
Abstract
Background
Free secretory component (free SC) in human milk is a critical constituent of secretory IgA (SIgA) for immune exclusion, but its concentration in human milk is unknown. To evaluate the relationship between free SC and SIgA, the influence of maternal factors (vaccination during pregnancy, allergy, previous infections, nutrition, mode of delivery and active lifestyle) on the concentrations of those secretory immune components in human milk was investigated.
Methods
Concentration of active free SC and SIgA in 124 milk samples from 91 mothers were measured via ELISA.
Results
Free SC in milk from Tdap-vaccinated mothers was lower than the Tdap-flu-vaccinated, flu-vaccinated or Rhogam-vaccinated mothers. Free SC in mothers who had a cesarean delivery was higher than mothers who had a vaginal delivery. Free SC in the nonallergic group was higher than the allergic group. Free SC was higher in mothers who rarely/never eat junk food, than in mothers who always/frequently eat junk food. Free SC also was higher in the moderate exercise group (active lifestyle) compared with the group who rarely/never exercise (sedentary lifestyle). Free SC in human milk was not affected by previous maternal infection or probiotic supplementation whereas SIgA was not changed by all investigated maternal factors.
Conclusion
This study suggests that active free SC is more impacted by maternal factors than active SIgA in human milk.
Impact
-
Active free secretory component (free SC) is more impacted by maternal factors than active secretory IgA (SIgA) in human milk.
-
Vaccination during pregnancy, allergy, nutrition, type of delivery and active lifestyle affect the secretion of free SC in human milk, but not SIgA secretion.
-
Free SC in human milk is a critical constituent of secretory IgA (SIgA) for immune exclusion against pathogens and its active concentration in milk strongly varies between mothers, partially due to their specific maternal background.
Similar content being viewed by others


Introduction
Secretory component (SC) is a glycoprotein attached to IgA or IgM (SC attached to IgA is denoted as secretory IgA (SIgA) and SC attached to IgM is SIgM).1 In the interstitial space of the mammary gland tissues, IgA-producing plasma cells (activated B cells) secrete immunoglobulin A (IgA), mainly in a dimeric form, which can bind to polymeric Ig receptor (pIgR)2,3 (Fig. 1a). Pentameric immunoglobulin M (IgM) produced by plasma cells can also bind to polymeric Ig receptor (pIgR). However, the external transport of IgA is preferred (6- to 12-fold) over IgM, which explains the higher amount of SIgA over SIgM in external secretions (including human milk and mucosal secretions).4 IgA binds via their Fc region to pIgR2 to form the pIgR-IgA complex and this complex can be transported in a vesicle across the mammary epithelial cell to the alveolar lumen (Fig. 1b).1 SIgA is released from the pIgR-IgA complex by proteolytic cleavage into the lumen (Fig. 1c). SC covalently linked to pIgA increases the survival of pIgA against proteolytic degradation by digestive enzymes and bacterial proteases.1,5,6 Excess of unoccupied pIgR secreted by epithelial cells is released by proteolytic cleavage in the same way as SIgA or SIgM to form “free SC” (Fig. 1d).

a In the interstitial space of the mammary gland tissues, plasma cell secretes immunoglobulin A (IgA), which can bind to the polymeric Ig receptor (pIgR). b IgA binds via their Fc region to pIgR to form the pIgR-IgA complex and this complex is transported in a vesicle across the mammary epithelial cell to the alveolar lumen. c SIgA is released from the pIgR-IgA complex by proteolytic cleavage into the alveolar lumen and then SIgA is diffused in human milk. d Excess of unoccupied pIgR secreted by mammary epithelial cells is released by proteolytic cleavage to form “free SC” in the alveolar lumen and diffuse in human milk. e The main role of SIgA and free SC in human milk is to perform immune exclusion by neutralizing pathogen agents and their toxins and block their attachment on the intestinal epithelial cells of newborns. f Free SC production in human milk could be increased by the attachment of microbial agents to SIgA on the mammary epithelial cells. g After microbial antigen recognition, T cells could produce cytokines and promote the SC production by epithelial cells.
