
Abstract
Patients receiving allogeneic hematopoietic cell transplantation (alloHCT) were previously shown to display a bacterial gut dysbiosis; however, limited data are available regarding the role of fungal microbiota in these patients. We evaluated the bacterial and fungal composition of the fecal microbiota at day 0 of alloHCT. Higher bacterial diversity was associated with an improved overall survival (OS) and disease-free survival (DFS). While fungal diversity had no impact on patient outcomes, we observed that high versus low relative abundance of Candida albicans in alloHCT patients at day 0 was associated with a significantly lower OS, DFS and graft-versus-host-free, relapse-free survival (GRFS) (p = 0.0008, p = 0.0064 and p = 0.026, respectively). While these results are limited by low patient numbers and low fungal read counts in some samples, they suggest a potentially important role for C albicans in alloHCT.
Similar content being viewed by others

Introduction
Allogeneic hematopoietic cell transplant (alloHCT) is an effective treatment for malignant and non-malignant hematopoietic diseases. Patients undergoing alloHCT can be concurrently exposed to cytotoxic chemotherapy, total body irradiation, immunosuppressors, and broad-spectrum antibiotics that can cause dramatic alterations of the intestinal microbiota.1 Loss of bacterial diversity at engraftment has been correlated with a worse outcome after alloHCT.2,3 In particular, high relative abundances of Enterobacterieceae and Enterococcus are associated with a decreased overall survival (OS)2,4,5 and an increased graft-versus-host disease (GVHD)-related mortality.4 In contrast, Clostridiales are associated with an improved outcome: reduced mortality for Lachnospiraceae2 and Ruminococcaeae,5 less GVHD for Blautia,6 and even decreased relapse rate for Eubacterium limosum.7
Furthermore, an association between the enteric virome and early post-transplant GVHD was recently suggested.8 Nevertheless, while fungal dysbiosis has been described in inflammatory bowel disease9 and primary sclerosing cholangitis,10 no study has addressed potential changes in the fungal gut microbiota (mycobiota) in alloHCT. Additionally, other data point to the importance of fungi on patients’ outcomes following alloHCT. Invasive fungal disease is an independent risk factor for long-term survival.11 In a mouse model of GVHD, injection of α-mannan, a major component of the fungal cell wall, or heat-killed Candida albicans exacerbated Th17-mediated GVHD.12 In humans, Candida spp. colonization at time of alloHCT has been associated with an increased incidence of grade II-IV acute GVHD.13 Finally, the interaction between bacteria and fungi within the gut and their interplay with the host and its immune system suggest that fungi may be implicated in the interaction between the microbiota and patient’s outcome after alloHCT. This study addresses this issue.
Results
This retrospective analysis included 71 adult patients who underwent alloHCT, 71 with bacterial sequencing and 70 with fungal sequencing at day 0. One patient had < than 200 bacterial sequencing reads, while 21 patients had less than <200 fungal reads per sample, leaving 70 patients with 16S samples and 49 patients with ITS2. Although the threshold of 200 reads is low, we used it to maximize the number of patients and as this threshold has previously been used in a large study.3 Patient and transplant characteristics are detailed in Table 1. Written informed consent was obtained from each patient. The study was approved by the local institutional review board.
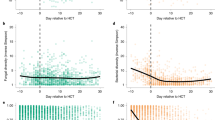
Median follow-up was 32 months (range, 2–56). We first analyzed the bacterial component and the median sequencing reads for the bacterial component were 26089 (range 628–46831). The bacterial microbiota was dominated by Enterococcus as well as numerous other pathobionts, including members of Enterobacteriaceae, Escherichia-Shigella and Klebsiella (online Supplementary Fig. S1). Furthermore, loss of beneficial members of the microbiota, particularly members of Clostridia, predicted poor outcomes (Supplementary Fig. S2A–S2C), while DFS (adjusted-p = 0.057) was higher in patients with higher alpha diversity (Supplementary Fig. S2D). These data are in accordance with the published literature, and validate the quality of our cohort and the methods used.2,3 Using ITS2 sequencing, we then assessed the composition of the mycobiota. We observed a wide variability in the detectable fungal read counts, with 3 samples undetectable following processing and the remaining ranging from 4-121249 reads per sample (median 4259.5). Excluding samples with read counts <200, we were left with 49 samples (median 56434, range 212–121249). There was no correlation between bacterial and fungal reads per sample. Using the univariate log-rank test at a false discovery rate (FDR) threshold of 0.1, we screened fungal genera for association with overall survival (Fig. 1A, B) in the 49 patients with at least 200 fungal reads per sample. Only one fungal genus, Candida, was associated with OS, with a higher than median proportion of Candida associated with lower OS (Fig. 1C). We then looked at the species level and identified that this effect was moderated by Candida albicans (Fig. 1D). Notably, the median split in the case of C albicans reduced to detectable or not detectable (25 patients had no detectable C albicans reads and 24 did). Next, we looked at performed similar analysis for DFS and GRFS. The genus Candida was again significantly predictive of poor outcome for DFS (Fig. 2A). Despite not passing the FDR significance threshold for GRFS (Fig. 2B), the species C albicans significantly predicted poorer outcomes for both DFS and GRFS (Fig. 2C-D, reporting uncorrected p values).

