
Abstract
Mature B-cell neoplasms and immature or precursor B-cell neoplasms need to be distinguished because these patients usually require different therapeutic approaches. B-cell neoplasms that express TdT without unequivocal other features of immaturity may therefore present a diagnostic challenge. We describe 13 patients with TdT-positive aggressive B-cell lymphoma. The clinicopathologic features of these patients were highly heterogeneous, but for the purpose of this study we grouped these cases as follows: (1) de novo high-grade B-cell lymphoma with MYC, BCL2, and/or BCL6 rearrangements (double-hit or triple-hit lymphoma) with TdT expression. In this group we included two cases of de novo composite lymphoma in which there were components of diffuse large B-cell lymphoma and TdT-positive blastic B-cell lymphoma; (2) TdT-positive aggressive B-cell lymphoma arising in patients who previously had follicular lymphoma; (3) initial relapse of TdT-negative aggressive B-cell lymphoma in patients who previously had follicular lymphoma, followed by relapses in which the neoplasm acquired TdT expression; and (4) mature B-cell lymphomas that acquired TdT expression at relapse. This group included one case of EBV-positive diffuse large B-cell lymphoma and one case of pleomorphic variant mantle cell lymphoma. All patients in this study had an aggressive clinical course and a dismal outcome despite appropriate therapy. Rather than “squeezing” these cases into current World Health Organization classification categories, we suggest the use of a descriptive term such as high-grade B-cell lymphoma with TdT expression. In these tumors, the cytogenetic findings and poor prognosis of this patient subgroup suggest that these neoplasms need to be distinguished from B-lymphoblastic leukemia/lymphoma. Segregation of these neoplasms also may foster additional research on these neoplasms.
Similar content being viewed by others


Introduction
Distinguishing mature B-cell lymphomas from immature or precursor B-cell neoplasms is important because different therapeutic approaches are often used. For example, most patients with diffuse large B-cell lymphoma (DLBCL) are treated in a similar way, most often with the R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) chemotherapy regimen whereas patients with B-lymphoblastic leukemia/lymphoma are treated with more intensive chemotherapy. Morphology provides important information, but it is well known that some mature B-cell neoplasms can have relatively immature morphologic features and present in a fashion similar to a leukemia. Lack of immunoglobulin light chains, dim or lack of expression of CD20, and expression of CD34, CD99 or terminal deoxynucleotidyl transferase (TdT) in neoplastic cells have been used as features to support immaturity. Morphologic review combined with a detailed immunophenotypic workup accurately classifies B-cell neoplasms in most cases. However, expression of TdT in World Health Organization (WHO) classification defined categories of B-cell lymphoma that are typically negative for TdT can occur rarely and present a diagnostic challenge [1, 2].
Perhaps the best known example of TdT expression by a mature B-cell lymphoma is progression of follicular lymphoma. At time of histological transformation to a higher-grade neoplasm, a small subset of follicular lymphoma cases can progress to a neoplasm that expresses TdT. The current recommendation in the WHO scheme is to classify these neoplasms as B-lymphoblastic lymphoma/leukemia transformed from follicular lymphoma [3,4,5]. A subset of these rare neoplasms also may carry MYC, BCL2, and/or BCL6 rearrangements (double-hit or triple-hit lymphoma), a known poor prognostic subset. Less information is available about other types of mature B-cell lymphoma that acquire TdT expression and few guidelines regarding these neoplasms are available in the literature or in the WHO scheme.
In this study, we describe 13 patients with a high-grade B-cell lymphoma that expressed TdT. This group is highly heterogeneous at the clinical and pathologic level and all patients had a dismal outcome despite being treated with intensive chemotherapy. It seems likely that these patients will require novel therapeutic approaches, and we suggest that TdT-positive mature B-cell lymphomas need to be segregated to facilitate the design of better therapies and foster additional research.
Materials and methods
Study group
We searched our institutional archives for patients with a diagnosis of B-cell lymphoma with TdT expression between January 1, 2007 and December 31, 2017. We also searched for any patients carrying the diagnosis of B-acute lymphoblastic leukemia who had a documented history of follicular lymphoma within the same period. Clinical and diagnostic data were obtained by review of the medical records. This study was approved by the institutional review board at The University of Texas MD Anderson Cancer Center.
Histologic and immunophenotypic methods
Tissue sections of biopsy specimens stained with hematoxylin-eosin and bone marrow aspirate smears stained with Wright-Giemsa were reviewed. The biopsy specimens were obtained from bone marrow, lymph nodes, or extranodal sites. Bone marrow biopsy specimens were decalcified using formic acid.
