
Abstract
Regression in melanoma is an immunological phenomenon that results in partial or complete replacement of the tumor with variably vascular fibrous tissue, often accompanied by pigment-laden macrophages and chronic inflammation. In some cases, tumor-infiltrating lymphocytes (TILs) may represent the earliest phase of this process. The prognostic significance of regression has long been a matter of debate, with inconsistent findings reported in the literature to date. This study sought to determine whether regression in primary cutaneous melanomas predicted sentinel lymph node (SLN) status and survival outcomes in a large cohort of patients managed at a single centre. Clinical and pathological parameters for 8,693 consecutive cases were retrieved. Associations between regression and SLN status, overall survival (OS), melanoma-specific survival (MSS) and recurrence-free survival (RFS) were investigated using logistic and Cox regression. Histological evidence of regression was present in 1958 cases (22.5%). Regression was significantly associated with lower Breslow thickness, lower mitotic rate, and absence of ulceration (p < 0.0001). Multivariable analysis showed that regression in combination with TILs independently predicted a negative SLN biopsy (OR 0.33; 95% C.I. 0.20–0.52; p < 0.0001). Patients whose tumors showed both regression and TILs had the highest 10-year OS (65%, 95% C.I. 59–71%), MSS (85%, 95% C.I. 81–89%), and RFS (60%, 95% C.I. 54–66%). On multivariable analyses, the concurrent presence of regression and TILs independently predicted the lowest risk of death from melanoma (HR 0.69; 95% C.I. 0.51–0.94; p = 0.0003) as well as the lowest rate of disease recurrence (HR 0.71; 95% C.I. 0.58–0.85; p < 0.0001). However, in contrast, in the subgroup analysis of Stage III patients, the presence of regression predicted the lowest OS and RFS, with MSS showing a similar trend. Overall, these findings indicate a prognostically favorable role of regression in primary cutaneous melanoma. However, in Stage III melanoma patients, regression may be a marker of more aggressive disease.
Similar content being viewed by others

Introduction
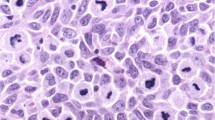
It has long been recognised that the interplay between tumor cells and the host immune system has a key role in the modification of disease progression and survival outcomes in patients with melanoma [1] and other cancer types [2, 3]. Regression in primary cutaneous melanoma is an immunological phenomenon that results in partial or complete disappearance of the tumor [4]. This process can be divided into three temporal phases, each with a distinct histological appearance (Fig. 1). The initiation of regression is heralded by tumor-infiltrating lymphocytes (TILs), which permeate the tumor and disrupt nests or directly appose tumor cells (Fig. 1A). As such, TILs represent the earliest phase of regression in many cases. In intermediate regression, there are areas of immature fibroblasts and newly formed blood vessels resembling granulation tissue (Fig. 1B). The final phase is late regression, in which tumor cells are at least partially replaced by mature fibrosis that is often associated with pigment incontinence and flattening of the overlying epidermis with loss of rete ridges (Fig. 1C). The phases of regression are not independent of each other and can co-exist to varying degrees in a single tumor.

A Tumor-infiltrating lymphocytes. B Intermediate regression. C Late regression.
Currently, Breslow thickness (BT), tumor mitotic rate and ulceration are considered the most important prognostic characteristics of a primary cutaneous melanoma, and these features are also helpful for predicting sentinel lymph node (SLN) status [5]. Recent work from our institution has shown that the presence of microsatellites and lymphovascular invasion are also associated with SLN positivity [6]. The latter, in turn, is the most powerful predictor of melanoma survival [7] and is of great importance for selecting patients who may benefit from adjuvant drug therapy and determining clinical trial eligibility [8, 9].
In contrast, the prognostic significance of histological regression in primary melanoma has been a matter of debate for decades. Whilst some studies reported an association with improved survival and a reduced likelihood of SLN positivity, others did not find any significant association, and some even reported worse outcomes in patients whose tumors showed regression. Recently, we showed that regression was a favorable prognostic factor for patients with Stage I and II cutaneous melanoma in two large cohorts from The Netherlands and Australia [10]. These findings prompted us to conduct a more detailed inquiry into the effect of various phases of regression as well as the interplay between them. In the present study, we sought to determine the impact of regression and TILs on SLN status and prognosis in a large cohort of patients treated at Melanoma Institute Australia (MIA). We also evaluated whether the extent (width) or depth of regression impacted patient outcomes. Finally, we investigated the association of regression with survival outcomes in patients whose tumor had already spread to SLNs. To our knowledge, this is the largest study of its kind undertaken to date.