A Top 20 fungal microbiota OTUs and alloHCT outcomes. B FDR-corrected p values for fungal genera tested by the log-rank test for overall survival. C Kaplan–Meier curves comparing OS between Candida (genus) high and low groups (p value uncorrected). D As in C but for Candida albicans (p value uncorrected). AlloHCT allogenic haematopoietic cell transplant, FDR false discovery rate, OS overall survival, OTU operational taxonomic units.

FDR-corrected p values for the log-rank test for fungal genera and DFS (A) and GRFS (B). C Candida albicans and DFS Kaplan–Meier curves (p value uncorrected). D Candida albicans and GRFS Kaplan–Meier curves (p value uncorrected). DFS disease-free survival, FDR false discovery rate, GRFS graft-versus-host disease-free, relapse-free survival.
To further address the low number of fungal reads in a number of samples, we repeated the analysis for C albicans and OS, DFS and GRFS alone with a threshold of 10000 reads per sample (dropping the total number of samples to 34, Supplementary Fig. S3A–C). Higher proportions of C albicans remained significantly associated with OS and GRFS (p = 0.018 and p = 0.038, respectively), although not for DFS (p = 0.052). To determine if there was any overall bias in terms of fungal read count and OS, we also compared fungal read counts split on both the 200 read cut-off (Supplementary Fig. S4A), as well as the median (Supplementary Fig. S4B) and identified no significant difference. When including those samples that failed to pass the 200 read fungal threshold as a third category, these samples were between the “High” and “Low” count groups on the Kaplan–Meier curve (Supplementary Fig. S4C). Overall, this suggests that low fungal read counts were not strongly associated with OS.
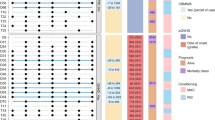
Of note, only 5 patients received antifungal treatment at the time of stool sampling. Only one of these samples fell below the threshold of 200 reads and 2 of the remaining 4 samples had detectable C albicans. To control for important clinical variables, we added the top bacterial (Lachnoclostridium genus) and top fungal (C albicans) predictors for OS to a multiple Cox proportional hazards regression in 47 subjects with both fungal and bacterial reads passing the threshold of 200 reads per sample. The clinical variables were patient’s age, conditioning regimen, donor type, graft, DRI category and initiation of broad-spectrum antibiotic before day 0 (Fig. 3). In this analysis C albicans continued to be associated with lower OS. In addition, there was no significant difference between C albicans abundance in Low/Intermediate and High/Very-high DRI category groups at commencement (p = 0.77).

DRI disease risk index, low_int low intermediate, MAC myeloablative cobditionning regimen, RIC reduced intensity conditioning regimen, BMSC/CB bone marrow/cord blood, PBSC peripheral blood stem cell, MSD matched sibling donor, HAPLO haploidentical donor, UD unrelated donor.
