
Abstract
Background
Malaria and iron deficiency (ID) in childhood are both associated with cognitive and behavioral dysfunction. The current standard of care for children with malaria and ID is concurrent antimalarial and iron therapy. Delaying iron therapy until inflammation subsides could increase iron absorption but also impair cognition.
Methods
In this study, Ugandan children 18 months to 5 years old with cerebral malaria (CM, n = 79), severe malarial anemia (SMA, n = 77), or community children (CC, n = 83) were enrolled and tested for ID. Children with ID were randomized to immediate vs. 28-day delayed iron therapy. Cognitive and neurobehavioral outcomes were assessed at baseline and 6 and 12 months (primary endpoint) after enrollment.
Results
All children with CM or SMA and 35 CC had ID (zinc protoporphyrin concentration ≥80 μmol/mol heme). No significant differences were seen at 12-month follow-up in overall cognitive ability, attention, associative memory, or behavioral outcomes between immediate and delayed iron treatment (mean difference (standard error of mean) ranged from −0.2 (0.39) to 0.98 (0.5), all P ≥ 0.06).
Conclusions
Children with CM or SMA and ID who received immediate vs. delayed iron therapy had similar cognitive and neurobehavioral outcomes at 12-month follow-up.
Impact
-
The optimal time to provide iron therapy in children with severe malaria is not known. The present study shows that delay of iron treatment to 28 days after the malaria episode, does not lead to worse cognitive or behavioral outcomes at 12-month follow-up.
-
The study contributes new data to the ongoing discussion of how best to treat ID in children with severe malaria.
Similar content being viewed by others


Introduction
Malaria is a major contributor to the developmental gap faced by children in sub-Saharan Africa relative to other regions.1 Prior studies by our group demonstrated that two manifestations of severe malaria (SM), cerebral malaria (CM) and severe malarial anemia (SMA), both contribute to cognitive impairment in children.2,3 In addition, we recently demonstrated that children exhibit persistent neurobehavioral problems following SM, including more anxious and depressed symptoms in children with SMA, and more somatic complaints and aggressive behavior in children with either SMA or CM.4 Iron deficiency (ID), also common in much of sub-Saharan Africa, often coexists with Plasmodium falciparum malaria,5 and has well-established consequences on cognition and child behavior.6 Young children with ID exhibit a more fearful, withdrawn affect than their iron-sufficient peers,7 and chronic ID can lead to more internalizing symptoms and problems with attention that persist into adolescence even when iron is given on diagnosis of ID.7 Additionally, ID can affect multiple cognitive functions, including motor control, memory, and attention resulting, in poorer scholastic achievement, and problem-solving skills.8
There is a complex interplay between iron status, malaria risk, and neurobehavioral development in malaria endemic areas. Studies show that iron therapy at the time of malaria treatment may lead to delayed parasite clearance and increased susceptibility to clinically significant P. falciparum malaria.9 Conversely, malaria can lead to anemia of inflammation. Levels of hepcidin and ferritin, an acute phase reactant implicated in iron metabolism, rise as a result of the inflammatory response to malaria, leading to sequestration of body iron and impaired iron absorption in the gut.10,11 Impaired iron absorption and sequestration of body iron can prevent utilization of iron for hematopoiesis and brain development.9 Studies of dietary ID7,12,13,14,15 and studies of children with SM2,4 have both shown impaired attention, internalizing, and externalizing behaviors, suggesting that dietary ID and malaria-related anemia of inflammation with reduced bioavailability of iron may act on the developing brain through similar and potentially additive pathways. Effective management of ID in SM could represent an important opportunity to limit the neurobehavioral toll of malaria. However, it is difficult to know the relative contributions of dietary ID and anemia of inflammation with reduced bioavailability of iron in a child presenting with SM, as the profound inflammation that characterizes SM alters currently available iron biomarkers.