The main role of SIgA and free SC from human milk in the neonatal gut is to perform immune exclusion by neutralizing pathogen agents and their toxins while blocking their attachment on the intestinal epithelial cells7,8 (Fig. 1e). Both free SC and SIgA can block the epithelial adhesion of enterotoxigenic Escherichia coli,9 neutralize toxin A of Clostridium difficile10 and bind to pneumococcal surface protein (SpsA).11 C. difficile toxin A was similarly inhibited by free SC and SIgA from human milk.10 SIgA can also bind to commensal bacteria (Lactobacillus rhamnosus and Bifidobacterium lactis) via SC. However, removing the glucans of SC complexed to SIgA abolished its binding capacity on commensal bacteria and its anchoring in mucus (the loss of localization in the gut reduced optimal functions of SIgA).12 SIgA and free SC can reduce biofilm formation, but SIgA treated with endoglycosidase H (to cleave the oligosaccharides from SC) abolished its capacity to decrease biofilm from Vibrio cholerae.13 These investigations suggest that free SC is a critical constituent of SIgA to perform immune exclusion and prevent the invasion of pathogens. Moreover, free SC may contribute to the maintenance of epithelial barrier integrity and mucosal homeostasis by reducing the accessibility of enteric bacteria to the lamina propria.14 Purified free SC from human colostrum also inhibits the adhesion of enteropathogenic Escherichia coli (EPEC) to epithelial cells, which suggests a protective effect of free SC against diarrhea in infants fed human milk.15 Free SC in human milk could play an essential role in the immune defenses (both innate and adaptive immunity) against infections,16,17 especially in the neonatal gut where the biosynthesis of SIgA, SIgM, and free SC is likely in a lower amount due to their immature immune system.18,19
Our previous study20 demonstrated that active SIgA and total IgA from human milk were detected in stools from preterm infants fed human milk, where most of the total IgA was IgA without the SC (99.3%). The lower proportion of SIgA compared with the total IgA in the stool was likely due to the release of the free SC during gastrointestinal proteolytic digestion.20 This higher recovery of free SC in human milk may contribute to the innate mucosal defense and prevent microbial infections. SIgA concentration (1000 μg/mL) in purified secretory components from pooled human colostrum was fivefold more than the free SC concentration (200 μg/mL).21 However, the concentration of free SC in mature milk (>3 weeks postpartum) from individual mothers and the maternal factors that influence its secretions remain unknown.
The aim of this study was to examine the influence of maternal factors on the concentrations of active free SC, SIgA and free SC/SIgA ratio in mature milk from healthy mothers. Vaccination during pregnancy, previous infection, allergy, mode of delivery, nutrition and an active lifestyle are the main maternal factors investigated to observe the change in the concentration of free SC and SIgA in human milk. Understanding their influence is critical because newborns need passive immunity from human milk secretory immune components until their immune system has matured.
Methods
Study design and participants
Raw human milk samples were from 91 healthy women, who are approved donors through Mothers Milk Cooperative (Boulder City, NV). These women are from the United States (see demographic description in Table 1). We received their consent to use their milk for research. Milk collection was approved by the institutional review board (IRB00012424) of Medolac Laboratories (A Public Benefit Corporation). The criteria pre-established for inclusion are passing blood tests (negative tests for HIV, HTLV, hepatitis B or C and syphilis), living in the USA, completing a health questionnaire, and no use of specific medications. Mothers, who were smokers, drug users or diagnosed with a systemic infection or other diseases (including obesity and human immunodeficiency virus) were excluded. Among the participant pool, 21 filled out a survey on their weekly nutrition and physical exercises, which specified whether they are ingesting probiotics (Greek yogurt, kombucha, capsules or no probiotic), eating junk food, having a healthy diet, or eating a specific diet (vegetarian, gluten-free or dairy-free).
Milk collection
Milk samples (150–250 mL) were collected 1–4 times at home with clean electric breast pumps into sterile plastic containers and stored immediately at −20 °C in deep freezers. The breast was cleaned with a wet washcloth (no soap or alcohol) before pumping. Milk samples were frozen and transported in insulated boxes to Medolac Laboratories (A Public Benefit Corporation), where they were kept frozen and stored at −30 °C in an industrial freezer until the ELISA measurements.
Free SC and SIgA concentrations
The concentration of free SC and SIgA was determined using ELISAs that was adapted from our previous publications.20,22 ELISAs were recorded with a microplate reader (SpectraMax iD5, Molecular Devices, Sunnyvale, CA, USA). Raw human milk samples (n = 124) were rapidly thawed at 37 °C in a water bath and centrifuged at 1301 × g for 20 min at 4 °C. After removing the fat layer with cotton swabs, the supernatant was collected, separated into aliquots and stored at −20 °C until analyzed. Clear flat-bottom microplates (Nunc MaxiSorp, Thermo Fisher Scientific, Rochester, NY) were coated with 100 μL of capture antibodies at 1 μg/mL in 1× phosphate-buffered saline pH 7.4 (PBS, Gibco, Grand Island, NY, USA): rabbit anti-human SC (Exalpha Biologicals Inc, Shirley, MA, USA) for free SC and rabbit anti-human IgA (α-chain specific) IgG for SIgA. Standard samples were prepared using purified SC without immunoglobulin from human milk (Exalpha biologicals Inc) and purified SIgA from human colostrum (Sigma-Aldrich, St. Louis, MO, USA). These standards were prepared using dilution series in the blocking buffer and the final concentration covered a range from 1 to 2000 ng/mL for free SC and from 5 to 5000 ng/mL for SIgA. Free SC control (250 ng/mL of purified SC without immunoglobulin was added in blocking buffer) and SIgA control (250 ng/mL of purified SIgA was added in blocking buffer) were also measured in four independent experiments to compare the detection of free SC and SIgA for both ELISAs. Supernatant samples were diluted 2000× for free SC and SIgA with a blocking buffer. For free SC, goat anti-human SC to horseradish peroxidase (HRP) was used (Exalpha biologicals Inc). For SIgA, mouse anti-human IgA secretory-chain IgM was added, the plate was incubated 1 h, washed, and then goat anti-mouse IgG conjugated to HRP was added (Sigma-Aldrich).