Patients and methods
Data collection
The study cohort consisted of consecutive patients with primary cutaneous melanoma treated between 1 January 1999 and 31 December 2014 at MIA (a subset of this cohort, namely 4,980 Stage I and II cases treated between 1 January 2000 and 31 December 2014, formed part of the study population in a previous publication by our group [10]). For each case, clinical parameters were recorded, including age at diagnosis, sex and primary melanoma anatomic site. Investigation and treatment data included whether a SLN biopsy was performed, SLN status, any subsequent lymph node dissection, date and type of first recurrence (local, regional, in-transit or distant), date of last follow-up and status at that time. Histology slides of all primary tumors were reviewed at the time of referral by MIA-affiliated pathologists at the Department of Tissue Pathology and Diagnostic Oncology, Royal Prince Alfred Hospital, Sydney. The “reviewer” pathology reports were analyzed for this study (the original pathology slides were not re-reviewed). Documented pathological characteristics of the primary tumor included tumor subtype, BT, Clark level, presence or absence of ulceration, dermal mitotic rate (per square mm), presence or absence of microsatellites and presence or absence of a host immune response. The latter was sub-categorized as TILs (which in some cases represent early regression), intermediate regression or late regression. Where multiple phases of immune response (TILs, intermediate regression and/or late regression) were present, each was recorded. Intermediate regression was defined as areas of immature scar and angiogenesis with or without superimposed chronic inflammation. Late regression was defined as replacement of all or part of the tumor with mature dermal fibrosis, often associated with pigment-laden macrophages, flattening of epidermis and/or loss of rete ridges. In cases where residual in-situ and/or invasive tumor cells were present above or below the area of regressive fibrosis, regression was recorded as present. TILs were reported as present if lymphocytes had infiltrated the tumor to some extent, causing at least partial disruption of tumor nests, whereas a peritumoral lymphocytic infiltrate alone was considered insufficient. Cases with missing data or ambiguous findings (n = 69) were excluded. Where available, the maximal depth of regression (n = 254) and width (diameter) of regression (n = 269) were also recorded. The depth of regression was measured from the top of the granular layer to the deepest point of fibrosis, ignoring any surrounding inflammation. The diameter of regression was taken as the horizontal extent of fibrosis (or the sum of all horizontal measurements, if more than one area of fibrosis was present). Other measurements of regression extent, such as percentage of tumour replaced by fibrosis, were not available. The clinical outcome measures were SLN status, overall survival (OS), melanoma-specific survival (MSS) and recurrence-free survival (RFS). RFS was defined as time from primary melanoma diagnosis to recurrence of any kind (local, regional or distant) or death.
Statistical analysis
Clinical and histopathological features collected at the time of melanoma diagnosis were summarised using standard statistics and stratified by type of host immune response (classified as “no host response,” “regression only,” “TILs only,” or “regression and TILs”). Categorical variables were described using frequency and proportion while continuous variables were summarised using median and range. Differences between the groups were tested using either chi-square test or Wilcoxon signed rank test as appropriate. The effect of host response on SLN positivity was evaluated using univariable and multivariable logistic regression. Kaplan-Meier curves, stratified by type of host response for OS, MSS and RFS, were calculated along with the survival rates at 3-, 5- and 10-year landmark time points. Survival differences between groups were assessed using the log-rank test. Univariable and multivariable Cox regression were used to test the associations between the type of host response and OS, MSS or RFS. Survival analyses were also carried out on specific subgroups, including patients with a positive SLN biopsy and patients with intermediate vs late regression. The extent of regression was also evaluated by stratifying groups according to the regression depth (lower median versus upper median) and diameter (lower median versus upper median).
Results
The clinical and pathological characteristics of the study population are presented in Table 1, stratified by the presence of TILs and regression. The intermediate and late phases of regression were grouped together for analyses. In total 8693 patients were available for analysis. The median age was 58 years (range, 7–102) and the male to female ratio was 1.4:1. Median follow-up was 40.7 months (95% C.I., 39–43). A total of 3680 (42%) patients underwent a SLN biopsy and, of those, 697 (19%) were SLN-positive. An infiltrate of TILs was present in 5502 tumors (63.3%). Histological evidence of regression was present in 1958 cases (22.5%), comprising cases with intermediate, late or both phases of regression. The majority of tumors were located on the extremities (44% of all cases), followed by the trunk (39%).