We performed multicolor flow cytometry immunophenotypic analysis on cell suspensions of tissue biopsy specimens or bone marrow aspirate specimens collected in EDTA-anticogulant and processed within 24 h of collection as described previously [6]. Erythrocytes were lysed with ammonium chloride (Pharm LyseTM, BD Biosciences, San Diego, CA) at room temperature for 10 min using a standard lyse/wash technique after incubation with monoclonal antibodies for 10 min at 4 °C. The following antibodies were used: CD2, cytoplasmic CD3, surface CD3, CD4, CD5, CD7, CD10, CD13, CD14, CD15, CD19, CD20, CD22, CD25, CD33, CD34, CD36, CD38, CD41, CD45, CD49d, CD52, CD56, CD64, CD66c, cytoplasmic CD79a, CD81, CD117, CD123, CD184, cytoplasmic IgM, human leukocyte antigen (HLA)-DR, kappa, lambda, myeloperoxidase, and terminal deoxynucleotidyl transferase (TdT). All antibodies were purchased from BD Biosciences (BD Biosciences). Samples were acquired on FACSCanto II instruments (BD Biosciences, San Diego, CA) and analysis of flow cytometry data was performed using FCS Express software (De Novo Software, Los Angeles, CA).
Immunohistochemical analysis was performed using formalin fixed, paraffin-embedded tissue sections as described previously [7]. The antibody panel included reagents specific for: CD3, CD20, CD30, CD79a, CD138, BCL6, and Ki-67 (Dako North America, Carpinteria, CA); CD5 and cyclin D1 (Thermo Scientific, Fremont, CA); CD34 and PAX5 (BD Biosciences); BCL2 and TdT (Leica Biosystems, Buffalo Grove, IL); and MYC (Ventana, Tucson, AZ). In situ hybridization for Epstein-Barr virus encoded small RNA (EBER) (Ventana) was also performed.
Conventional cytogenetic analysis and fluorescence in situ hybridization (FISH)
Conventional cytogenetic analysis was performed on G-banded metaphase cells prepared from unstimulated bone marrow aspirate cultures using standard techniques [8]. Twenty metaphases were analyzed and the results reported using the International Systems for Human Cytogenetic Nomenclature [9]. Fluorescence in situ hybridization (FISH) was performed on bone marrow smears or tissue samples to assess for MYC rearrangement (LSI MYC dual color, breakapart probe), IGH-BCL2 fusion (LSI IGH/BCL2 dual color, dual fusion probe), BCL6 rearrangement (LSI BCL6 dual color, breakapart probe) or BCR-ABL1 fusion (LSI BCR/ABL ES probe) as described previously [7]. All FISH probes were obtained from Abbott Molecular, Inc., (Des Plaines, IL). At least 200 interphases were analyzed.
Statistical analysis
Overall survival (OS) was defined from the day of diagnosis of a TdT-positive B-cell lymphoma to the last follow-up or death. Patients who underwent stem cell transplant were censored. Distribution of OS was estimated with the Kaplan-Meier method, with difference compared by the log-rank test. All P values are two-tailed and considered significant when < 0.05. Statistical analysis was performed using GraphPad Prism 5.0.
Results
De novo high-grade B-cell lymphoma with double-hit or triple-hit genetics and TdT expression
This group included five men and one woman who did not have a history of indolent lymphoma. This group included two subgroups. The first subgroup included four men (cases #1–4) who presented with newly found lumps or masses with or without B symptoms. Pathologic examination showed a diffuse proliferation of medium-sized lymphoid cells with round nuclear contours, open chromatin, inconspicuous nucleoli, and scant cytoplasm (Fig. 1a). Touch imprints showed a predominance of monomorphic medium-sized cells with scant basophilic cytoplasm, round nuclei and inconspicuous nucleoli. Apoptosis was frequent and a starry-sky appearance was present. Mitotic figures were easily seen.

De novo high-grade B-cell lymphoma with MYC, BCL2, and BCL6 rearrangements and TdT expression. a Hematoxylin and eosin, x400. b CD20 stain, x400. c Ki-67, x400. d TdT, x400
The neoplastic cells were positive for CD10, CD19, CD20, PAX-5, BCL6 (partial), MUM-1/IRF4, TdT and monotypic surface immunoglobulin light chain expression, but were negative for CD34. Ki-67 was 95–100% (Fig. 1b, d).
Conventional karyotyping was not performed in these patients. FISH demonstrated rearrangements of MYC and BCL2 in two patients (cases #1 and 2) and MYC, BCL2, and BCL6 in two patients (cases #3 and 4). These patients were treated with rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin (R-EPOCH) (cases #1, 2, and 4) or EPOCH (case #3). Clinical follow-up was available for three of these patients. One patient (case #1) went to his hometown for treatment and was lost for follow-up. In case #2, the patient underwent autologous stem cell transplant after achieving complete remission with R-EPOCH. However, this patient developed relapse 14 months later. He was treated with rituximab, hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (R-hyperCVAD) or blinatumomab off protocol, but died 2 months after relapse. Two patients had primary refractory disease; one patient died 8 months after diagnosis (case #3) and in the other patient therapy was changed to rituximab, dexamethasone, cytarabine, and cisplatin (R-DHAP) (case #4).