World Health Organization (WHO) guidelines recommend starting iron and antimalarial therapies concurrently when ID (defined as anemia or an abnormal value for any iron biomarker) and malaria occur concurrently.16 However, recent studies have demonstrated that the relative timing of antimalarial and iron therapies is important and that concurrent administration may not facilitate optimal iron intake into hemoglobin (Hb). A study of Gambian children recovering from malarial anemia demonstrated that iron incorporation into Hb after iron supplementation remained significantly reduced 2 weeks after starting antimalarials, while iron incorporation in children recovering from ID anemia alone was excellent at baseline and 2 weeks later.11 In addition, a recent study of Ugandan children with malaria and anemia showed that iron incorporation into Hb was twice as great when the start of iron therapy was delayed by 4 weeks vs. given concurrently.17 Together, these findings suggest that delaying iron therapy until after parasite-induced inflammation and the resultant disruptions in iron metabolism are resolved may permit greater iron absorption and incorporation, and that 4 weeks may be the most appropriate delay. However, whether delaying iron supplementation constitutes a risk to the developing brain is unknown. We conducted a clinical trial in which children with SMA and CM who were iron deficient (as defined by elevated zinc protoporphyrin (ZPP)), and iron-deficient community children (CC), were randomized to start iron therapy either immediately or after 28 days and were assessed for malaria incidence, Hb level, and cognitive and neurobehavioral outcomes over 12 months of follow-up. In this manuscript, we describe the results of immediate vs. 28-day delayed iron therapy on general cognitive ability and neurobehavioral outcomes at the 6- and 12-month follow-up visits.
Methods
Participant enrollment, randomization, iron treatment, and follow-up
Children 18 months to 4.9 years of age with CM, SMA, or CC were enrolled at Mulago Hospital, Kampala, Uganda between June 2010 and September 2014. CM was defined as: (1) coma (Blantyre coma score ≤2); (2) P. falciparum on blood smear; and (3) no other known cause of coma. SMA was defined as the presence of P. falciparum on blood smear in children with an Hb level ≤5 g/dL.
CC 18 months to 4.9 years of age who were currently healthy with no symptoms of illness and no history of chronic illness were recruited from the extended family or household compound area of children with severe malaria. CC were enrolled to be in the same age range as children with CM or SMA, but were not matched to specific children with CM or SMA. Mean age and weight-for-age z-scores did not differ between children with CM or SMA and CC.18 Exclusion criteria for all children included (1) known chronic illness requiring medical care; (2) known developmental delay; or (3) history of coma, head trauma, hospitalization for malnutrition, or cerebral palsy.
Children with ID, defined as a ZPP level ≥80 µmol/mol heme, were randomized to receive a 3-month course of daily oral ferrous sulfate (2 mg/kg per day) either concurrently with antimalarial treatment (immediate group) or 28 days after receiving antimalarial treatment (delayed group).
Complete details on participant enrollment, randomization, study iron treatment, and follow-up are provided in our manuscript on the effect of immediate vs. delayed iron treatment in this study population on iron biomarkers, malaria incidence, and Hb levels,18 and in Supplementary Methods S1 (online). The results showed that children with SMA in the delayed compared to immediate treatment group had lower mean soluble transferrin receptor (6.1 vs. 7.8 mg/L, p = 0.03) and ZPP (83 vs. 106 µmol/mol heme, p = 0.02) after 12 months and showed a non-significant trend toward fewer episodes of severe malaria (incidence rate ratio [95% confidence interval], 0.39 [0.14, 1.12]).18
Cognitive testing
Children were assessed for general cognitive ability, sustained attention, and associative memory a week after discharge (CM or SMA) or at enrollment (CC). These assessments were repeated at 6 and 12 months after enrollment. The assessments were conducted from the cognitive testing rooms on the pediatric ward at Mulago National Referral Hospital. Assessments were carried out by neuropsychological testers with undergraduate degrees in Psychology. They were blinded to the participant’s study group and treatment arms and not involved in the randomization or clinical procedures. The Mullen Scales of Early Learning (MSEL),19 which assesses motor, visual, and language ability, were used to measure general cognitive ability. Scores from fine motor, visual reception, receptive language, and expressive language scales were summed to give the early learning composite score, a measure of general cognitive ability. Ability to sustain attention was assessed using the Early Childhood Vigilance Test (ECVT),20 where a child is asked to focus his or her gaze on cartoons screened on a computer for ~7 min; the measure of sustained attention is the percentage of time the child spends gazing at the screen. Associative memory was assessed using the Color Object Association Test (COAT),21 in which children are required to associate toys with specific color-coded boxes and scored on the total number of toys placed in the correct boxes. The MSEL, COAT, and ECVT have been successfully used to assess cognition, memory, and attention in multiple studies of children with HIV or malaria in Uganda.2,22 The tests used designed to assess children in the study’s age range and have been used and validated in a number of studies and cross-cultural settings in Uganda and sub-Saharan Africa.4,23,24,25,26
Socioemotional behavioral testing
Baseline neurobehavioral testing was performed 1-week post discharge for children with CM or SMA and at enrollment for CC. Assessments were repeated 6 and 12 months after enrollment.
