
Abstract
Objective
We hypothesized that videolaryngoscope use for tracheal intubations would differ across NICUs, be associated with higher first attempt success and lower adverse events.
Study design
Data from the National Emergency Airway Registry for Neonates (01/2015 to 12/2017) included intubation with direct laryngoscope or videolaryngoscope. Primary outcome was first attempt success. Secondary outcomes were adverse tracheal intubation associated events and severe desaturation.
Results
Of 2730 encounters (13 NICUs), 626 (23%) utilized a videolaryngoscope (3% to 64% per site). Videolaryngoscope use was associated with higher first attempt success (p < 0.001), lower adverse tracheal intubation associated events (p < 0.001), but no difference in severe desaturation. After adjustment, videolaryngoscope use was not associated with higher first attempt success (OR:1.18, p = 0.136), but was associated with lower tracheal intubation associated events (OR:0.45, p < 0.001).
Conclusion
Videolaryngoscope use is variable, not independently associated with higher first attempt success but associated with fewer tracheal intubation associated events.
Similar content being viewed by others
Introduction
Tracheal intubation (TI) is a frequently performed procedure in Neonatal Intensive Care Units (NICU) and delivery rooms but is commonly complicated by unsuccessful first intubation attempts, adverse tracheal intubation associated events (TIAEs), and severe oxygen desaturations [1, 2]. Furthermore, success rates are highly variable for neonatal TIs, ranging from 20% for residents to 72% for attending neonatologists [3]. Neonatal TI is not a simple procedure to gain proficiency in and requires a distinctive set of skills. Beside the neonate’s limited respiratory reserve limiting procedural duration, difficulty visualizing the glottis secondary to small oral opening and airway caliber, as well as particular larynx anatomy [4] represent a challenge even for experienced clinicians.
The videolaryngoscope (VL) was introduced to adult and pediatric medicine more than a decade ago [5, 6]. It incorporates a fiberoptic camera lens into the light source of a laryngoscope blade, effectively positioning the laryngoscopist’s eye at the tip of the blade and extending the viewing angle to 80o, compared to the 15o view offered by direct laryngoscopy (DL) [7]. The VL is connected to a video monitor which displays a magnified image [8]. Video-assisted intubation is increasingly recognized as the method of choice in teaching TI because of the view it offers simultaneously to both the trainee and the supervisor [9].
Mannequin studies have reported improved TI success rates and decreased time to intubation using VL [10,11,12]. Videolaryngoscopy has shown its clinical usefulness in infants as small as 530 g [13]. Three clinical trials have shown that VL has the potential to improve success rates for neonatal intubations performed by trainees [14,15,16], however, the potential benefits of VL use in more experienced providers is also needed. The use of VL for NICU TI may improve first attempt intubation success, however, data are limited.
The aim of this study is to evaluate VL use in neonatal TIs across diverse institutions. We hypothesized that the use of VL for TIs would be highly variable across NICUs, and would be associated with higher first attempt success and lower adverse events, after adjusting for patient, provider, and practice factors.
Methods
Study design
This was a retrospective cohort study using prospectively collected neonatal TI data obtained from the National Emergency Airway Registry for Neonates (NEAR4NEOS), an international multicenter quality improvement registry. This study includes data from 13 academic NICUs. The institutional review board at each participating NEAR4NEOS site either approved the study or granted a waiver of informed parental consent for the use of patient data as a quality improvement activity.
Data collection
Using a standardized NEAR4NEOS data collection form, each center collected data on patient, provider, practice, and outcomes for each neonatal TI encounter [2]. These data were recorded by a designated member of the care team immediately after the procedure and later verified for accuracy by the site’s study team. Consistency of data captured was ensured by utilizing NEAR4NEOS standardized operational definitions [2]. Each participating NICU developed a site-specific compliance plan to ensure appropriate data capture of more than 90% of intubations, data verification, and timely data entry into a secured, password protected Research Electronic Data Capture (REDCap) system hosted by the data coordinating center at Children’s Hospital of Philadelphia. TI data from one site without consistent compliance reporting was excluded from the analysis.
Patient data included gestational age, corrected weight on the day of TI, day of life on the day of TI, and associated comorbidities. Practice data included indication for intubation, profession and experience level of the primary airway provider, intubation approach and type of premedication.