Statistical analyses
Concentration of free SC and SIgA and free SC/SIgA ratio (calculated for each specific mother’s milk) in human milk samples were compared between the following characteristics using unpaired t tests in GraphPad Prism software (version 8): vaccination during pregnancy (flu/influenza vaccine, tetanus, diphtheria and acellular pertussis (Tdap) vaccine, both flu and Tdap vaccines, Rhogam vaccine, no vaccine); infant gender (female and male); prematurity (preterm-delivery and term-delivery); postpartum time for preterm-delivery (6–9 and 10–14 months); postpartum time for term-delivery (7–9, 4–5, 10–13 and 15–17 months); previous infection during the last year for mothers (infection or no infection); infection during last year for infants; supplemented in prenatal vitamins (vitamins or no vitamins); mode of delivery (cesarean or vaginal); allergy in mothers (allergy or no allergy); daily ingestion of probiotics in mothers (probiotics or no probiotic), eating junk food in mothers (0–2 times per month or 1–4 time per week), physical exercises in mothers (moderate cardio 3–6 times per week or mild cardio/walking 0–2 times per week) and specific diets in mothers (gluten, dairy or meat-free/restriction vs. eat all groups of food/no restriction). Differences were designated significant at p < 0.05. Linear regression was used to determine a correlation between free SC and SIgA concentrations. The sample size (n = 124 milk samples and N = 91 mothers) was selected based on the previous literature sample sizes and proved adequately powered based on the results.20,22,23
Results
Mother demographic and characteristic
The demographic and characteristic details for the donors are presented in Table 1.
Vaccination during pregnancy
Free SC concentration in milk from mothers who received a flu vaccine during pregnancy was 3.1-fold higher than those with Tdap vaccine (p = 0.020, Fig. 2a), but did not differ with nonvaccinated mothers and mothers vaccinated with both flu and Tdap or mothers vaccinated with Rhogam. Free SC in milk from mothers vaccinated with Tdap was 2.1- and 3.1-fold lower than mothers who were vaccinated with both flu and Tdap (p = 0.042) or Rhogam (p = 0.007), respectively, but did not differ from the nonvaccinated mothers. Free SC in milk from the Rhogam vaccine group was 1.5-fold higher than the flu and Tdap vaccine group (p = 0.088). Free SC concentration in milk from nonvaccinated women did not differ from all of the vaccinated women or vaccine-specific groups (Supplementary Table S1). Free SC/SIgA ratio in milk from mothers vaccinated with Tdap was 3.1-fold lower than mothers vaccinated with both flu and Tdap (p = 0.035, Fig. 2b), but other groups did not differ. SIgA did not differ between vaccines and no vaccine groups.

Effect of vaccination during pregnancy on the concentration of a free secretory component (free SC) and b free SC/secretory IgA (SIgA) ratio in human milk. Milk from mothers vaccinated with flu (Flu, n = 26, N = 20), mothers vaccinated with tetanus-reduced-dose diphtheria and acellular pertussis (Tdap, n = 11, N = 8), milk from mothers vaccinated with both flu and Tdap (Flu + Tdap, n = 36, N = 26), milk from mothers vaccinated with Rhogam (n = 6, N = 4) and nonvaccinated mothers (no vaccine, n = 45, N = 33). Values are mean ± SEM for milk samples (n) in each group (N represents the number of women). Asterisks show significant differences between variables (**p < 0.01; *p < 0.05) using unpaired t tests.
Allergy
Free SC concentration in milk from allergic mothers was 2.2-lower than nonallergic mothers (p = 0.009, Fig. 3a). SIgA concentration and free SC/SIgA ratio in milk did not differ between mothers with allergy and mothers without allergy (Supplementary Table S1).