Primary outcomes were age-adjusted z-scores at 12-month follow-up for: (1) internalizing, externalizing, and total behavioral problems, assessed with the parent-report preschool Child Behavioral Checklist (CBCL);27 (2) global executive function, evaluated using the parent-report Behavior Rating Inventory of Executive Functioning, Preschool edition (BRIEF-P);28 and age-adjusted scores for (3) observer-rated affect and behaviors, coded using the Behavior Rating Scales (BRS), developed by Lozoff et al.7 to capture behavioral domains associated with ID, adapted by author M.K. for use with older children,29 and assessed from videotaped cognitive testing sessions by an experienced BRS coder at the University of Minnesota. The CBCL is a parent-report tool focused on indicators of externalizing and internalizing behavior. The BRIEF is a parent-report tool focused on indicators of emotional regulation and executive functioning. Literate parents completed printed versions of the two tools themselves; illiterate parents were read all items in each tool verbatim in a language of their choosing (English or Luganda), and their verbal responses were recorded by a trained tester.
The CBCL and BRIEF have previously been adapted for use in Uganda,25 while the BRS was adapted for this study by author M.K. (details are provided in Supplementary Methods S2 [online]) and coded by an experienced coder (intra-class correlation coefficient >0.8). For the CBCL, children were scored on the syndrome scales, which are: emotionally reactive, anxious/depressed, somatic complaints, withdrawn, attention problems, aggressive behavior, and sleep problems. These were summarized into internalizing problems (emotionally reactive, anxious/depressed, somatic complaints, withdrawn), externalizing problems (attention problems, aggressive behavior), and total problems, which included both internalizing and externalizing problems, as well as two more scales, sleep problems and other problems.4,23
Secondary outcomes included 12-month follow-up sub-scale scores of the BRIEF-P and CBCL; and baseline and 6-month follow-up global executive function, internalizing behavior, externalizing behavior, total behavioral problems, and observer-rated behavior scores. For CBCL and BRIEF scores and sub-scales, higher scores indicate more problematic behavior or diminished function. For the BRS, higher raw scores on Fearful/Wary Affect, Negative Affect, and Hyperactivity/Over-activity, and lower raw scores on Positive Affect, Adaptation to Change, and Exploration and Activity Level, indicated more problematic behavior.
Statistical analysis
Age-adjusted z-scores for general cognitive and neurobehavioral outcomes were computed using the scores of CC age 18 months–4.9 years enrolled in a parallel prospective longitudinal cohort study of children with CM, SMA, or CC that did not include iron treatment.2 Scores from asymptomatic CC were used to generate age-adjusted z-scores because this provided population-specific normative values for cognitive and behavioral outcomes, as opposed to using the US-based norms given with most tests, which would be inappropriate for this population.
For each outcome, the z-score was computed as (actual score − mean score for child’s age)/standard deviation (SD), where the mean score for age and SD were computed by fitting a mixed linear model to data from all available visits for CC in the parallel study2 (allowing correlated errors for a child’s multiple visits); z-scores have a mean of 0 and SD of 1 in the reference population (CC) over all time points.
Five of seven BRS outcomes were heavily skewed and could not be converted to a z-score. These skewed scales were converted to categorical outcomes that best matched the scale distribution. For Fearful/Wary Affect, Negative Affect, Positive Affect, and Overall Hyperactivity/Over-activity, any expression was termed “present” and no expression was termed “absent.” For Overall Adaptation to Change/Cooperation, scores equal to or above the median were termed “present,” and a score below the median “absent.”