A second subgroup of two patients had high-grade B-cell lymphoma with a biphasic or composite pattern. Case #5 was a 43-year-old man who sought medical attention for sore throat, dysphagia, and 20-pound weight loss. Endoscopy revealed a right supraglottic mass. Case #6 was a 61-year-old woman who presented with abdominal pain thought initially to be acute cholecystitis. CT scan demonstrated mesenteric lymphadenopathy with the largest lymph node 5.7 centimeters in greatest dimension. Pathologic examination of these two neoplasms showed a biphasic neoplasm. One component resembled DLBCL and was composed of sheets of large lymphoid cells with round-to-ovoid nuclear contours, vesicular chromatin, a single prominent nucleolus, and a moderate amount of cytoplasm (Fig. 2a, b). These large cells were CD10+, CD20+, BCL2+, BCL6 (weak+), Ki-67 ~60%, and TdT(−). A second component was composed of medium-sized lymphoid cells with immature chromatin that were TdT(+), CD10+, CD20(−), CD45(−), BCL2+, BCL6(−), and Ki-67 90–100% (Fig. 2c, d). FISH analysis showed MYC and BCL2 rearrangements in case 5 and MYC, BCL2, and BCL6 rearrangements in case 6. Of note, MYC and BCL2 rearrangements were found in both components of the neoplasm in case #5. Staging bone marrow was negative for lymphoma in both patients. The cerebrospinal fluid was negative for lymphoma in case #5, but not evaluated in patient #6.

De novo high-grade B-cell lymphoma with MYC and BCL2 rearrangements with biphasic appearances of diffuse large B-cell lymphoma and TdT-positive blastic B-cell lymphoma in the same lymph node. a Hematoxylin and eosin, x400. b Left. Blastic B-cell lymphoma component, x1,000. b Right. Diffuse large B-cell lymphoma (DLBCL) component, x1,000. c CD20 expression is only present in the DLBCL component, x200. d TdT stain in the blastic B-cell lymphoma component, x200
Clinical follow-up was available. In case #5, the patient was treated with a chemotherapy regimen designed for B-lymphoblastic lymphoma/leukemia (daunorubicin, cyclophosphamide, vincristine sulfate, and L-asparaginase), but after a preliminary response the patient had recurrence and underwent allogeneic stem cell transplant 6 months after diagnosis. The patient died 2 months after the transplant. In case #6, the patient achieved partial remission after six cycles of R-EPOCH and is being considered for stem cell transplant at time of writing.
Follicular lymphoma followed by TdT-positive aggressive B-cell lymphoma
Three patients belong to this group. Two patients (cases #7 and #9) had follicular lymphoma, grade 1 involving axillary lymph nodes, and one patient (case #8) had follicular lymphoma, grade 2 in the right parotid gland. Patient #7 also had squamous cell carcinoma of the tonsil and initial treatment was designed for the tonsillar cancer. The other two patients were treated with R-CHOP and achieved complete remission. With a median interval of 13 months (range, 11 to 18 months), all three patients developed aggressive and high-grade B-cell lymphoma involving the left mandible (case #7), abdomen (#8), and left axillary lymph node (#9), respectively. Bone marrow was not involved by lymphoma in all patients.
Pathologic examination of these lymphomas showed lymph node or extranodal sites diffusely involved by sheets of medium-to-large lymphoid cells with a starry-sky appearance. The neoplastic cells had round to slightly irregular nuclear contours, fine chromatin and scant cytoplasm. Mitotic figures were frequent. The neoplastic cells were positive for CD10, CD19, and TdT and were negative for CD20, CD34, and surface immunoglobulin by flow cytometry. Immunohistochemical analysis showed BCL6 was expressed in one neoplasm (case #9). Ki-67 was 90–100% in all patients. FISH to assess MYC, BCL2, and BCL6 was performed using formalin-fixed, paraffin-embedded tissue in two neoplasms (cases #8 and 9), but results were successful in only case #9 who had MYC and BCL2 rearrangements. In case #7 tissue remaining in the paraffin block was insufficient for FISH studies.
Two patients were treated with R-hyperCVAD therapy. One patient (case #7) did not respond to therapy and died 3.2 months after diagnosis. The other patient (case #9) showed a very good response to the therapy and underwent autologous stem cell transplant, but the disease progressed 1.5 months after the transplant. This patient was treated with various modalities including radiation, R-DHAP chemotherapy, and chimeric antigen receptor T-cell infusion, but died 5.3 months after the autologous stem cell transplant. Patient #8 responded initially to rituximab, ifosfamide, and etoposide, but developed recurrence 3 months later. He was switched to R-hyperCVAD, but had progressive disease involving the kidney, lower retroperitoneum, extraperitoneal space, and testis and died 6.1 months after diagnosis.