Discussion
In this study we report a tentative association of fecal C albicans relative abundance with worse OS, DFS and GRFS in a cohort of patients prior to alloHCT. We confirmed that expansion of potentially pathogenic bacteria and reduced ‘beneficial’ taxa was apparent, with reduced bacterial diversity associated with reduced DFS and reduction in a broad membership of Clostridia being associated with poor outcomes. This is consistent with previous findings that identify reduced bacterial diversity is a poor prognostic marker in alloHCT.2,3
Alterations of the fecal mycobiota have been reported in a number of conditions. Notably, both C albicans9 and Malassezia restricta14 have been associated with inflammatory bowel disease, while Malassezia has been associated with pancreatic cancer.15 C albicans also worsens intestinal inflammation a murine colitis model.16 Altered interkingdom correlations between bacteria and fungi are also apparent in IBD,9 with increased correlations in ulcerative colitis and decreased correlations in Crohn’s disease, suggesting an alteration in the interkingdom microbiome structure is associated with intestinal inflammation. Of note, we did not detect any correlations between bacterial and fungal taxa in this cohort.
Increased C albicans has also been associated with non-response to fecal microbiota transplantation (FMT) in treatment for recurrent Clostridioides difficile infection (CDI).17 Interestingly, increased Candida abundance pre-FMT is associated with improved response to FMT in ulcerative colitis.18 The bacterial, fungal and viral microbiome has also been evaluated in an in-depth, longitudinal study of a patient receiving multiple FMT treatments for GVHD.19 This paper identified a reduction in fungal diversity following FMT and alterations in a number of fungal species (including increases in Candida dubliniensis and Sporisorium reilianum).
Of note, none of the patients in our cohort died from C. albicans-related infection. We were not able to determine how C. albicans contributed to death or DFS events, and our study was not powered to analyze the impact on acute and chronic GVHD. Nevertheless, C. albicans has been shown to exacerbate Th17-mediated GVHD in a mouse model,12 while colonization with Candida spp. has been associated with increased risk of acute GVHD13 and C albicans has recently been shown to be the main member of the fungal mycobiome that induces antifungal Th17 response.20 In keeping with its association with IBD9 and its expansion in response to intestinal inflammation,20 C. albicans may contribute to colonic inflammation after alloHCT and GVHD. C. albicans outgrowth in alloHCT patients may be linked to bacterial microbiota dysbiosis. Interestingly, Enterobacteriaceae, which have been associated with a decreased OS after alloHCT,2 promote C. albicans colonization in the mouse gut, leading to inflammation worsening in a colitis model.21 Furthermore, increased relative abundance of Candida spp. have been reported following antibiotic treatment,22 suggesting a link between the detrimental effect of broad-spectrum antibiotics after alloHCT, gut microbiota dysbiosis and C. albicans.
Significant weaknesses in the current study are the low numbers of patients and the variability in fungal read counts. Unfortunately, due to sample limitations we were not able to re-sequence these samples. We have performed a number of steps to try and test the main conclusion of this paper and have demonstrated that C albicans is associated with OS and GRFS in samples up to read depths of 10000, even though this reduced the number of subjects to 34. However, we acknowledge that this is a significant limitation to the study and further work will be required to confirm this observation.
Overall, our study identifies C. albicans as a potentially important player in the gut mycobiota in the setting of alloHCT. Further studies are required to confirm our findings and to evaluate the mechanism of action of our observation. Finally, this raises the question of gut microbiota manipulation, such as FMT, which should aim to target not only the bacterial, but also the fungal microbiota, to correct alterations and improve patients’ outcomes after alloHCT.
Methods
Patients
This retrospective analysis included 55 consecutive adult patients who underwent alloHCT between April 2013 and December 2015 in a single institution (Saint-Antoine University Hospital, Paris, France) and who had available frozen feces collected on day 0 of the alloHCT. Patient and transplant characteristics are detailed in Table 1. Written informed consent was obtained from each patient. The study was approved by the local institutional review board.
Infection prophylaxis, monitoring, and supportive care
All received the preparative regimen as inpatients in private positive-pressure rooms, and remained hospitalized until hematopoietic and clinical recovery. Empiric broad-spectrum antibiotics were administered if a patient developed a temperature ≥38.3 °C, or ≥38 °C for 1 h, or showed any sign of infection. Antimicrobial prophylaxis consisted of acyclovir and trimethoprim-sulfamethoxazole or atovaquone, starting after neutrophil recovery, for one year, and extended if CD4+ T cells remained below 0.2 × 109/L. No antifungal prophylaxis was administered.