To estimate the mean age-adjusted z-score differences (I – D) at baseline and 6 and 12 months, linear regression models were fitted separately for each study group (CM, SMA, and CC). Categorical BRS outcomes, adjusted for age and sex, were compared by logistic regression. The three primary outcomes at 12 months were pre-specified and no adjustment for multiple testing was made to P values. For outcomes at baseline and 6 months, we adjusted for multiple testing using Holm’s sequential Bonferroni procedure.30 Hb at baseline and malaria incidence over the 12-month follow-up period did not differ between I and D treatment arms and so were not adjusted for in analysis. Data were analyzed using STATA version 12.1 (Stata Corp, Texas). Sample sizes of 50 CC, 80 CM, and 100 SMA, equally allocated between delayed and immediate iron treatment groups, were estimated a priori to give 89% power (α = 0.05) to detect a 1 SD difference in z-scores between the CM group with the immediate treatment strategy and other malaria-iron treatment groups
Data sharing statement
Deidentified individual participant data (with data dictionaries) will be made available upon publication to researchers who provide a methodologically sound proposal for data analysis that is consistent with the goals of the approved protocol. The study protocol, statistical analysis plan, and informed consent form will be provided with the participant data. Proposals should be submitted to Debbie Bennett, debabenn@iupui.edu.
Results
Study cohort characteristics
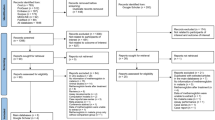
The numbers of children tested for general cognitive and neurobehavioral outcomes at each time point are shown in Supplementary Fig. S1 (online). All tests of cognition and behavior used were designed for children <5 years, so testing numbers decreased as some children became >5 years old.
Baseline demographic, clinical, and laboratory findings are summarized in the accompanying manuscript on iron biomarkers and malaria incidence and in Supplementary Table S1a for the children who received iron treatment (online). All variables, including home environment and socioeconomic status, were similar in each disease group in the I vs. D treatment arms.
Cognitive outcomes at 12-month follow-up
For the primary cognitive outcome endpoint (cognitive outcomes at 12-month follow-up), there were no statistically significant differences between children in the immediate compared to delayed treatment arm in any study group (CM, SMA, or CC) for any cognitive outcome (general cognitive ability, sustained attention, associative memory, Table 1 and Fig. 1).

Scores are shown as unadjusted means with 95% confidence intervals.
Effect sizes for differences in immediate and delayed treatment arms were small (<0.5) for all cognitive outcomes for children with severe malaria (CM or SMA, Table 1). Effect size was larger for associative memory for CC, with a mean difference (standard error of mean (SE) of 0.98 (0.50), P = 0.06), favoring immediate therapy. Overall, scores for cognitive ability were lower in children with CM or SMA were lower than CC, but the study was not designed or powered to assess statistical differences between these study groups.
Cognitive outcomes at baseline and 6-month follow-up
No significant differences between immediate and delayed iron treatment arms were seen for any cognitive z-score at baseline or 6-month follow-up testing for children with SMA, but modestly higher z-scores in general cognitive ability were seen at baseline in CC in the immediate treatment arm (mean difference (SE), +0.77 (0.33), P = 0.03) and at 6-month follow-up in children with CM in the immediate (+0.70 (0.28), P = 0.01 (Table 2 and Fig. 1).
Socioemotional behavior at 12-month follow-up
For the primary behavioral endpoint (neurobehavioral outcomes at 12-month follow-up), no significant differences in internalizing, externalizing, or total problem behaviors on the CBCL were seen for I vs. D iron therapy for any study group (Table 3, Supplementary Table S3), nor were any significant differences seen in the CBCL sub-scales (Table 4, Supplementary Table S5). Similarly, no significant differences were seen in BRIEF global executive composite (Table 3, Supplementary Table S3) or sub-scale z-scores (Table 4, Supplementary Table S5). Analyzing observed behavior, no differences were seen in the BRS outcomes between the I vs. D iron treatment arms for children in any study group (Table 5a, b).