Initial TdT-negative aggressive B-cell lymphoma in patients who previously had follicular lymphoma, followed by relapses in which the neoplasm acquired TdT expression
There were two patients in this category who had a history of follicular lymphoma, treated with immunochemotherapy achieving partial (case #10) or complete remission (case #11). Eleven and 14 months after diagnosis, respectively, new lymphadenopathy appeared and histologic examination showed a diffuse (case #10) or diffuse and nodular (case #11) proliferation of medium-sized lymphoid cells with round nuclear contours, open chromatin, 2–3 nucleoli and moderate amount of cytoplasm (Fig. 3a). A starry-sky pattern was focally present and mitotic figures were frequent. Flow cytometry sowed CD10+/CD19+/CD20(-) aberrant B-cells with monotypic surface light chain expression. Immunohistochemical analysis showed that the neoplastic cells were positive for BCL2 and BCL6 (weak) and negative for TdT (Fig. 3b). Ki-67 rate was 100% in case #10 and 70% in case #11. In case 11, MYC and BCL2 rearrangements were detected by FISH. Both neoplasms were classified as high-grade B-cell lymphoma and, in case 11, with MYC and BCL2 rearrangements (double-hit lymphoma), likely transformed from follicular lymphoma. Staging bone marrow biopsy was negative for lymphoma in case 10.

High-grade B-cell lymphoma with MYC and BCL2 rearrangements with TdT expression. This patient had a history of follicular lymphoma and relapse with aggressive B-cell lymphoma without TdT expression (a and b) before additional relapse associated with TdT expression (c and d). a Hematoxylin and eosin, x400. b TdT, x400. c Hematoxylin and eosin, x400. d TdT, x400
Patient #10 was treated with R-CHOP therapy, but suffered from tumor lysis syndrome with renal failure. Due to atypical lymphoid cells identified in the peripheral blood, a second bone marrow aspiration and biopsy were performed 3 weeks after the diagnosis of the high-grade B-cell lymphoma. The bone marrow was hypercellular (90%) with diffuse sheets of immature-appearing cells (Fig. 3c). The aspirate smears showed 74% medium-sized immature cells with TdT expression by immunofluorescence. Flow cytometry immunophenotyping showed that the immature cells were positive for CD10, CD19, and TdT, and negative for CD20, surface and cytoplasmic immunoglobulin light chains. Conventional karyotype showed a complex karyotype with t(8;14)(q24.1;q32) and t(14;18)(q32;q21.3). The patient was treated with R-hyperCVAD but did not respond and died 5.4 months after development of the TdT+ high-grade B-cell lymphoma/leukemia.
Patient #11 was treated with rituximab, ifosfamide, carboplatin, and etoposide (R-ICE) following the diagnosis of high-grade B-cell lymphoma with MYC and BCL2 rearrangement and achieved complete remission. Subsequently, she underwent autologous stem cell transplant, but was found to have a recurrent disease in the retroperitoneum 3 months later. The immunophenotype was identical to the previous double-hit lymphoma. However, bone marrow showed diffuse sheets of immature-appearing cells, positive for TdT, PAX-5, and BCL2 and negative for CD20, CD34, BCL6 and cyclin D1 with Ki-67 90% (Fig. 3d). Flow cytometry showed CD45 dim+ cells, positive for CD10, CD19, and CD38 and negative for CD5, CD20, and surface immunoglobulin. She was treated with radiation and lenalidomide but died approximately 1 month later from TdT+ high-grade B-cell lymphoma/leukemia.
Mature B-cell lymphomas that acquired TdT expression at relapse
Two patients are included in this group. A 71-year-old man (case #12) had a fall resulting in significant back pain went to a local emergency room for evaluation. CT scan revealed lymphadenopathy involving the retroperitoneum and left external iliac region. Pathologic examination of a retroperitoneal lymph node showed a diffuse proliferation of large atypical lymphoid cells with round-to-ovoid nuclear contours, vesicular chromatin, prominent single-to-multiple nucleoli and moderate amount of cytoplasm, imparting an immunoblastic or plasmablastic appearance (Fig. 4a). A starry-sky pattern with numerous apoptotic bodies and mitotic figures were present. The neoplastic cells were positive for TdT, CD10 (weak), CD79a, PAX-5, BOB.1, and CD45 and were negative for CD5, CD20, CD34, CD138, ALK-1, BCL2, BCL6, cyclin D1, EMA, HHV8, kappa and lambda light chains, MUM-1, and OCT2. In situ hybridization for Epstein-Barr virus encoded small RNA was strongly positive in the neoplastic cells (Fig. 4b, d). Ki-67 was 95–100%. FISH analysis showed MYC rearrangement, but no evidence of BCL2 and BCL6 rearrangement. The case was thought best classified as EBV-positive DLBCL, but unusual features for this diagnosis included MYC rearrangement and TdT expression. The patient was treated with one cycle of EPOCH in his hometown and came to our institution for a second opinion. The R-CHOP regimen was recommended but the patient wanted to be treated at a local hospital and was lost for follow-up.