The presence of a host immune response was significantly associated with several favorable histological parameters. Tumors showing TILs were found to have a lower median BT than tumors lacking this feature, while tumors with established regression were associated with the lowest median BT, regardless of whether or not TILs were also present (median BT of 1.8, 1.3, and 0.8 mm in tumors lacking any host response, those with TILs only, and those with regression with or without TILs, respectively; p < 0.0001). Mitotic rates were lower in tumors that had evidence of regression (46.8% of tumors with regression had a mitotic count of 0/mm2, vs 18.2% of tumors with no host response). Likewise, the finding of ulceration inversely correlated with the presence of regression, with the lowest proportion of ulcerated tumors found in the group showing both regression and TILs (10.4%, compared with 23.5% in tumors lacking any host response and 21.0% in tumors with TILs only; p < 0.0001). With regard to melanoma subtype, superficial spreading melanoma was most frequently associated with regression, with 28% of cases showing evidence of this feature, whereas only 11% of nodular melanomas showed evidence of regression, the least of any tumor subtype.
Factors impacting sentinel node positivity
Of the patients who underwent SLN biopsy (n = 3680), both regression and TILs were associated with a lower likelihood of SLN positivity, with the lowest positive biopsy rate found when both TILs and regression were present (9.9% compared with 25.5% in tumors lacking any host response, p < 0.0001).
The impact of various histological parameters on SLN status is shown in Table 2. On univariable logistic regression analysis, all combinations of TILs and regression were significantly associated with a lower rate of SLN positivity. This association held true in the multivariable model, corresponding toodds ratios (ORs) of 0.67 (95% C.I. 0.46–0.98) for regression only, 0.59 (95% C.I. 0.48–0.72) for TILs only, and 0.33 (95% C.I. 0.20–0.52) for regression in combination with TILs (p < 0.0001). Compared with superficial spreading melanoma, multivariable analysis showed a significantly increased likelihood of having a positive SLN if the primary tumor was of acral lentiginous subtype (OR 2.50; 95% C.I. 1.47–4.24; p < 0.0001), while desmoplastic melanoma showed the opposite association (OR 0.30; 95% C.I. 0.19–0.47; p < 0.0001). As expected, ulceration and higher mitotic rates were independent predictors of SLN positivity.
Factors impacting recurrence and survival
Kaplan–Meier curves of survival stratified by the presence and type of immune response are displayed in Fig. 2. Compared with patients whose tumor showed no regression or TILs, those with both features had the highest 5- and 10-year OS, MSS and RFS rates. Likewise, all types of survival at both 5 and 10 years were significantly improved in patients showing TILs alone (without concurrent regression). Patients whose tumors showed regression alone (without concurrent TILs) had improved MSS and RFS at 5 and 10 years, although no statistically significant effect on OS was seen (Supplementary Table 1).

(A), melanoma-specific survival (B), and recurrence-free survival (C) in the overall cohort.
Logistic regression analyses of OS, MSS and RFS are presented in Table 3. The presence of any pattern of immune response was associated with improvement of all outcomes in the univariable models. On multivariable analyses, the concurrent presence of regression and TILs independently predicted the lowest risk of death from melanoma (HR 0.69; 95% C.I. 0.51–0.94; p = 0.0003) as well as the lowest risk of disease recurrence (HR 0.71; 95% C.I. 0.58–0.85; p < 0.0001). The finding of regression alone showed a similar trend, but the associations did not reach statistical significance, with a HR of 0.93 (95% C.I. 0.73–1.19) for MSS and 0.89 (95% C.I. 0.76–1.04) for RFS.
Subgroup analyses did not show any significant association between regression depth (n = 254) and survival or disease recurrence (cases were stratified as having either above or below the median thickness of regression; see Supplementary Fig. 1). Similarly, analyses of regression diameter (n = 269) did not yield significant results (Supplementary Fig. 2).
Finally, we compared the relative effects of intermediate and late regression on patient outcomes (Supplementary Fig. 2). Patients selected for this analysis were stratified as having either intermediate or late regression in their primary tumor (without concurrent TILs), and compared with those who lacked any host response. Survival analyses showed no significant difference between the two phases of established regression.
Prognostic impact in stage III melanoma
Figure 3 shows the survival analyses in a subgroup of patients who had a lymph node metastases. The best outcomes were observed in patients who had TILs in their primary tumor, while the worst outcomes were seen in the patient group who had regression only. There was significant separation between the curves for OS, with corresponding 5-year survival fractions of 0.70 (95% C.I. 0.65–0.75) in the TILs group vs 0.44 (95% C.I. 0.31–0.63) in the regression-only group. Similarly, a significant difference in the 5-year RFS was observed, while the MSS curves were not significantly separated but showed the same trend.