Socioemotional behavior at baseline and 6-month follow-up
No significant differences were seen in socioemotional, executive function, or observed behavior scores between I and D treatment groups in any study group at baseline or at 6-month follow-up (Supplementary Table S2a–d [online]).
Discussion
In this randomized clinical trial of immediate vs. 28-day delayed iron therapy for children with severe malaria and ID, general cognitive and neurobehavioral outcomes were similar at 12 months in children who started iron 28 days after antimalarial treatment as compared to those who started iron at the time of antimalarial treatment. The study was powered to detect a fairly large difference in cognitive or behavioral z-scores (1 SD), so it is possible that smaller differences were present and not detected. Future studies with larger sample sizes are needed to clarify the current study findings, and the studies may also need longer follow-up time, as the effects of iron supplementation may take additional time to evaluate. Interestingly, the only large effect sizes seen for cognition (>0.5 z-score) were in the CC, with a mean difference of 0.98 (SE 0.5) for associative memory, favoring the immediate treatment arm (P = 0.06). This finding suggests that in the absence of inflammation, children with ID as defined by ZPP may do better with immediate treatment.
Iron plays a role in the regulation of dopaminergic activity where dopamine, a key neurotransmitter in the extrapyramidal system of the brain, acts as a powerful regulator of many aspects of cognitive brain function,31 and modulates externally focused and internally directed attention, concentration, motivational processes, and working memory.32 Numerous studies have demonstrated that ID is associated with an impairment in multiple cognitive domains, including general cognitive ability, executive function, recognition memory, inhibitory control, and sustained attention,7,15,33,34 and impairment in multiple areas of behavior.7,12,13,15
Detection of dietary ID during an episode of severe malaria is problematic, as virtually all measures of ID are affected by inflammation, and/or hemolysis that occurs in severe malaria. Studies of dietary ID and development have used composite measures, which often include one or more of: ZPP, mean corpuscular volume (MCV), transferrin saturation, and levels of serum ferritin, hepcidin, and soluble transferrin receptor.34 ZPP, ferritin, and hepcidin35,36 levels are strongly affected by inflammation; transferrin saturation depends on serum iron levels, which are an unreliable marker of ID; MCV lacks sensitivity; and serum transferrin receptor levels are altered by the hemolysis seen in malaria.5,37,38 Thus, there is no ideal marker for dietary ID during acute severe malaria. We chose ZPP because it is a point-of-care test for ID and because children in the Pemba study39 who had an elevated ZPP level and received iron therapy experienced fewer hospitalizations and deaths than children with elevated ZPP who did not receive iron. It is possible, however, that a biomarker that predicts subsequent mortality and morbidity risk may not be the same as one that predicts improved neurobehavioral outcomes. The elevated blood concentrations of ZPP, CRP, and ferritin at baseline among children with severe malaria suggest sequestered iron and therefore reduced iron bioavailability, with iron not going to the sites most needed (blood cells, brain).
The resolution of inflammation and consequent release of sequestered iron may be sufficient to correct disruptions in iron absorption and utilization alone, without additional iron therapy. Without a no-iron treatment arm in children with severe malaria, this study could not answer the question of whether iron therapy was required for all of these children.
However, starting supplementation earlier in life and/or more prolonged follow-up may be required to determine if delayed iron treatment has a long-term effect on cognition.
Previous studies by our group showed that delayed iron resulted in improved iron incorporation and lower hepcidin after 28 days.17,40 In the present study, we report elsewhere that children who received delayed iron treatment also had improved iron status at 12-month follow-up.18 These findings suggest that assessment of cognitive outcomes at longer follow-up (e.g., 2 years) in this population may be important to fully address the question of whether delayed iron treatment determine if delayed iron treatment has a long-term effect on cognition in children with severe malaria and reduced iron bioavailability.