Epstein-Barr virus-positive diffuse large B-cell lymphoma with TdT expression. a Hematoxylin and eosin, x400. b In situ hybridization of Epstein-Barr virus encoded small RNA (EBER), x200. c Ki-67, x400. d TdT, x400
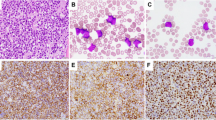
A 59-year-old woman (case #13) presented to our institution complaining of an inability to swallow and close her mouth due to facial weakness. She was status post three cycles of R-CHOP therapy for mantle cell lymphoma in leukemic phase diagnosed at an outside hospital 2 months prior to her visit. Magnetic resonance imaging brain scan was consistent with diffuse leptomeningeal enhancement, particularly involving cranial nerves III, V, VII, and VIII. Lymph node biopsy showed a diffuse proliferation of medium-sized cells with round to irregular nuclei, fine chromatin, small nucleoli and scant cytoplasm (Fig. 5a). Flow cytometry immunophenotyping demonstrated a monotypic B-cell population with surface kappa light chain, positive for CD5, CD10, CD19, CD20, CD22, CD38, CD43, CD44, and CD79b. Immunohistochemical studies revealed that the lymphoid cells were positive or PAX-5, BCL2, and cyclin D1, consistent with mantle cell lymphoma. Ki-67 was approximately 70%. TdT expression was also observed in a subset of lymphoma cells (Fig. 5b, d). FISH analysis was negative for MYC rearrangement. Lumbar puncture was positive for lymphoma cells. Bone marrow was negative for lymphoma. She was treated with high-dose methotrexate with cytarabine intrathecal therapy. Patient wanted to receive treatment in her hometown and there is no further follow-up.

Blastoid mantle cell lymphoma with TdT expression. a Hematoxylin and eosin, x400. b Cyclin D1 stain, x400. c Ki-67, x400. d TdT, x400
Discussion
We report 13 patients with high-grade B-cell lymphoma with TdT expression. These patients had heterogeneous histories and clinicopathologic features, but we have arbitrarily divided them into four groups for the purpose of organizing the data (Fig. 6). The first group is de novo high-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements and TdT expression. Four of these patients had a homogeneous appearing neoplasm and two patients had a composite lymphoma with areas of TdT(−) DLBCL and TdT(+) blastic B-cell lymphoma. In case #5, both components showed rearrangements of MYC and BCL2, suggesting that both components arose from a common clone. Alternatively, the TdT(−) DLBCL component possibly could have been an intermediate step on the way to developing TdT(+) blastic B-cell lymphoma, representing a rare “snapshot” of the transformation.

Four groups of high-grade B-cell lymphoma/leukemia with TdT expression. DHL high-grade B-cell lymphoma with MYC and BCL2 rearrangements (double-hit lymphoma), THL high-grade B-cell lymphoma with MYC, BCL2, and BCL6 rearrangements (triple-hit lymphoma), FL follicular lymphoma
We believe these neoplasms would be diagnosed as B-lymphoblastic lymphoma/leukemia if the WHO recommendations and scheme are strictly applied. However, the cases in this study did not show other features supporting immaturity such as expression of CD34 or lack of expression of surface immunoglobulin. Furthermore, we suggest that the presence of double-hit genetics is sufficiently distinctive to support recognizing these neoplasms as being different from typical de novo B-lymphoblastic lymphoma/leukemia for two reasons. First, rearrangements in MYC and BCL2 and/or BCL6 are extremely rare in de novo B-lymphoblastic lymphoma/leukemia [10,11,12]. In a single center retrospective study, three of 1624 (0.2%) patients with de novo B-lymphoblastic lymphoma/leukemia had rearrangements in MYC and BCL2 [12]. Second, these patients have a dismal prognosis, similar to other patients with double- or triple-hit lymphoma, despite receiving chemotherapy designed for B-lymphoblastic lymphoma/leukemia [10,11,12]. The median OS of the six patients in this study was 13.1 months, similar to the prognosis of patients with double- or triple-hit lymphoma without TdT expression [13, 14]. Accordingly, we are reluctant to use TdT expression to support a diagnosis of B-lymphoblastic lymphoma/leukemia in the context of findings otherwise supporting the diagnosis of high-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements. Instead, we emphasize the cytogenetic findings and use a descriptive term such as blastic B-cell lymphoma with rearrangements in MYC, BCL2, and/or BCL6.