(A), melanoma-specific survival (B), and recurrence-free survival (C) in sentinel lymph node-positive patients.
Discussion
The findings of this study demonstrate that histological regression in primary cutaneous melanoma is associated with favorable pathological features including lower BT, lower mitotic rate and lack of ulceration. Furthermore, we found that regression had a positive impact on clinical outcomes, predicting lower rates of SLN positivity and better survival compared with patients who lack this feature. Considering the individual contributions of established regression and TILs, there appeared to be an additive effect whereby the simultaneous presence of both features was independently associated with the longest MSS and RFS. Furthermore, regression independently predicted a negative SLN biopsy in our cohort, even in the absence of TILs.
The existing literature on the prognostic significance of regression shows conflicting results. Early studies reported an association between regression and worse outcomes including distant metastasis [11,12,13,14,15] and death [14, 16]. These studies were all limited to thinner melanomas (BT ≤ 1.5 mm). This led to the hypothesis that regression may be the biological phenomenon responsible for the metastatic potential of so-called “thin metastasizing melanomas”, a subset of tumors that deviated from the usually favorable prognosis of such lesions. The proposed mechanism was underestimation of the true BT. To investigate this possibility, Traves et al conducted a study of 77 melanomas showing regression, comparing the BT with the depth of regression [17]. The authors found that regression depth exceeded BT only in melanomas <0.76 mm in thickness (10/18 cases), but the difference was small and would not have caused upstaging of the tumor had the regression thickness been taken into account. Furthermore, other studies demonstrated no effect of regression on outcomes [18,19,20,21], including some that focused exclusively on thin melanomas [22, 23]. In contrast, some studies found a positive prognostic impact [24,25,26]. One of the latter was a meta-analysis that included a total of 8,557 patients, which showed that there was a lower risk of death when regression was present in the primary tumor (RR 0.77, 95% C.I. 0.61–0.97). Osella-Abate et al. [27] found that regression predicted a better RFS. In that study, regression was quantified as the ratio between the linear extension of regression and tumor. Defined in this way, a 10% cut-off was established as the minimum amount of regression required for a favorable outcome. Although MSS was not significantly affected in that cohort, an important caveat that could have confounded the outcome was that cases with more than 75% regression were excluded from analysis.
Studies investigating the effect of regression on SLN status have been equally inconsistent. Concordant with our findings, several authors have reported a decreased likelihood of a positive SLN biopsy when regression is present [19, 21, 28, 29]. Most notably, a meta-analysis of 10,098 patients showed a markedly lower risk of SLN positivity with the presence of regression in the primary tumor (OR 0.56; 95% C.I. 0.41–0.77) [30]. On the other hand, a lack of significant effect has also been reported [18, 20]. In marked contrast, Olah et al. [31] found that in patients with melanomas less than 2 mm thick, the relative risk of SLN positivity for patients with regressing tumors was 9.78 (95% C.I. 3.56–26.86) compared to patients with nonregressing tumors. Similarly, Kocsis et al. [32] showed that patients with melanomas <1 mm thick had a 5.8-fold increase in the probability of a positive SLN when regression was present. More recent work by Maurichi et al. [33] has also identified extensive regression as a risk factor for SLN positivity in thin melanomas.
The lack of consensus observed in the literature for the prognostic significance of regression may be partially explained by inconsistent histological criteria for reporting regression. A clear definition of regression was first proposed by Clark et al. in 1989, and was similar to that used in our study, except that it required a complete absence of in-situ or invasive melanoma cells in the area of regression [34]. Defined in this way, regression was found to have an unfavorable association with survival in that study by Clark et al. However, the restrictive definition may have led to a number of partially regressed melanomas being inappropriately classified as having absent regression. This viewpoint is supported by many clinical examples of melanoma in which there is clear clinical or dermatoscopic evidence of partial tumor loss and concurrent histological findings of regressive fibrosis with overlying melanoma in-situ and in some cases residual dermal invasive melanoma. Indeed, patients occasionally present with metastatic melanoma and are subsequently discovered to have melanoma in-situ with underlying dermal regression [35].