In addition, prior studies of iron therapy to improve neurobehavioral outcomes in children under 2 years with dietary ID, including one that followed subjects into adolescence, have not demonstrated a clear long-term neurobehavioral benefit to iron treatment once dietary ID is established. Conversely, the dopamine signaling effects of acute, dietary ID in preschool- and school-aged children have been shown to resolve in <8 weeks with iron therapy.13,15 Thus, the benefits of iron treatment in children >2 years of age with previous dietary ID requires further study. In addition, possible benefits of acute vs. delayed iron in children with reduced iron bioavailability who are <2 years also requires further study, since children <2 years may be at the highest risk of brain injury from ID, but only a small proportion of the children enrolled in the present study were <2 years of age.
Assessment of behavior is a complex, culturally dependent process. The CBCL and BRIEF have been used and validated in numerous countries and cultural settings,41,42 including in Uganda.4,25 The BRS have been used in other countries and were adapted and piloted in Uganda prior to study implementation.7,41,42,43 Luganda-proficient neuropsychology testers were available on site for questions on verbal responses. This access was important because although some behaviors, like fear and hyperactivity, can be assessed based on facial cues and body language with relative accuracy, others, like positive affect and cooperation, may lose nuance without fluency in the language in which the observed interaction is conducted.
Even without general cognitive or neurobehavioral benefits, delayed iron therapy may have clinical and physiologic benefits for children with malaria. In our assessment of iron biomarkers in this same study, we found a significantly lower prevalence of ID based on ZPP in children with SMA in the delayed iron group at 12-month follow-up.18 Additionally, a recent study comparing immediate and delayed iron for ID in uncomplicated malaria suggested that delayed iron was associated with a lower incidence of sick child visits as compared to immediate iron.44 Given the potential benefit to iron status and the reduced infection risk associated with delayed iron therapy, the lack of harmful effects on general cognitive and neurobehavioral outcomes reported in this analysis suggests that delayed iron therapy may be a safe and potentially superior alternative to the current standard of care for children with ID and SM.
In conclusion, compared to immediate iron therapy, 28-day delayed iron therapy did not alter general cognitive or neurobehavioral outcomes at 12-month follow-up in children with SM and ZPP level defined ID. Additional studies are required to answer a number of questions raised by the present study, including how to define ID in SM, what biomarker(s) best predicts neurobehavioral outcomes in the context of ID and SM, the optimal age at which to provide iron therapy for ID, and whether inflammation-related sequestration of iron has the same effects on neurobehavioral outcomes as dietary ID. In addition, studies that overcome some of the limitations of our study, including the small sample size for children <2 years of age, and the ability to detect only relatively large differences in cognitive and behavioral outcomes (one standard deviation or greater), are also required before definitive recommendations can be made on the timing of iron treatment in severe malaria. Iron status and the timing of iron therapy in malaria remain important areas of study because of the potential risks of iron therapy in dietary iron-replete children in malaria endemic areas and because the populations at risk for malaria and iron undernutrition overlap so extensively.
References
Lu, C., Black, M. M. & Richter, L. M. Risk of poor development in young children in low-income and middle-income countries: an estimation and analysis at the global, regional, and country level. Lancet Glob. Health 4, e916–e922 (2016).
Bangirana, P. et al. Severe malarial anemia is associated with long-term neurocognitive impairment. Clin. Infect. Dis. 59, 336–344 (2014).
John, C. C. et al. Cerebral malaria in children is associated with long-term cognitive impairment. Pediatrics 122, e92–e99 (2008).
Ssenkusu, J. M. et al. Long-term behavioral problems in children with severe malaria. Pediatrics 138, e20161965 (2016).
Prentice, A. M., Ghattas, H., Doherty, C. P. & Cox, S. E. Iron metabolism and malaria. Food Nutr. Bull. 28, S524–S539 (2007).
Prentice, A. M., Verhoef, H. & Cerami, C. Iron fortification and malaria risk in children. JAMA 310, 914–915 (2013).
Lozoff, B. et al. Dose–response relationships between iron deficiency with or without anemia and infant social-emotional behavior. J. Pediatr. 152, 696–702. e693 (2008).
Lozoff, B., Jimenez, E., Hagen, J., Mollen, E. & Wolf, A. W. Poorer behavioral and developmental outcome more than 10 years after treatment for iron deficiency in infancy. Pediatrics 105, e51–e51 (2000).