A second group of three patients had a history of follicular lymphoma and developed a TdT-positive blastic B-cell lymphoma. Although we did not test the clonal relationship of the FL and subsequent TdT-positive blastic B-cell lymphoma, this occurrence is recognized in the literature as a rare form of high-grade transformation of follicular lymphoma. While there is only one patient with documented double-hit genetics in this group, it is possible one or both of the other patients could have had double-hit genetics if sufficient tissue was available for FISH [3,4,5, 15,16,17,18,19,20,21]. Despite the presence of double-hit genetics, as we understand the WHO classification system, the recommendation is to use the term B-lymphoblastic lymphoma transformed from FL. We agree that this approach is useful for distinguishing these cases from de novo B-lymphoblastic lymphoma/leukemia, but we suggest that this designation does not fully convey the substantially worse outcome of patients with follicular lymphoma who progress to TdT-positive aggressive lymphoma as compared to patients with de novo B-lymphoblastic lymphoma/leukemia. Available data show that these patients usually have a highly aggressive clinical course and have significantly worse outcome compared with de novo B-lymphoblastic lymphoma/leukemia irrespective of Philadelphia chromosome (Ph) status. Hyper-CVAD based regimens represent the standard treatment for patients with B-lymphoblastic lymphoma/leukemia. In patients with B-acute lymphoblastic leukemia, a complete remission rate of > 90% with a 5-year OS of 40% is commonly achieved [22]. With the introduction of tyrosine kinase inhibitors, the outcomes of Ph + B-acute lymphoblastic leukemia also have been improved with a 5-year OS of around 50% [23]. In this study, patients underwent hyper-CVAD-based intensive chemotherapy, and the median OS for this group was only 5.3 months.
The third group is likely related to the second group as both patients had a history of follicular lymphoma. However, this group is intriguing because these tumors suggest that high-grade B-cell lymphoma with double-hit genetics without TdT expression could be an intermediate step to B-lymphoblastic lymphoma/leukemia with double-hit genetics. In the third group, patients with a history of follicular lymphoma developed TdT-negative double-hit lymphoma and then acquired TdT expression at later relapse. Similar observations have been reported by others [16, 20]. Whether there is an intermediate step of TdT-negative double-hit lymphoma that occurs during the leukemogenesis of TdT-positive double-hit lymphoma remains to be elucidated, but we show that at least a subset of patients can show this pattern of tumor evolution.
The fourth group in this study included two patients with mature high-grade B-cell lymphoma with TdT expression. These cases also posed a diagnostic dilemma because of discordant expression of an immature marker (TdT) in otherwise mature B-cell lymphomas: EBV-positive DLBCL and mantle cell lymphoma. Except for TdT expression, other features supporting immaturity were not present in these tumors. To the best of our knowledge, TdT expression has not been reported in patients with EBV-positive DLBCL. A single case of mantle cell lymphoma with concurrent TdT and cyclin D1 expression has been reported [24].
Terminal deoxynucleotidyl transferase is a DNA polymerase that incorporates nucleotides to the 3’-OH-terminal of single-stranded DNA in a template-independent manner. TdT plays an essential role in increasing antigen receptor diversity by catalyzing random addition of deoxyribonucleotides to single-stranded DNA during V(D)J recombination of the immunoglobulin and T-cell receptor genes [25]. In normal tissue, TdT expression is mostly confined to B- or T-cell precursors in the thymus and bone marrow, but not in mature lymphocytes [26]. During B-cell development, TdT is normally expressed at the pro-B-cell stage, but its expression gradually declines and disappears when IGH rearrangement is complete and IGK or IGL rearrangement begins (the pre-B-cell stage). In lymphoid neoplasms, TdT is expressed in most cases of acute B- or T-lymphoblastic leukemia/lymphoma. In contrast, most studies have shown that TdT expression is absent in other types of B- and T-cell lymphoma [27,28,29]. However, TdT is not a specific marker for B- or T-lymphoblastic lymphoma/leukemia because expression of TdT also can be seen in acute myeloid leukemia with minimal differentiation, blastic plasmacytoid dendritic cell neoplasm and Merkel cell carcinoma [30,31,32].
The data in this study show that TdT can be expressed rarely in mature B-cell lymphomas, usually at time of progression or relapse. In the current WHO classification, cases of follicular lymphoma that transform to a high-grade B-cell lymphoma with TdT expression are considered as lymphoblastic transformation of FL. This terminology, in our opinion, may suggest that these neoplasms may behave similarly to de novo B-lymphoblastic lymphoma/leukemia and the experience reported here shows that this is not the case. Many of these neoplasms have rearrangements in MYC, BCL2 and/or BCL6 and a very poor prognosis. Currently, the WHO classification provides less guidance for cases of de novo high-grade B-cell lymphoma with double/triple hit genetics that express TdT or for mature B-cell neoplasms other than follicular lymphoma that relapse as TdT-positive high-grade B-cell lymphoma. In our opinion, using the designation of lymphoblastic transformation in these contexts is potentially confusing. Furthermore, we suggest that such designation does not capture the essence of these diseases and might potentially misguide patient management. We therefore suggest a descriptive term such as high-grade B-cell lymphoma with TdT expression with emphasis on cytogenetic findings to convey their distinctive nature, which is distinct from typical B-lymphoblastic lymphoma/leukemia. It should be emphasized, however, that this terminology is not intended to be used for typical cases of B-lymphoblastic leukemia/lymphoma. Furthermore, this terminology is not intended for rare cases of B-lymphoblastic leukemia/lymphoma with surface light chain expression [33].