a Effect of allergy in mothers on the concentration of free secretory component (free SC) in human milk. b Effect of infection in mothers on free SC/SIgA ratio in human milk. c Effect of cesarean and vaginal birth (mode of delivery) on the concentration of free SC in human milk. d Effect of ingestion of probiotics in mothers on free SC/SIgA ratio in human milk. Values are mean ± SEM for milk samples (n) in each following groups (N represents the number of women): a allergy (n = 12, N = 6) and no allergy (n = 112, N = 85); b infection (n = 25, N = 17) and no infection (n = 99, N = 74); c cesarean (n = 6, N = 5) and vaginal birth (n = 118, N = 86); and probiotics (n = 29, N = 15) and no probiotic (n = 10, N = 6). b Mothers had infection(s) in the last year, but they were not infected during the sample collection. The type of infection was mastitis (n = 9, N = 6), flu/respiratory infection (n = 6, N = 4), bacterial infection/diarrhea (n = 4, N = 3) and yeast infection (n = 6, N = 4). d Mothers supplemented daily with probiotics during the milk collection by eating Greek yogurt and/or kombucha (n = 22, N = 11) or probiotic capsule (n = 7, N = 4). Asterisks show significant differences between variables (**p < 0.01; *p < 0.05) using unpaired t tests.
Infection
The free SC/SIgA ratio in milk from mothers that had at least one infection during the last year (but not during the milk collection) was 2.2-fold higher than mothers who had no infection in the last year (p = 0.030, Fig. 3b), but did not differ for free SC and SIgA concentrations (Supplementary Table S1). Moreover, free SC, SIgA and free SC/SIgA ratio in human milk did not differ between infants that had infection during the last year and infants who did not have infection during the last year (Supplementary Table S1).
Mode of delivery
Free SC concentration in milk from mothers who delivered via cesarean was 2.6-fold higher than mothers who delivered their infant vaginally (p = 0.006, Fig. 3c). Free SC/SIgA ratio in milk from women who delivered via cesarean was higher (3.1-fold, p = 0.067) than women who delivered vaginally. SIgA concentration did not differ between mothers with a cesarean delivery and those with a vaginal delivery (Supplementary Table S1).
Ingestion of probiotics
Free SC/SIgA ratio in milk from mothers ingesting daily probiotics (via Greek yogurt, kombucha and/or capsule) was 2.3-fold lower than mothers who did not take probiotics (p = 0.008, Fig. 3d). SIgA and free SC concentrations did not differ between mothers ingesting probiotics and those who do not consume probiotics (Supplementary Table S1).
Frequency of eating junk food or a healthy diet
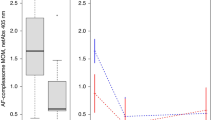
Free SC concentration and free SC/SIgA ratio in milk from mothers who rarely/never eat junk food (0–2 times per month) and daily healthy diet was 2.5- and 3.1-fold, respectively, higher than mothers who always/frequently eat junk food (1–4 times per week) (p = 0.003, Fig. 4a, b), but did not differ for SIgA concentration (Supplementary Tables S2 and S3).

Effect of time per week for eating junk food in mothers on a the concentration of secretory component (free SC) and b the free SC/SIgA ratio in human milk. Effect of physical exercises on c the concentration of secretory component (free SC) and d the free SC/SIgA ratio in human milk. Values are mean ± SEM for milk samples (n) in each following group (N represents the number of women): junk food, 1–4 times per week (n = 16, N = 11) and 0–2 times per month (daily healthy diet) (n = 20, N = 9); moderate exercise (active lifestyle), 3–6 times per week/moderate (n = 26, N = 13) and milk exercise (sedentary lifestyle), 0–2 times per week (n = 8, N = 5). Asterisks show significant differences between variables (**p < 0.01; *p < 0.05) using unpaired t tests.
Physical exercises
Free SC concentration (p = 0.037, Fig. 4c) and free SC/SIgA ratio (p = 0.021, Fig. 4d) in milk from mothers doing moderate exercises (active lifestyle, 3–6 times per week) was 2.5- and 4.5-fold higher than mothers doing mild exercises (sedentary lifestyle, 0–2 times per week). SIgA concentration in milk from women who do moderate exercises was higher than those who do mild/no exercises (p = 0.070, Supplementary Tables S2 and S3).
Other maternal factors
Free SC, SIgA and free SC/SIgA ratio in milk did not differ between preterm-delivering mothers and term-delivering mothers, infant gender (male vs. female), specific diets (vegetarian free and/or gluten-free dairy-free vs. no restriction) and supplemented in prenatal vitamins (Supplementary Table S2). SIgA concentration in milk from term-delivering mothers lactating at 7–9 months postpartum was 1.9-fold higher than those lactating at 10–13 months postpartum (p = 0.024, Supplementary Table S2). SIgA concentration in milk from preterm-delivering mothers lactating at 6–9 months postpartum was higher than those lactating at 10–14 months postpartum (p = 0.092, Supplementary Table S2). Free SC and free SC/SIgA ratio in milk did not differ between postpartum time for preterm- and term-delivering mothers.