Today, the most commonly used definition of regression is complete or partial replacement of tumor cells by lymphocytic inflammation, as well as epidermal attenuation and nonlaminated dermal fibrosis accompanied by inflammatory cells, melanophages, and telangiectasia. This definition is in line with the College of American Pathologists (CAP) reporting protocol [36], which also recommends quantifying the amount of regression as less than or more than 75% of the lesion. Despite this, substantial variability persists in the literature [4]. Some studies do not specify how regression was defined, while others establish threshold values below which regression is considered absent. Additionally, interpretation of any given case is subjective, and it can sometimes be difficult to distinguish between late regression and biopsy-related scar or a non-regressive fibrous stromal response. Similarly, there is some histological overlap between TILs and the inflammatory infiltrate often observed in intermediate regression. Many authors did not control for the presence of TILs in their analyses, whereas others specifically excluded TILs as a criterion [28]. In fact, whether or not TILs equate with an early phase of regression is still a matter of debate. Kang et al [37] first described the three phases of regression, where the early phase was represented by a dense lymphocytic infiltrate admixed with nests of melanocytes. However, whilst a cytotoxic T cell-mediated antitumor response is thought to have a significant role in tumor regression, the process is complex and multifactorial. Most authors consider TILs alone insufficient for defining regression, as it is unclear whether the initiation of an immune response necessarily results in effective clearing of the tumor cells [38]. Indeed, there is evidence that different T-cell immunophenotypes predominate in regressed versus non-regressed melanomas, such that the immune cell milieu in non-regressed tumors favors immune tolerance and suppression of the antitumor response [27]. Nevertheless, lymphocytes clearly have a vital role in the initiation of regression, as underscored by the clinical efficacy of immunotherapy-based treatments.
TILs represented the commonest form of host immune response observed in our cohort (present in 63% of all cases). In tumors lacking evidence of established regression, the presence of TILs independently predicted improved OS, MSS and RFS, consistent with the hypothesis that TILs reflect effective tumor clearance by the immune system in a proportion of cases. These results are in line with previous work from our institution [39], which showed that, in melanomas > 0.75 mm in thickness, higher TIL grades correlated with better MSS. The findings of that study corroborated previous reports of a similar nature [40]. More recent work has shown that applying a simple TIL percentage scoring system allows significant separation of survival curves, with higher TIL percentages predicting better OS, RFS and MSS [41]. A recent meta-analysis of 41 studies of TILs and their role in prognostication has confirmed the favorable association with survival [42].
Our sub-group analyses of intermediate vs late regression did not show significant differences in their prognostic effects. This may be because the two phases are essentially the same process observed at different time points in its evolution. In both intermediate and late regression, there has been a loss of neoplastic cells, inciting a host response of healing and repair. In addition, as regression is a dynamic process, there is a substantial degree of overlap between the two phases, leading to difficult distinction between them in some cases.
In our study, patients whose melanoma had spread to a SLN had worse survival outcomes if their primary tumor showed evidence of regression. Considering that regression predicted improved outcomes in the overall cohort, this was an unexpected finding. Interestingly, TILs retained their favorable prognostic effect in SLN-positive patients. One possible explanation for this observation is that the corresponding primary tumors with regression in patients with SLN metastases are inherently more aggressive, and metastasize despite the presence of regression. There are two possible mechanisms at play in this scenario. The first is that nodal spread occurs before the immune response is able to clear the primary tumor. Alternatively, the primary tumor may be genetically heterogeneous, such that a proportion of cells are cleared while the less immunogenic clones escape immune attack and seed to regional lymph nodes. Only one previous study has examined the prognostic effects of regression in Stage III patients [25], with findings that contradict ours. In that cohort of patients with positive SLNs, evidence of regression in the primary tumor independently predicted a lower death rate from melanoma (sub-HR 0.34; 95% C.I. 0.12–0.92). However, the authors of that paper did not control for the presence of TILs, which may have been the reason for the observed positive association with outcome. The interactions between tumor cells, various T cell subsets, and the tumor microenvironment are the subject of ongoing research that may enhance our understanding of these processes.
The main strength of this study is the cohort size; to our knowledge, it is the largest study to date examining the prognostic implications of histological regression in melanoma. A limitation is that many of the pathology reports were issued before widespread use of synoptic report templates. For these cases, data were extracted from free text and thus subject to interpretation. A further problem is potential interobserver variability. Kang et al. [37] noted that, despite rigid criteria, interobserver agreement was suboptimal when a three-tier classification of regression was used. Grouping intermediate and late regression as one variable, as well as the single-institution study design and the power afforded by the large cohort size, should have ameliorated the impact of some of these issues. Finally, quantification of TIL density was not taken into account in this study. Whilst the effects of regression diameter and depth were analysed, no significant differences in survival were seen. It is possible that a more meaningful measure would be the relative extent of regression as a percentage of the tumor. Given mounting evidence that both TIL grade [39, 40] and percentage of fibrosis [27] may have discriminative value, there is potential for further research to address the impact of these parameters.