In summary, we have described 13 cases of B-cell lymphoma at time of initial diagnosis or relapse characterized by aggressive morphologic features, a B-cell immunophenotype, a poor prognosis, and TdT expression that do not easily fit into current WHO classification defined entities. We suggest the term high-grade B-cell lymphoma with TdT expression for these neoplasms. Segregating these rare tumors may be useful for prognostication and also may facilitate additional research and the design of novel therapeutic approaches for these patients.
References
Soliman DS, Al-Sabbagh A, Ibrahim F, et al. High-grade B-cell meoplasm with surface light chain restriction and TdT coexpression evolved in a MYC-rearranged diffuse large B-cell lymphoma: a dilemma in classification. Case Rep Hematol. 2017;2017:6891957.
Moench L, Sachs Z, Aasen G, et al. Double- and triple-hit lymphomas can present with features suggestive of immaturity, including TdT expression, and create diagnostic challenges. Leuk Lymphoma. 2016;57:2626–35.
De Jong D, Voetdijk BM, Beverstock GC, et al. Activation of the c-myc oncogene in a precursor-B-cell blast crisis of follicular lymphoma, presenting as composite lymphoma. N Engl J Med. 1988;318:1373–8.
Kroft SH, Domiati-Saad R, Finn WG, et al. Precursor B-lymphoblastic transformation of grade I follicle center lymphoma. Am J Clin Pathol. 2000;113:411–8.
Young KH, Xie Q, Zhou G, et al. Transformation of follicular lymphoma to precursor B-cell lymphoblastic lymphoma with c-myc gene rearrangement as a critical event. Am J Clin Pathol. 2008;129:157–66.
Ok CY, Leventaki V, Wang SA, et al. Detection of an abnormal myeloid clone by flow cytometry in familial platelet disorder with propensity to myeloid malignancy. Am J Clin Pathol. 2016;145:271–6.
Kanagal-Shamanna R, Medeiros LJ, Lu G, et al. High-grade B cell lymphoma, unclassifiable, with blastoid features: an unusual morphological subgroup associated frequently with BCL2 and/or MYC gene rearrangements and a poor prognosis. Histopathology. 2012;61:945–54.
Montenegro-Garreaud X, Miranda RN, Reynolds A, et al. Myeloproliferative neoplasms with t(8;22) (p11.2;q11.2)/BCR-FGFR1: a meta-analysis of 20 cases shows cytogenetic progression with B-lymphoid blast phase. Hum Pathol. 2017;65:147–56.
McGowan-Jordan J, Simons A, Schmid M. An international system for human cytogenomic nomenclature. Basel (Switzerland): Karger; 2016.
Thangavelu M, Olopade O, Beckman E, et al. Clinical, morphologic, and cytogenetic characteristics of patients with lymphoid malignancies characterized by both t(14;18)(q32; q21) and t(8;14)(q24;q32) or t(8;22)(q24;q11). Genes Chromosomes Cancer. 1990;2:147–58.
Subramaniyam S, Fraser CR, Rao PH, et al. De novo B lymphoblastic leukemia/lymphoma in an adult with t(14;18)(q32; q21) and c-MYC gene rearrangement involving 10p13. Leuk Lymphoma. 2011;52:2195–9.
Liu W, Hu S, Konopleva M, et al. De novo MYC and BCL2 double-hit B-cell precursor acute lymphoblastic leukemia (BCP-ALL) in pediatric and young adult patients associated with poor prognosis. Pediatr Hematol Oncol. 2015;32:535–47.
Li S, Lin P, Fayad LE, et al. B-cell lymphomas with MYC/8q24 rearrangements and IGH@BCL2/t(14;18)(q32; q21): an aggressive disease with heterogeneous histology, germinal center B-cell immunophenotype and poor outcome. Mod Pathol. 2012;25:145–56.
Oki Y, Noorani M, Lin P, et al. Double hit lymphoma: the MD Anderson Cancer Center clinical experience. Br J Haematol. 2014;166:891–901.
Gauwerky CE, Hoxie J, Nowell PC, et al. Pre-B-cell leukemia with a t(8; 14) and a t(14; 18) translocation is preceded by follicular lymphoma. Oncogene. 1988;2:431–5.
Geyer JT, Subramaniyam S, Jiang Y, et al. Lymphoblastic transformation of follicular lymphoma: a clinicopathologic and molecular analysis of 7 patients. Hum Pathol. 2015;46:260–71.
Kaplan A, Samad A, Dolan MM, et al. Follicular lymphoma transformed to “double-hit” B lymphoblastic lymphoma presenting in the peritoneal fluid. Diagn Cytopathol. 2013;41:986–90.