Stool collection and DNA extraction
Fecal samples were collected in sterile boxes, immediately homogenized, and aliquots of 0.2 g were frozen at −80 °C for further analysis. DNA was extracted from the fecal samples, as previously described.9 Briefly, following microbial lysis by both mechanical and chemical methods, nucleic acids were precipitated in isopropanol for 10 min at room temperature, incubated for 15 min on ice, and centrifuged for 30 min at 20,000 × g and 4 °C. Pellets were suspended in 450 μL of phosphate buffer and 50 μL of potassium acetate. After RNase treatment and DNA precipitation, nucleic acids were recovered via centrifugation at 20,000 × g and 4 °C for 30 min. The DNA pellet was suspended in 80 mL of trypsin-EDTA buffer. DNA samples were then subjected to 16 S and ITS2 sequencing for bacterial and fungal microbiota analyses, respectively.
16S and ITS2 DNA sequencing
Bacterial diversity in stools was determined by targeting a portion of the ribosomal genes in extracted DNA. A 16S DNA gene fragment comprising the V3 and V4 hypervariable regions (16S sense 5′-TACGGRAGGCAGCAG-3′ and antisense 5′-CTACCNGGGTATCTAAT-3′) was amplified using an optimized and standardized 16S amplicon library preparation protocol (Metabiote, GenoScreen, Lille, France). Briefly, 16S DNA PCR was performed using 5 ng of genomic DNA according to the manufacturer’s protocol (Metabiote), 192 bar-coded primers (Metabiote MiSeq Primers) at final concentrations of 0.2 μmol/L and an annealing temperature of 50 °C for 30 cycles. The PCR products were purified using an Agencourt AMPure XP-PCR purification system (Beckman Coulter, Brea, CA, USA), quantified according to the manufacturer’s protocol and multiplexed at equal concentrations. Sequencing was performed using a 250 bp paired-end sequencing protocol on an Illumina MiSeq platform (Illumina, San Diego, CA, USA) at GenoScreen, Lille, France. Raw paired-end reads were subjected to the following processes: (1) quality filtering using the PRINSEQ-lite PERL script,23 by truncating the bases from the 3′ end, that did not exhibit a quality <30, based on the Phred algorithm; and (2) searching for and removing both forward and reverse primer sequences using CutAdapt, with no mismatches allowed in the primer sequences. Sequences, for which perfect forward and reverse primers were not found, were eliminated. A similar approach was used for fungi microbiota using the primers ITS2 (sense 5′-GTGART- CATCGAATCTTT-3′ and antisense 5′-GATATGCTTAAGTTCA GCGGGT-3′) and the optimized and standardized ITS2 amplicon library preparation protocol (Metabiote, GenoScreen).
16S and ITS2 sequence analysis
The sequences were quality filtered and analyzed using the dada2 software package (version 1.14.1)24 in the R programming language (R version 3.6.3)25 for both 16S and ITS2. Dada2 outputs amplicon sequence variants (ASV’s) although for consistency with previous literature, these are referred to throughout the paper as operational taxonomic units (OTU). Taxonomic classification was performed using ilva reference database (version 138) for 16S rRNA reads and for the fungal reads, a classifier based on the UNITE ITS database (version 8.3).26,27 Bacterial and fungal OTUs that could not be assigned to a Phylum-level taxonomy were excluded. Samples were retained if they had>200 reads. Raw sequence data are accessible in the sequence read archive (SRA, accession number PRJNA746557).
Statistical analyses
Patients’ characteristics were expressed as median (range). Alpha diversity was estimated by the Shannon diversity index,which is calculated based on both number of unique OTUs and their evenness of distribution. Taxa were not filtered and samples were not rarefied prior to calculating alpha diversity. Data handling employed the phyloseq package (version 1.30.0) throughout.28
Survival analysis was performed using the survival (version 3.1-8)29 and survminer (version 0.4.8)30 packages in R. For filtering, only OTUs present in at least 10% of sampleswere included at the genus level initially and at the Species level for the genus Candida. Taxa counts were then normalized to proportion of the total count per sample. For assessment with the logrank test and Kaplan–Meier curves, diversity metrics and counts were then dichotomized to Low (</= median) or High (>median) across the whole cohort. For taxa which were undetectable in more than 50% of samples, this was equivalent to detectable (High) and undetectable (Low).
