S. et al. Altered adiposity after extremely preterm birth. Pediatr. Res. 57, 211–215 (2005).
Gale, C., Santhakumaran, S., Wells, J. C. K. & Modi, N. Adjustment of directly measured adipose tissue volume in infants. Int. J. Obes. 38, 995–999 (2014).
Ross, R., Leger, L., Guardo, R., de Guise, J. & Pike, B. G. Adipose tissue volume measured by magnetic resonance imaging and computerized tomography in rats. J. Appl. Physiol. 70, 2164–2172 (1991).
Golab, B. P., Voerman, E., van der Lugt, A., Santos, S. & Jaddoe, V. W. V. Subcutaneous fat mass in infancy and abdominal, pericardial and liver assessed by magnetic resonance imaging at the age of 10 years. Int. J. Obes. 43, 392–401 (2019).
Modi, N. et al. Determinants of adiposity during preweaning postnatal growth in appropriately grown and growth-restricted term infants. Pediatr. Res. 60, 345–348 (2012).
International Commission on Radiological Protection. Report of the Task Group on Reference Man. ICRP Publication 23 (Pergamon Press, 1975).
Kabir, N. & Forsum, E. Estimation of total body fat and subcutaneous adipose tissue in full-term infants less than 3 months old. Pediatr. Res. 34, 448–454 (1993).
Martin, A. D., Daniel, M. Z., Drinkwater, D. T. & Clarys, J. P. Adipose tissue density, estimated adipose lipid fraction and whole body adiposity in male cadavers. Int. J. Obes. Relat. Metab. Disord. 18, 79–83 (1994).
Dju, M. Y., Mason, K. E. & Filer, I. J. Jr. Vitamin E (tocopherol) in human tissue from birth to old age. Am. J. Clin. Nutr. 6, 50–60 (1958).
Ponrartana, S. et al. Brown adipose tissue in the buccal fat pad during infancy. PLoS ONE 9, e89533 (2014).
Author information
Authors and Affiliations
Contributions
T.A. conceived the idea, interpreted the findings, and drafted the initial manuscript. R.S.T. and J.P.L. interpreted the findings, provided critical feedback, as well as edits and revisions to the manuscript. All authors approved the final version of this manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Abe, T., Thiebaud, R.S. & Loenneke, J.P. The mysterious values of adipose tissue density and fat content in infants: MRI-measured body composition studies. Pediatr Res 90, 963–965 (2021). https://doi.org/10.1038/s41390-021-01376-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-021-01376-y
This article is cited by
-
SubQ-Sim: A Subcutaneous Physiologically Based Biopharmaceutics Model. Part 1: The Injection and System Parameters
Pharmaceutical Research (2023)