In conclusion, we found that the presence of histological regression in primary melanomas was associated with lower rates of SLN positivity and better survival outcomes. Of all the patterns of immune response, the combination of regression and TILs had the strongest protective effect on SLN status, MSS and RFS, even when controlling for other prognostic variables. Despite not being part of the AJCC staging system for cutaneous melanoma, the presence or absence of regression should form part of the minimal data set in melanoma synoptic report templates [43]. Furthermore, information about the regression status of the primary tumor may be useful to clinicians when deciding on optimal management strategies and should be evaluated as a parameter for possible inclusion in prognostic nomograms.
Data availability
All data generated or analysed during this study are included in this published article and its supplementary information files.
Change history
04 August 2021
A Correction to this paper has been published: https://doi.org/10.1038/s41379-021-00878-8
References
Ramirez-Montagut T, Turk MJ, Wolchok JD, Guevara-Patino JA, Houghton AN. Immunity to melanoma: Unraveling the relation of tumor immunity and autoimmunity. Oncogene. 2003;22:3180–7.
Markman JL, Shiao SL. Impact of the immune system and immunotherapy in colorectal cancer. J Gastrointest Oncol. 2015;6:208–23.
Carbone DP, Gandara DR, Antonia SJ, Zielinski C, Paz-Ares L. Non-small-cell lung cancer: Role of the immune system and potential for immunotherapy. J Thorac Oncol. 2015;10:974–84.
Aung PP, Nagarajan P, Prieto VG. Regression in primary cutaneous melanoma: Etiopathogenesis and clinical significance. Lab Investig. 2017;97:657–68.
Amin, MB AJCC Cancer Staging System, 8th Edition. Am. Jt. Commitee Cancer (2017).
Niebling MG, Haydu LE, Lo SN, Rawson RV, Lamboo LGE, Stollman JT, et al. The prognostic significance of microsatellites in cutaneous melanoma. Mod Pathol. 2020. https://doi.org/10.1038/s41379-020-0500-9.
Sharouni El, Stoddell MA, Ahmed MD, Suijkerbuijk T, Cust KPM, Witkamp AE, et al. Sentinel node biopsy in patients with melanoma improves the accuracy of staging when added to clinicopathological features of the primary tumor. Ann Oncol. 2020. https://doi.org/10.1016/j.annonc.2020.11.015.
Long GV, Hauschild A, Santinami M, Atkinson V, Mandala M, Chiarion-Sileni V, et al. Adjuvant dabrafenib plus trametinib in stage III BRAF-mutated melanoma. N Engl J Med 2017;377:1813–23.
Eggermont AMM, Blank CU, Mandala M, Long GV, Atkinson V, Dalle S, et al. Adjuvant pembrolizumab versus placebo in resected stage III melanoma. N Engl J Med. 2018;378:1789–801.
El Sharouni M, Aivazian K, Witkamp AJ, Sigurdsson V, van Gils CH, Scolyer RA, et al. Association of histologic regression with a favorable outcome in patients with stage 1 and stage 2 cutaneous melanoma. JAMA Dermatol. 2020. https://doi.org/10.1001/jamadermatol.2020.5032.
Guitart J, Lowe L, Piepkorn M, Prieto VG, Rabkin MS, Ronan SG, et al. Histological characteristics of metastasizing thin melanomas: A case-control study of 43 cases. Arch Dermatol. 2002. https://doi.org/10.1001/archderm.138.5.603.
Massi D, Franchi A, Borgognoni L, Reali UM, Santucci M. Thin cutaneous malignant melanomas (≤1.5 mm): Identification of risk factors indicative of progression. Cancer. 1999;85:1067–76.
Slingluff CL, Seigler HF. ‘Thin’ malignant melanoma: Risk factors and clinical management. Ann Plast Surg. 1992. https://doi.org/10.1097/00000637-199201000-00023.
Blessing K, McLaren KM, McLean A, Davidson P. Thin malignant melanomas (< 1.5 mm) with metastasis: a histological study and survival analysis. Histopathology. 1990. https://doi.org/10.1111/j.1365-2559.1990.tb00757.x.
Ronan SG, Eng AM, Briele HA, Shioura NN, Gupta TKDas. Thin malignant melanomas with regression and metastases. Arch Dermatol 1987;123:1326–30.