Free SC ELISA detected 254 ± 15 ng/mL for control with 250 ng/mL of purified free SC from human milk whereas 10 ± 1 ng/mL for control with 250 ng/mL of purified SIgA from human colostrum. The specificity of free SC ELISA for free SC was 25.7-fold higher than for SIgA (p < 0.001, Fig. 5a). SIgA ELISA detected 52 ± 6 ng/mL for control with 250 ng/mL of purified free SC whereas 240 ± 5 ng/mL for control with 250 ng/mL of purified SIgA. The specificity of SIgA ELISA for SIgA was 4.6-fold higher than for free SC (p < 0.001, Fig. 5b). Therefore, free SC ELISA was specific to active/native free SC whereas SIgA ELISA was specific to active/native SIgA.

Concentration of free SC in blocking buffer with 250 ng/mL of purified secretory IgA (SIgA250) and in blocking buffer with 250 ng/mL of free secretory component (free SC 250) using (a) free SC ELISA and b SIgA ELISA. Values are mean ± SD, n = 4. Asterisks show significant differences between variables (***p < 0.001) using unpaired t tests.
Active free SC concentration was not correlated with active SIgA concentration in human milk (p = 0.29, slope = −0.082 ± 0.08).
Discussion
Although the effects of prematurity (preterm- and term-delivery), postpartum/lactation time (colostrum, transitional milk and mature milk) and maternal infections on SIgA concentration in human milk have been well-characterized,20,23,24,25,26 the influence of maternal factors on the free SC concentration in human milk remains unexplored. The present study is the first to investigate the influence of vaccination during pregnancy, mode of delivery, maternal allergy, previous infections in women and infants, nutrition (probiotics, junk food/healthy food, and specific diets), physical exercises (active lifestyle) and other maternal factors (prenatal vitamins, prematurity and postpartum time) on the concentration of active free SC and SIgA and free SC/SIgA ratio in human milk. These preliminary data are important for understanding the secretion of secretory components in human milk that can protect the infant against infection.
Overall concentrations of free SC and SIgA were similar in human milk (783 and 748 μg/mL, respectively) when all maternal factors were combined. Dallas and Rolfe21 reported that SIgA concentration (1000 μg/mL) in purified secretory components from pooled human colostrum was fivefold more than free SC concentration (200 μg/mL). This difference is likely related to the early lactation (colostrum) and the purification process compared with raw mature human milk in this study.21
Free SC concentration in milk from mothers vaccinated with Tdap was lower than in milk from mothers with both Tdap and flu vaccines, flu vaccine or Rhogam vaccine, but did not differ between nonvaccinated women and vaccinated women (all together or separated). SIgA in human milk was not affected by the vaccination during pregnancy, but the free SC/SIgA ratio was higher in mothers with both flu and Tdap vaccines compared to Tdap vaccine only. These observations could be due to the late time of vaccination in Tdap group and/or the natural antibodies present in the mother’s milk due to the previous exposition to microbial infection.27 The interactions between immune and vaccine components are still not well understood. The interactions could either improve or suppress the immune response in individual mothers depending on the antigen capture and lymphocyte recognition and responses.28 These differences between vaccine groups could also be related to a higher percentage of women supplemented with prenatal vitamins in the flu group (78.6%), both flu and Tdap group (70.2%) and Rhogam group (100%) compared to the Tdap group (54.5%). Siddiqua et al.29 reported that vitamin B12 supplementation during pregnancy increased influenza A (H1N1)-specific IgA responses in plasma and in colostrum from mothers compared to nonsupplemented mothers. Vitamin D may enhance the immune response of the vaccine due to the expression of its receptor on most of the immune cells.30 After vaccination in young adults, levels of hepatitis B-specific antibodies in group supplemented with vitamin D were higher than those nonsupplemented.31
For the first time, we demonstrated that the free SC/SIgA ratio in milk from mothers that had infections during the last year (but were not infected during the milk collection) was higher than in milk from mothers without infection. This result could be related to a higher secretion of free SC compared with SIgA by epithelial cells when mothers have an infection. The production of free SC in human milk could be induced by the attachment of microbial agents to SIgA on the mammary epithelial cells (Fig. 1f).1 However, concentrations of free SC and SIgA did not differ between the noninfection group and the infection group. In accordance with this observation, Hassiotou et al.26 observed no difference for SIgA concentration (but higher leukocytes contents) in milk from mothers with infection (breast-related and/or cold) compared to those without infection. Among leukocytes, T cells could produce cytokines after microbial antigen recognition and activate the immune responses. The release of cytokines during microbial infection could also promote the SC production by epithelial cells (Fig. 1g).
Free SC concentration in milk from mothers who delivered via cesarean was higher than mothers who delivered their infant vaginally. A previous study found that milk from mothers who had a cesarean-section had higher total bacteria concentration and lower counts of Bifidobacterium subspecies than mothers who delivered vaginally.32 The maternal microbiota induced by cesarean-section could increase the production of free SC by mammary epithelial cells. More studies are required to evaluate the interactions between maternal microbiota, mode of delivery and free SC in human milk.