Multivariate modeling of OS was performed with the Cox proportional hazards model. The top fungal and bacterial taxa (C albicans and Lachnoclostridium, respectively) were incorporated with 6 clinical variables: (binary: broad-spectrum antibiotics at commencement or no broad-spectrum antibiotics at commencement), age (binary: ≥50 or <50), DRI category (binary: high/very high or low/intermediate), conditioning regimen (binary: RIC or MAC), cell source (categorical: BMSC/CB or PBSC) and HLA match (categorical: haplotype, MDS or UD). Three patients who could not be assigned a DRI category due to HSCT-indication (AA) were included as DRI category low/intermediate.
Plotting was performed with ggplot2 (version 3.2.2)31 and ggpubr (version 0.4.0).32 All analysis scripts are available on github (https://github.com/ajlavelle/microbiota_allogeneic_transplant).
References
Malard, F., Gasc, C., Plantamura, E. & Dore, J. High gastrointestinal microbial diversity and clinical outcome in graft-versus-host disease patients. Bone Marrow Transplant. 53, 1493–1497 (2018).
Taur, Y. et al. The effects of intestinal tract bacterial diversity on mortality following allogeneic hematopoietic stem cell transplantation. Blood 124, 1174–1182 (2014).
Peled, J. U. et al. Microbiota as Predictor of Mortality in Allogeneic Hematopoietic-Cell Transplantation. N. Engl. J. Med. 382, 822–834 (2020).
Stein-Thoeringer, C. K. et al. Lactose drives Enterococcus expansion to promote graft-versus-host disease. Science 366, 1143–1149 (2019).
Holler, E. et al. Metagenomic analysis of the stool microbiome in patients receiving allogeneic stem cell transplantation: loss of diversity is associated with use of systemic antibiotics and more pronounced in gastrointestinal graft-versus-host disease. Biol. Blood Marrow Transplant. 20, 640–645 (2014).
Jenq, R. R. et al. Intestinal blautia is associated with reduced death from graft-versus-host disease. Biol. Blood Marrow Transplant. 21, 1373–1383 (2015).
Peled, J. U. et al. Intestinal microbiota and relapse after hematopoietic-cell transplantation. J. Clin. Oncol. 35, 1650–1659 (2017).
Legoff, J. et al. The eukaryotic gut virome in hematopoietic stem cell transplantation: new clues in enteric graft-versus-host disease. Nat. Med. 23, 1080–1085 (2017).
Sokol, H. et al. Fungal microbiota dysbiosis in IBD. Gut 66, 1039–1048 (2017).
Lemoinne S., et al. Fungi participate in the dysbiosis of gut microbiota in patients with primary sclerosing cholangitis. Gut 69, 92–102(2019).
Girmenia, C. et al. Incidence and outcome of invasive fungal diseases after allogeneic stem cell transplantation: a prospective study of the Gruppo Italiano Trapianto Midollo Osseo (GITMO). Biol. Blood Marrow Transplant. 20, 872–880 (2014).
Uryu, H. et al. alpha-Mannan induces Th17-mediated pulmonary graft-versus-host disease in mice. Blood 125, 3014–3023 (2015).
van der Velden, W. J. et al. Role of the mycobiome in human acute graft-versus-host disease. Biol. Blood Marrow Transplant. 19, 329–332 (2013).
Limon, J. J. et al. Malassezia is associated with Crohn’s disease and exacerbates colitis in mouse models. Cell Host Microbe 25, 377–388.e376 (2019).
Aykut, B. et al. The fungal mycobiome promotes pancreatic oncogenesis via activation of MBL. Nature 574, 264–267 (2019).
Jawhara, S. et al. Colonization of mice by Candida albicans is promoted by chemically induced colitis and augments inflammatory responses through galectin-3. J. Infect. Dis. 197, 972–980 (2008).
Zuo, T. et al. Gut fungal dysbiosis correlates with reduced efficacy of fecal microbiota transplantation in Clostridium difficile infection. Nat. Commun. 9, 3663 (2018).
Leonardi, I. et al. Fungal trans-kingdom dynamics linked to responsiveness to fecal microbiota transplantation (FMT) therapy in ulcerative colitis. Cell Host Microbe 27, 823–829 e823 (2020).
Zhang, F. et al. Longitudinal dynamics of gut bacteriome, mycobiome and virome after fecal microbiota transplantation in graft-versus-host disease. Nat. Commun. 12, 65 (2021).