Clark, M. A. et al. Host iron status and iron supplementation mediate susceptibility to erythrocytic stage Plasmodium falciparum. Nat. Commun. 5, 4446 (2014).
de Mast, Q. et al. Assessment of urinary concentrations of hepcidin provides novel insight into disturbances in iron homeostasis during malarial infection. J. Infect. Dis. 199, 253–262 (2009).
Doherty, C. P. et al. Iron incorporation and post-malaria anaemia. PLoS ONE 3, e2133 (2008).
Lozoff, B. Iron deficiency and child development. Food Nutr. Bull. 28, S560–S571 (2007).
Lozoff, B. et al. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutr. Rev. 64, S34–S43 (2006).
Lozoff, B. et al. Preschool-aged children with iron deficiency anemia show altered affect and behavior. J. Nutr. 137, 683–689 (2007).
Lozoff, B., Klein, N. K. & Prabucki, K. M. Iron-deficient anemic infants at play. J. Dev. Behav. Pediatr. 7, 152–158 (1986).
World Health Organization. Conclusions and recommendations of the WHO Consultation on prevention and control of iron deficiency in infants and young children in malaria-endemic areas. Food Nutr. Bull. 28, S621 (2007).
Cusick, S. E. et al. Delaying iron therapy until 28 days after antimalarial treatment is associated with greater iron incorporation and equivalent hematologic recovery after 56 days in children: a randomized controlled trial. J. Nutr. 146, 1769–1774 (2016).
Cusick, S. E., Opoka, R. O., Ssemata, A. S., Georgieff, M. K. & John, C. C. Delayed iron improves iron status without altering malaria risk in severe malarial anemia. Am. J. Clin. Nutr. https://doi.org/10.1093/ajcn/nqaa004 (2020).
Mullen, E. M. Mullen Scales of Early Learning (AGS, Circle Pines, 1995).
Goldman, D. Z., Shapiro, E. G. & Nelson, C. A. Measurement of vigilance in 2-year-old children. Dev. Neuropsychol. 25, 227–250 (2004).
Jordan, C. M., Johnson, A. L., Hughes, S. J. & Shapiro, E. G. The Color Object Association Test (COAT): the development of a new measure of declarative memory for 18-to 36-month-old toddlers. Child Neuropsychol. 14, 21–41 (2007).
Boivin, M. J. et al. Effect of caregiver training on the neurodevelopment of HIV-exposed uninfected children and caregiver mental health: a Ugandan cluster-randomized controlled trial. J. Dev. Behav. Pediatr. 38, 753–764 (2017).
Bangirana, P. et al. Reliability of the Luganda version of the Child Behaviour Checklist in measuring behavioural problems after cerebral malaria. J. Child Psychol. Psychiatry 3, 38 (2009).
Kariuki, S. M., Abubakar, A., Murray, E., Stein, A. & Newton, C. R. Evaluation of psychometric properties and factorial structure of the pre-school child behaviour checklist at the Kenyan Coast. J. Child. Psychol. Psychiatry 10, 1 (2016).
Familiar, I. et al. Use of the Behavior Rating Inventory of Executive Function and Child Behavior Checklist in Ugandan children with HIV or a history of severe malaria. J. Dev. Behav. Pediatr. 36, 277–284 (2015).
Bass, J. K. et al. Association of caregiver quality of care with neurocognitive outcomes in HIV-affected children aged 2–5 years in Uganda. AIDS Care 28, 76–83 (2016).
Achenbach, T. M. & Ruffle, T. M. The Child Behavior Checklist and related forms for assessing behavioral/emotional problems and competencies. Pediatr. Rev. 21, 265–271 (2000).
Gioia, G. A., Andrwes, K. & Isquith, P. K. Behavior Rating Inventory of Executive Function-Preschool Version (BRIEF-P) (Psychological Assessment Resources, Odessa, 1996).
Fuglestad, A. J. et al. Iron deficiency after arrival is associated with general cognitive and behavioral impairment in post-institutionalized children adopted from Eastern Europe. Matern. Child Health J. 17, 1080–1087 (2013).
Holm, S. A simple sequentially rejective multiple test procedure. Scand. J. Stat. 6, 65–70 (1979).