Free SC/SIgA ratio in milk from women supplemented in probiotics (Greek yogurt, kombucha and/or capsules) was lower than women nonsupplemented in probiotics. This lower ratio could be due to the higher binding of free SC on probiotic bacteria in human milk. N-branched glycans on free SC are the main components responsible for specific binding to Gram-positive bacteria.12 Perez et al.33 have suggested that mothers transfer their intestinal microbiota in their milk via an entero-mammary pathway mediated by the immune system (commensal bacterial may be captured by dendritic cells and transported in the tight junctions of the intestinal epithelium to the mammary gland).34 SIgA concentration in milk was not significantly affected by the ingestion of probiotics, but SIgA was twofold higher in the probiotic group compared with the nonprobiotic group. Depending of the maternal immune system, short-chain fatty acids produced by probiotic bacteria could induce the production of SIgA in the intestine,35,36 and this excess of SIgA could be secreted in human milk. Baldassarre et al.37 reported that SIgA concentration in milk from the probiotic-supplemented mothers was higher than the nonsupplemented mothers, whereas no significant difference was observed by Quin et al.38 The effects of the daily ingestion of probiotics (at least one billion of probiotics per day) on the secretion of free SC and SIgA in human milk was investigated in this study, but not the dose and probiotic strains. Greek yogurt, kombucha, capsules or other types of probiotics usually contain a large diversity of probiotic strains, which may help to improve gut immunity compared with the ingestion of single-probiotic strain or no probiotic.
Free SC concentration in milk from the nonallergic group was higher than the allergic group, but SIgA concentration and free SC/SIgA ratio were not affected by maternal allergy. In agreement with our results, Kuitunen et al.39 found that total IgA concentration did not differ in mature milk between nonallergic and allergic mothers. Higher concentrations of anti-inflammatory interleukin (IL)-10 and transforming growth factor (TGF)-β (and lower IgE concentration) were observed in milk from the nonallergic mothers compared to the mothers with allergy.40 We speculate that cytokines IL-10 and TGF-β could promote the production of free SC by epithelial cells in human milk. Future studies are required to investigate the effect of IL-10 and TGF-β on the secretion of free SC in human milk and the impact of their interaction to reduce the risk of allergy in infants and children.
Free SC concentration and the free SC/SIgA ratio in human milk were higher in mothers who rarely/never eat junk food (frequently having a healthy diet) than in mothers who always/frequently eat junk food. Free SC and the free SC/SIgA ratio were also higher in milk from mothers doing moderate physical exercises 3–6 times per week (daily physical activity was between 30 and 90 min) compared to mothers rarely/never exercise (sedentary lifestyle). Daily healthy diet in mothers with an active lifestyle (62%) was higher compared to mothers characterized by a sedentary lifestyle (38%). Therefore, the combination of active lifestyle and a healthy diet may increase the secretion of free SC in human milk, but not the SIgA secretion. In agreement with our study, Lovelady et al.41 also reported that SIgA, lactoferrin and lysozyme in human milk were not affected by cardiovascular fitness levels (30 min/day for 3 days/week vs. exercised once a week or less for 6 weeks). The effect of physical exercises on the immune components could vary on the degree of maternal fitness and intensity, the duration of exercise and the nutrition before, during and after the exercise. These factors (including the daily caloric intake of junk food or healthy food) were not investigated in this study. As moderate cardiovascular activities and healthy nutrition are well-known to be associated with the reduction of illness and health diseases, mothers who have an active lifestyle and a healthy diet can possibly stimulate the production of free SC to prevent illness in their infant. More studies are needed to evaluate these possibilities and mechanisms.
A limitation of this study is the small sample size for some maternal factors, especially for mothers vaccinated with Rhogam vaccine or Tdap vaccine, women with allergy, women nonsupplemented with probiotics, junk food diet vs. healthy diet and moderate vs. mild physical exercise groups. The data presented are preliminary and need to be replicated with a larger size sample in a longitudinal design (analysis of multiple variables) in order to evaluate the potential interactions between the maternal factors. We did not measure the anti-inflammatory cytokines (TGF-β and IL-10) and IgE in human milk to understand the influence of maternal allergy on free SC. The measurements of these cytokines are important for future works to determine their potential influence on secretory components.
Conclusion
This study demonstrated that active free SC concentration is more affected by maternal factors (vaccination during pregnancy, allergy, mode of delivery, healthy diet and active lifestyle) than active SIgA concentration in human milk. Free SC in human milk is a critical constituent of SIgA for the immune exclusion against pathogens and its active concentration in milk strongly varies between mothers partially due to their specific maternal background. Future studies are needed to evaluate the beneficial effects of free SC in human milk for the prevention of neonatal infections.
References
Isobe, Y., Chen, S. T., Nakane, P. K. & Brown, W. R. Studies on translocation of immunoglobulins across intestinal epithelium. Acta Histochem. Cytoch. 10, 161–171 (1977).