Maurichi A, Miceli R, Camerini T, Mariani L, Patuzzo R, Ruggeri R, et al. Prediction of survival in patients with thin melanoma: Results from a multi-institution study. J Clin Oncol. 2014;32:2479–85.
Traves V, Botella-Estrada R, Requena C, Nagore E. Regression does not significantly underestimate melanoma thickness. Melanoma Res. 2012;22:96–98.
Burton AL, Gilbert J, Farmer RW, Stromberg AJ, Hagendoorn L, Ross MI, et al. Regression does not predict nodal metastasis or survival in patients with cutaneous melanoma. Am Surg. 2011;77:1009–13.
Letca AF, Ungureanu L, Senila SC, Grigore LE, Pop S, Fechete O, et al. Regression and sentinel lymph node status in melanoma progression. Med Sci Monit. 2018;24:1359–65.
Tas F, Erturk K. Presence of histological regression as a prognostic factor in cutaneous melanoma patients. Melanoma Res. 2016;26:492–6.
Ribero S, Galli F, Osella-Abate S, Bertero L, Cattaneo L, Merelli B, et al. Prognostic impact of regression in patients with primary cutaneous melanoma >1 mm in thickness. J Am Acad Dermatol. 2019;80:99–105. e5
McGovern VJ, Shaw HM, Milton GW. Prognosis in patients with thin malignant melanoma: influence of regression. Histopathology. 1983;7:673–80.
McClain SE, Shada AL, Barry M, Patterson JW, Slingluff CL Jr. Outcome of sentinel lymph node biopsy and prognostic implications of regression in thin malignant melanoma. Melanoma Res. 2012;22:302–9. https://doi.org/10.1097/CMR.0b013e328353e673.
Ma MW, Medicherla RC, Qian M, Vega-Saenz de Miera E, Friedman EB, Berman RS, et al. Immune response in melanoma: An in-depth analysis of the primary tumor and corresponding sentinel lymph node. Mod Pathol 2012;25:1000–10.
Zugna D, Senetta R, Osella-Abate S, Fierro MT, Pisacane A, Zaccagna A, et al. Favourable prognostic role of histological regression in stage III positive sentinel lymph node melanoma patients. Br J Cancer. 2018;118:398–404.
Gualano MR, Osella‐Abate S, Scaioli G, Marra E, Bert F, Faure E, et al. Prognostic role of histological regression in primary cutaneous melanoma: a systematic review and meta-analysis. Br J Dermatol 2018;178:357–62.
Osella-Abate S, Conti L, Annaratone L, Senetta R, Bertero L, Licciardello M, et al. Phenotypic characterisation of immune cells associated with histological regression in cutaneous melanoma. Pathology. 2019;51:487–93.
Kaur C, Thomas RJ, Desai N, Green MA, Lovell D, Powell BW, et al. The correlation of regression in primary melanoma with sentinel lymph node status. J Clin Pathol. 2008;61:297–300.
White RL, Ayers GD, Stell VH, Ding S, Gershenwald JE, Salo JC, et al. Factors predictive of the status of sentinel lymph nodes in melanoma patients from a large multicenter database. Ann Surg Oncol. 2011;18:3593–3600.
Ribero S, Gualano MR, Osella-Abate S, Scaioli G, Bert F, Sanlorenzo M, et al. Association of histologic regression in primary melanoma with sentinel lymph node status: A systematic review and meta-analysis. JAMA Dermatol. 2015;151:1301–7.
Oláh J, Gyulai R, Korom I, Varga E, Dobozy A. Tumour regression predicts higher risk of sentinel node involvement in thin cutaneous melanomas [7]. Br J Dermatol. (2003) https://doi.org/10.1046/j.1365-2133.2003.05502.x.
Kocsis A, Karsko L, Kurgyis ZS, Besenyi ZS, Pavics L, Dosa-Racz E, et al. Is it necessary to perform sentinel lymph node biopsy in thin melanoma? A retrospective single center analysis. Pathol Oncol Res. 2019. https://doi.org/10.1007/s12253-019-00769-z
Maurichi A, Miceli R, Eriksson H, Newton-Bishop J, Nsengimana J, Chan M, et al. Factors affecting sentinel node metastasis in thin (T1) cutaneous melanomas: development and external validation of a predictive nomogram. J Clin Oncol. 2020;38:1591–601.
Clark WH, Elder DE, Guerry D, Braitman LE, Trock BJ, Schultz D, et al. Model predicting survival in stage I melanoma based on tumor progression. J Natl Cancer Inst. (1989) https://doi.org/10.1093/jnci/81.24.1893.