Lukowski, A. F. et al. Iron deficiency in infancy and neurocognitive functioning at 19 years: evidence of long-term deficits in executive function and recognition memory. Nutr. Neurosci. 13, 54–70 (2010).
Nieoullon, A. Dopamine and the regulation of cognition and attention. Prog. Neurobiol. 67, 53–83 (2002).
Algarín, C. et al. Iron‐deficiency anemia in infancy and poorer cognitive inhibitory control at age 10 years. DMCN 55, 453–458 (2013).
Wang, Y., Huang, L., Zhang, L., Qu, Y. & Mu, D. Iron status in attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. PLoS ONE 12, e0169145 (2017).
Falkingham, M. et al. The effects of oral iron supplementation on cognition in older children and adults: a systematic review and meta-analysis. Nutr. J. 9, 4 (2010).
Namaste, S. M. et al. Adjusting ferritin concentrations for inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 106, 359S–371S (2017).
Prentice, A. M. et al. Hepcidin is the major predictor of erythrocyte iron incorporation in anemic African children. Blood 119, 1922–1928 (2012).
Verhoef, H. et al. Serum transferrin receptor concentration indicates increased erythropoiesis in Kenyan children with asymptomatic malaria. Am. J. Clin. Nutr. 74, 767–775 (2001).
Sazawal, S. et al. Effects of routine prophylactic supplementation with iron and folic acid on admission to hospital and mortality in preschool children in a high malaria transmission setting: community-based, randomised, placebo-controlled trial. Lancet 367, 133–143 (2006).
Cusick, S. E., Opoka, R. O., Ssemata, A. S., Georgieff, M. K. & John, C. C. Comparison of iron status 28 d after provision of antimalarial treatment with iron therapy compared with antimalarial treatment alone in Ugandan children with severe malaria. Am. J. Clin. Nutr. 103, 919–925 (2016).
Corapci, F., Calatroni, A., Kaciroti, N., Jimenez, E. & Lozoff, B. Longitudinal evaluation of externalizing and internalizing behavior problems following iron deficiency in infancy. J. Pediatr. Psychol. 35, 296–305 (2009).
Lozoff, B. et al. Behavior of infants with iron‐deficiency anemia. Child Dev. 69, 24–36 (1998).
Lozoff, B. et al. Behavioral and developmental effects of preventing iron-deficiency anemia in healthy full-term infants. Pediatrics 112, 846–854 (2003).
Jaramillo, E. G. et al. Delaying the start of iron until 28 days after antimalarial treatment is associated with lower incidence of subsequent illness in children with malaria and iron deficiency. PLoS ONE 12, e0183977 (2017).
Acknowledgements
We thank the study participants, their families, and the study team, including clinical officers, nurses, laboratory technologists, and data entry personnel. This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) (grant number 3U01HD064698) and the Fogarty International Center (grant number D43 NS078280).
Author information
Authors and Affiliations
Contributions
A.S.S. was responsible for IRB application, conduct of the study and data collection, interpretation of data, and drafting the initial manuscript. M.H. carried out the statistical analyses, interpreted the data, and drafted the initial manuscript. P.B. directed the conduct of the study, interpreted the data, reviewed and revised the manuscript, and approved the final manuscript as submitted. A.S.S. carried out statistical analyses and interpretation of data. S.E.C. conceptualized and designed the study, was responsible for IRB application, conduct of the study and data collection, statistical analyses, and interpretation of data. R.O.O. directed the conduct of the study and interpreted the data. M.K. and M.K.G. helped to conceptualize and design the study, and interpreted the data. C.C.J. conceptualized and designed the study, directed the conduct of the study, and interpreted the data. All authors contributed significantly to the intellectual design, provided critical revisions to the manuscript, and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Informed consent
Written informed consent was required from the study participant’s legal guardian for participation in this study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Ssemata, A.S., Hickson, M., Ssenkusu, J.M. et al. Delayed iron does not alter cognition or behavior among children with severe malaria and iron deficiency. Pediatr Res 88, 429–437 (2020). https://doi.org/10.1038/s41390-020-0957-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-020-0957-8

{kind=link}