Weicker, J. & Underdown, B. J. A study of the association of human secretory component with IgA and IgM proteins. J. Immunol. 114, 1337–1344 (1975).
Watson, D. Immunological functions of the mammary gland and its secretion-comparative review. Aust. J. Biol. Sci. 33, 403–422 (1980).
Brandtzaeg, P. et al. The B‐cell system of human mucosae and exocrine glands. Immunol. Rev. 171, 45–87 (1999).
Lindh, E. Increased resistance of immunoglobulin A dimers to proteolytic degradation after binding of secretory component. J. Immunol. 114, 284–286 (1975).
Berdoz, J., Blanc, C. T., Reinhardt, M., Kraehenbuhl, J. P. & Corthésy, B. In vitro comparison of the antigen-binding and stability properties of the various molecular forms of IgA antibodies assembled and produced in CHO cells. Proc. Natl. Acad. Sci. USA 96, 3029–3034 (1999).
Dickinson, E. C. et al. Immunoglobulin A supplementation abrogates bacterial translocation and preserves the architecture of the intestinal epithelium. Surgery 124, 284–290 (1998).
Mazanec, M. B., Nedrud, J. G., Kaetzel, C. S. & Lamm, M. E. A three-tiered view of the role of IgA in mucosal defense. Immunol. Today 14, 430–435 (1993).
Giugliano, L. G., Ribeiro, S. T. G., Vainstein, M. H. & Ulhoa, C. J. Free secretory component and lactoferrin of human milk inhibit the adhesion of enterotoxigenic Escherichia coli. J. Med. Microbiol. 42, 3–9 (1995).
Dallas, S. D. & Rolfe, R. D. Binding of Clostridium difficile toxin A to human milk secretory component. J. Med. Microbiol. 47, 879–888 (1998).
Hammerschmidt, S., Talay, S. R., Brandtzaeg, P. & Chhatwal, G. S. SpsA, a novel pneumococcal surface protein with specific binding to secretory immunoglobulin A and secretory component. Mol. Microbiol. 25, 1113–1124 (1997).
Mathias, A. & Corthésy, B. Recognition of gram-positive intestinal bacteria by hybridoma-and colostrum-derived secretory immunoglobulin A is mediated by carbohydrates. J. Biol. Chem. 286, 17239–17247 (2011).
Murthy, A. K. et al. Mannose-containing oligosaccharides of non-specific human secretory immunoglobulin A mediate inhibition of Vibrio cholerae biofilm formation. PLoS ONE 6, e16847 (2011).
Murthy, A. K., Dubose, C. N., Banas, J. A., Coalson, J. J. & Arulanandam, B. P. Contribution of polymeric immunoglobulin receptor to regulation of intestinal inflammation in dextran sulfate sodium‐induced colitis. J. Gastroenterol. Hepatol. 21, 1372–1380 (2006).
De Araujo, A. N. & Giugliano, L. G. Lactoferrin and free secretory component of human milk inhibit the adhesion of enteropathogenic Escherichia coli to HeLa cells. BMC Microbiol. 1, 25 (2001).
Perrier, C., Sprenger, N. & Corthésy, B. Glycans on secretory component participate in innate protection against mucosal pathogens. J. Biol. Chem. 281, 14280–14287 (2006).
Royle, L. et al. Secretory IgA N-and O-glycans provide a link between the innate and adaptive immune systems. J. Biol. Chem. 278, 20140–20153 (2003).
Rognum, T. O., Thrane, P. S., Stoltenberg, L., Vege, Å. & Brandtzaeg, P. Development of intestinal mucosal immunity in fetal life and the first postnatal months. Pediatr. Res. 32, 145–148 (1992).
Jain, N. & Walker, W. A. Diet and host-microbial crosstalk in postnatal intestinal immune homeostasis. Nat. Rev. Gastroenterol. Hepatol. 12, 14–25 (2014).
Demers-Mathieu, V. et al. Differences in maternal immunoglobulins within mother’s own breast milk and donor breast milk and across digestion in preterm infants. Nutrients 11, 920 (2019).
Dallas, S. & Rolfe, R. Binding of Clostridium difficile toxin A to human milk secretory component. J. Med. Microbiol. 47, 879–888 (1998).
Demers-Mathieu, V. et al. Antenatal influenza A-specific IgA, IgM, and IgG antibodies in mother’s own breast milk and donor breast milk, and gastric contents and stools from preterm infants. Nutrients 11, 1567 (2019).
Demers-Mathieu, V., Underwood, M. A., Beverly, R. L., Nielsen, S. D. & Dallas, D. C. Comparison of human milk immunoglobulin survival during gastric digestion between preterm and term infants. Nutrients 10, 631 (2018).
Mehta, R. & Petrova, A. Biologically active breast milk proteins in association with very preterm delivery and stage of lactation. J. Perinatol. 31, 58 (2011).