Abramova L, Slingluff CL, Patterson JW. Problems in the interpretation of apparent ‘radial growth phase’ malignant melanomas that metastasize. J Cutan Pathol. 2002;29:407–14.
Shon W, Frishberg DP, Gershenwald JE, Gill P, North J, Prieto VG, et al. Protocol for the Examination of Biopsy Specimens From Patients With Melanoma of the Skin. Version: Melanoma Biopsy 4.1.0.0. https://documents.cap.org/protocols/cp-skin-melanoma-excision-19-4100.docx (Accessed on 1.8.2020).
Kang S, Barnhill RL, Mihm MC, Sober AJ. Histologic regression in malignant melanoma: an interobserver concordance study. J Cutan Pathol 1993;20:126–9.
Requena C, Botella-Estrada R, Traves V, Nagore E, Almenar S, Guillen C.Problems in defining melanoma regression and prognostic implication. Actas Dermo-Sifiliográficas (English Ed.). 2009;100:759–66.
Azimi F, Scolyer RA, Rumcheva P, Moncrieff M, Murali R, McCarthy SW, et al. Tumor-infiltrating lymphocyte grade is an independent predictor of sentinel lymph node status and survival in patients with cutaneous melanoma. J Clin Oncol. 2012;30:2678–83.
Thomas NE, Busam KJ, From L, Kricker A, Armstrong BK, Anton-Culver H, et al. Tumor-infiltrating lymphocyte grade in primary melanomas is independently associated with melanoma-specific survival in the population-based genes, environment and melanoma study. J Clin Oncol. 2013;31:4252–9.
Saldanha G, Flatman K, Teo KW, Bamford M. A Novel Numerical Scoring System for Melanoma Tumor-infiltrating Lymphocytes Has Better Prognostic Value Than Standard Scoring. The American Journal of Surgical Pathology, 2017:41;906–14. https://doi.org/10.1097/PAS.0000000000000848.
Fu Q, Chen N, Ge C, Li R, Li Z, Zeng B, et al. Prognostic value of tumor-infiltrating lymphocytes in melanoma: a systematic review and meta-analysis. Oncoimmunology. 2019;8:1–14.
Scolyer RA, Balamurgan T, Busam K, Elder D, Evans A, Gershenwald J, et al. Invasive melanoma, histopathology reporting guide. 2nd edition. Sydney, Australia: International Collaboration on Cancer Reporting; 2019. ISBN: 978-1-92568732-3
Funding
KA is supported by Deborah McMurtrie and John McMurtrie AM through the McMurtrie Cancer Pathology Fellowship. MAES was supported by a Research Fellowship Grant from the European Association of Dermatology and Venereology (EADV). JFT and RAS are recipients of an Australian National Health and Medical Research Council (NHMRC) Program Grant (APP1093017). RAS is supported by an NHMRC Practitioner Fellowship (APP1141295). RPMS is supported by Melanoma Institute Australia. Support from the Cameron Family as well as from colleagues at Melanoma Institute Australia, Royal Prince Alfred Hospital and NSW Health Pathology is gratefully acknowledged.
Author information
Authors and Affiliations
Contributions
Conceptualization: KA, RAS; Data acquisition and interpretation: All authors; Project Administration and support: JFT, RAS; Supervision: RAS; Writing of Initial Draft of Manuscript: KA; Manuscript Review and Approval: All authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted in accordance with the ethical approval from the Sydney Local Health District Human Research Ethics Committee (Protocol No. X15-0454 and HREC/11/RPAH/444).
Competing interests
RAS has received fees for professional services from Evaxion, Provectus Biopharmaceuticals Australia, Qbiotics, Novartis, Merck Sharp & Dohme, NeraCare, AMGEN Inc., Bristol-Myers Squibb, Myriad Genetics, GlaxoSmithKline. JFT has received honoraria for advisory board participation from Bristol-Myers Squibb, Merck Sharp & Dohme Australia, GlaxoSmithKline and Provectus Inc, and travel support from GlaxoSmithKline and Provectus Inc. RPMS has received honoraria for advisory board participation from MSD, Novartis and Qbiotics and speaking honoraria from BMS. All other authors have no relevant disclosures.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: Due to an table error.
Supplementary information
Rights and permissions
About this article

Cite this article
Aivazian, K., Ahmed, T., El Sharouni, MA. et al. Histological regression in melanoma: impact on sentinel lymph node status and survival. Mod Pathol 34, 1999–2008 (2021). https://doi.org/10.1038/s41379-021-00870-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41379-021-00870-2