Bacher, P. et al. Human anti-fungal Th17 immunity and pathology rely on cross-reactivity against Candida albicans. Cell 176, 1340–55 e1315 (2019).
Sovran, B. et al. Enterobacteriaceae are essential for the modulation of colitis severity by fungi. Microbiome 6, 152 (2018).
Samonis, G. et al. Prospective evaluation of effects of broad-spectrum antibiotics on gastrointestinal yeast colonization of humans. Antimicrob. Agents Chemother. 37, 51–53 (1993).
Schmieder, R. & Edwards, R. Quality control and preprocessing of metagenomic datasets. Bioinformatics 27, 863–864 (2011).
Callahan, B. J. et al. DADA2: High-resolution sample inference from Illumina amplicon data. Nat. Methods 13, 581–583 (2016).
R. R Foundation for Statistical Computing, Vienna, Austria. http://www.R-project.org/. 2020.
Kessy A., et al. UNITE QIIME release for Fungi. UNITE Community. https://doi.org/10.15156/BIO/786385 (2020).
Koljalg, U. et al. Towards a unified paradigm for sequence-based identification of fungi. Mol. Ecol. 22, 5271–5277 (2013).
McMurdie, P. J. & Holmes, S. phyloseq: an R package for reproducible interactive analysis and graphics of microbiome census data. PLoS One 8, e61217 (2013).
Therneau, T. M & Grambsch, P. M. Modeling survival data: extending the Cox model (Springer, New York, 2000).
Kassambara A., Kosinski M., Biecek P. survminer: Drawing Survival Curves using ‘ggplot2’. R package version 0.4.6. 2019.
Wickham H. ggplot2: elegant graphics for data analysis.; 2009.
Kassambara A. ggpubr: ‘ggplot2’ Based Publication Ready Plots. R package version 0.2.3. 2019.
Acknowledgements
The authors acknowledge the Association for Training, Education and Research in Hematology, Immunology and Transplantation for the generous and continuous support of the research work. We are grateful to Prof. Junia V. Melo (University of Adelaide, Australia) for critical reading of this manuscript. We thank Baptiste Lamarthée for his technical assistance and our nursing staff for offering the best care to our patients.
Author information
Authors and Affiliations
Contributions
F.M. designed the study, recruited patients, performed experimental work, collected, assembled and analyzed data, and wrote and revised the manuscript. A.L. analyzed data and performed statistical analysis. G.B. and R.M. recruited patients, collected and assembled data, and helped write the manuscript. R.D., E.B., and T.L., recruited patients, collected data and helped write the manuscript. S.J. and N.R. performed experimental work. B.G., H.S. and M.M. designed the study, supervised research, analyzed data and helped with writing the manuscript.
Corresponding author
Ethics declarations
Competing interests
F.M. reports lecture honoraria from Therakos/Mallinckrodt, Janssen, Keocyte, Sanofi, JAZZ pharmaceuticals and Astellas, all outside the submitted work. H.S. received consultancy, or lecture fees from Carenity, Abbvie, Astellas, Danone, Ferring, Mayoly Spindler, MSD, Novartis, Roche, Tillots, Enterome, Maat Pharma, BiomX, Biose and Takeda, all outside the submitted work.; and is a co-founder of Exeliom bioscience. M.M. reports grants and lecture honoraria from Janssen, Sanofi, Maat Pharma and JAZZ pharmaceuticals, lecture honoraria from Celgene, Amgen, BMS, Takeda, and Pfizer, grants from Roche, all outside the submitted work. The other authors declare no competing financial interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Malard, F., Lavelle, A., Battipaglia, G. et al. Impact of gut fungal and bacterial communities on the outcome of allogeneic hematopoietic cell transplantation. Mucosal Immunol 14, 1127–1132 (2021). https://doi.org/10.1038/s41385-021-00429-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41385-021-00429-z
This article is cited by
-
Insights into gut microbiomes in stem cell transplantation by comprehensive shotgun long-read sequencing
Scientific Reports (2024)
-
Immune responses to human fungal pathogens and therapeutic prospects
Nature Reviews Immunology (2023)
-
The association of intestinal microbiota diversity and outcomes of allogeneic hematopoietic cell transplantation: a systematic review and meta-analysis
Annals of Hematology (2023)