Breakey, A. A., Hinde, K., Valeggia, C. R., Sinofsky, A. & Ellison, P. T. Illness in breastfeeding infants relates to concentration of lactoferrin and secretory immunoglobulin A in mother’s milk. Evol. Med. Public Health 2015, 21–31 (2015).
Hassiotou, F. et al. L. Maternal and infant infections stimulate a rapid leukocyte response in breastmilk. Clin. Transl. Immunol. 2, e3 (2013).
Raya, B. A. et al. The induction of breast milk pertussis specific antibodies following gestational tetanus–diphtheria–acellular pertussis vaccination. Vaccine 32, 5632–5637 (2014).
Insel, R. A. Potential alterations in immunogenicity by combining or simultaneously administering vaccine components. Ann. N. Y. Acad. Sci. 754, 35–48 (1995).
Siddiqua, T. J. et al. Vitamin B12 supplementation during pregnancy and postpartum improves B12 status of both mothers and infants but vaccine response in mothers only: a randomized clinical trial in Bangladesh. Eur. J. Nutr. 55, 1 (2019).
Lang, P. O. & Aspinall, R. Can we translate vitamin D immunomodulating effect on innate and adaptive immunity to vaccine response? Nutrients 7, 2044–2060 (2015).
Jafarzadeh, A. et al. The association of the vitamin D status with the persistence of anti-HBs antibody at 20 years after primary vaccination with recombinant hepatitis B vaccine in infancy. Clin. Res. Hepatol. Gastroenterol. 41, 66–74 (2017).
Khodayar-Pardo, P., Mira-Pascual, L., Collado, M. C. & Martinez-Costa, C. Impact of lactation stage, gestational age and mode of delivery on breast milk microbiota. J. Perinatol. 34, 599–605 (2014).
Perez, P. F. et al. Bacterial imprinting of the neonatal immune system: lessons from maternal cells? Pediatrics 119, e724–e732 (2007).
Donnet-Hughes, A. et al. Potential role of the intestinal microbiota of the mother in neonatal immune education. P. Nutr. Soc. 69, 407–415 (2010).
Wu, W. et al. Microbiota metabolite short-chain fatty acid acetate promotes intestinal IgA response to microbiota which is mediated by GPR43. Mucosal Immunol. 10, 946–956 (2016).
LeBlanc, J. G. et al. Beneficial effects on host energy metabolism of short-chain fatty acids and vitamins produced by commensal and probiotic bacteria. Microb. Cell Fact. 16, 1 (2019).
Baldassarre, M. et al. Administration of a multi-strain probiotic product to women in the perinatal period differentially affects the breast milk cytokine profile and may have beneficial effects on neonatal gastrointestinal functional symptoms. Nutrients 8, 677 (2016).
Quin, C. et al. Probiotic supplementation and associated infant gut microbiome and health: a cautionary retrospective clinical comparison. Sci. Rep. 8, 1–16 (2018).
Kuitunen, M., Kukkonen, A. K. & Savilahti, E. Impact of maternal allergy and use of probiotics during pregnancy on breast milk cytokines and food antibodies and development of allergy in children until 5 years. Int. Arch. Allergy Immunol. 159, 162–170 (2012).
Böttcher, M. F., Jenmalm, M. C., Garofalo, R. P. & Björkstén, B. Cytokines in breast milk from allergic and nonallergic mothers. Pediatr. Res. 47, 157 (2000).
Lovelady, C. A., Hunter, C. P. & Geigerman, C. Effect of exercise on immunologic factors in breast milk. Pediatrics 111, e148–e152 (2003).
Acknowledgements
We thank all study participants for their valuable contributions. We also want to thank Adrianne Weir and Jennifer Medo for the recruitment of mothers and the management of milk samples. The authors disclosed receipt of the financial support from Medolac Laboratories (A Public Benefit Corporation) for the conduct of the study.
Author information
Authors and Affiliations
Contributions
V.D.-M. conceptualized and designed the study, carried out the statistical analysis, drafted the manuscript, and approved the final paper as submitted. V.D.-M. has primary responsibility for the final content. G.M., C.D., and D.M.D. carried out ELISA analyses and E.M. conceptualized the study. G.M., C.D., D.M.D., and E.M. critically revised the paper and approved the final paper as submitted.
Corresponding author
Ethics declarations
Competing interests
The authors are employees of Medolac Laboratories (A Public Benefit Corporation).
Patient consent
Written consents to use their milk for research were obtained from those mothers.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Demers-Mathieu, V., Mathijssen, G., Dapra, C. et al. Active free secretory component and secretory IgA in human milk: do maternal vaccination, allergy, infection, mode of delivery, nutrition and active lifestyle change their concentrations?. Pediatr Res 89, 795–802 (2021). https://doi.org/10.1038/s41390-020-0966-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-020-0966-7