Kishimoto W, Shirase T, Chihara D, et al. Double-hit lymphoma with a feature of follicular lymphoma concurrent with clonally related B lymphoblastic leukemia: a preference of transformation for the bone marrow. J Clin Exp Hematop. 2012;52:113–9.
Kobrin C, Cha SC, Qin H, et al. Molecular analysis of light-chain switch and acute lymphoblastic leukemia transformation in two follicular lymphomas: implications for lymphomagenesis. Leuk Lymphoma. 2006;47:1523–34.
Slot LM, Hoogeboom R, Smit LA, et al. B-lymphoblastic lymphomas evolving from follicular lymphomas co-express surrogate light chains and mutated gamma heavy chains. Am J Pathol. 2016;186:3273–84.
Sun X, Gordon LI, Peterson LC. Transformation of follicular lymphoma to acute lymphoblastic leukemia. Arch Pathol Lab Med. 2002;126:997–8.
Thomas DA, O’Brien S, Faderl S, et al. Chemoimmunotherapy with a modified hyper-CVAD and rituximab regimen improves outcome in de novo Philadelphia chromosome-negative precursor B-lineage acute lymphoblastic leukemia. J Clin Oncol. 2010;28:3880–9.
Ravandi F, O’Brien S, Thomas D, et al. First report of phase 2 study of dasatinib with hyper-CVAD for the frontline treatment of patients with Philadelphia chromosome-positive (Ph + ) acute lymphoblastic leukemia. Blood. 2010;116:2070–7.
Kallen ME, Rao NP, Kulkarni SK, et al. B-lymphoblastic transformation of mantle cell lymphoma/leukemia with “double hit” changes. J Hematop. 2015;8:31–6.
Motea EA, Berdis AJ. Terminal deoxynucleotidyl transferase: the story of a misguided DNA polymerase. Biochim Biophys Acta. 2010;1804:1151–66.
Onciu M, Lorsbach RB, Henry EC, et al. Terminal deoxynucleotidyl transferase-positive lymphoid cells in reactive lymph nodes from children with malignant tumors: incidence, distribution pattern, and immunophenotype in 26 patients. Am J Clin Pathol. 2002;118:248–54.
Orazi A, Cattoretti G, John K, et al. Terminal deoxynucleotidyl transferase staining of malignant lymphomas in paraffin sections. Mod Pathol. 1994;7:582–6.
Kung PC, Long JC, McCaffrey RP, et al. Terminal deoxynucleotidyl transferase in the diagnosis of leukemia and malignant lymphoma. Am J Med. 1978;64:788–94.
Suzumiya J, Ohshima K, Kikuchi M, et al. Terminal deoxynucleotidyl transferase staining of malignant lymphomas in paraffin sections: a useful method for the diagnosis of lymphoblastic lymphoma. J Pathol. 1997;182:86–91.
Patel KP, Khokhar FA, Muzzafar T, et al. TdT expression in acute myeloid leukemia with minimal differentiation is associated with distinctive clinicopathological features and better overall survival following stem cell transplantation. Mod Pathol. 2013;26:195–203.
Sangle NA, Schmidt RL, Patel JL, et al. Optimized immunohistochemical panel to differentiate myeloid sarcoma from blastic plasmacytoid dendritic cell neoplasm. Mod Pathol. 2014;27:1137–43.
Sur M, AlArdati H, Ross C, et al. TdT expression in Merkel cell carcinoma: potential diagnostic pitfall with blastic hematological malignancies and expanded immunohistochemical analysis. Mod Pathol. 2007;20:1113–20.
Vasef MA, Brynes RK, Murata-Collins JL, Arber DA, Medeiros LJ. Surfaceimmunoglobulin light chain-positive acute lymphoblastic leukemia of FAB L1 or L2 type. Am J Clin Pathol. 1998;110:143–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Ok, C.Y., Medeiros, L.J., Thakral, B. et al. High-grade B-cell lymphomas with TdT expression: a diagnostic and classification dilemma. Mod Pathol 32, 48–58 (2019). https://doi.org/10.1038/s41379-018-0112-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41379-018-0112-9
This article is cited by
-
Aggressive B-cell non-Hodgkin lymphomas: a report of the lymphoma workshop of the 20th meeting of the European Association for Haematopathology
Virchows Archiv (2024)
-
High-grade B-cell lymphoma (HGBL)-NOS is clinicopathologically and genetically more similar to DLBCL/HGBL-DH than DLBCL
Leukemia (2023)
-
Diagnostic approaches and future directions in Burkitt lymphoma and high-grade B-cell lymphoma
Virchows Archiv (2023)
-
International Consensus Classification of acute lymphoblastic leukemia/lymphoma
Virchows Archiv (2023)
-
Blastoid high-grade B-cell lymphoma initially presenting in bone marrow: a diagnostic challenge
Modern Pathology (2022)