Inclusion and exclusion criteria
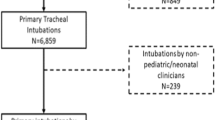
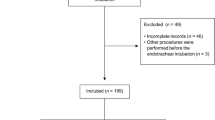
All primary TIs in the NICU between January 2015 and December 2017 were included in the analysis. Primary TIs using either DL or VL in NICUs were included. TIs performed outside the NICU, including in the delivery room, performed by non-NICU personnel, or for endotracheal tube changes were excluded from the analysis.
Direct and video laryngoscopy
The use of DL or VL for intubation was based on provider preference. The device used was noted on the NEAR4NEOS data form at the time of intubation and subsequently uploaded to the NEAR4NEOS database. Options on the data form included ‘ laryngoscope’ to indicate traditional DL or ‘video laryngoscopy’ to indicate the use of a laryngoscopic device with video capabilities. Examples of commonly used VL devices include CMAC, NeoView, Glidescope, InfantView, and Airtraq. Indirect view was defined as the use of video image by the airway provider and direct view was defined as the use of naked eye image by the airway provider.
Definition of outcomes
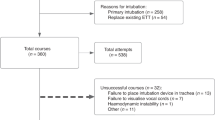
Specific outcomes of interest included the first attempt success (primary outcome), number of intubation attempts, occurrence of TIAEs, and severe oxygen desaturation during the intubation (secondary outcomes). First attempt success was defined as successful intubation on the first attempt by the first provider. TIAEs were categorized as ‘non-severe’ or ‘severe’ using previously described operational definitions [17]. Non-severe TIAEs included esophageal intubation with immediate recognition, mainstem intubation, lip trauma, pain or agitation requiring additional sedation delaying intubation, epistaxis, emesis without aspiration, hypertension requiring therapy, and dysrhythmia including bradycardia with heart rate <60 beats per minute (brief episode for which cardiac compressions were not needed) or an arrhythmia requiring treatment. Severe TIAEs included direct airway injury, esophageal intubation with delayed recognition, emesis with aspiration, laryngospasm, pneumothorax, gum or dental trauma, hypotension requiring intervention, malignant hyperthermia, need for cardiac compressions, and cardiac arrest.
Oxygen desaturations were captured separately from adverse TIAEs. Pulse oximetry was used to identify two oxygen saturation (SpO2) measurements for each intubation: the highest SpO2 measurement immediately before the first intubation attempt, and the lowest measured SpO2 during the intubation encounter. Severe oxygen desaturation was defined as ≥20% decrease in SpO2 from the highest level achieved immediately before the first intubation attempt. This was only reported for TIs in which a pre-intubation SpO2 level was recorded.
Statistical analysis
Descriptive statistics were used to present the demographic data as number and proportion for categorical variables and as median and interquartile range (IQR) for nonparametric data. The relationships between the patient, provider, and practice characteristics with VL use were analyzed using univariate analyses with Chi-square or Fisher’s Exact test for dichotomous variables and with Kruskal-Wallis test for nonparametric variables. The independent effect of VL use on the outcomes was assessed by generalized estimate equation multivariable logistic regression model while controlling for patient, provider, practice factors, and clustering by site. Covariates were included in the multivariable model when there was an association with VL use at p < 0.05 in the univariate analysis. Sensitivity analysis by limiting the cohort to NICUs with > 10 VL TIs was also completed. Statistical analysis was performed using STATA 14.0 (StataCorp, College Station, TX, USA).
Results
Demographics and factors associated with videolaryngoscope use
A total of 2,730 TIs encounters from 13 NICUs were analyzed. Six hundred twenty-eight (23%) TIs utilized a VL, most of which was the C-MAC VL (Karl Storz ©,Tuttlingen, Germany). VL was used in 7 sites, and its use varied across sites (3%–64% per site, Fig. 1 and Supplemental Table A). Tables 1 and 2 describe patient and intubation characteristics comparing intubations done with VL and DL. VL was used more frequently in more mature, larger, and older neonates; when neonates had a congenital or craniofacial anomaly; and in situations of ventilation failure, upper airway obstruction or when an intubation was done for a procedure. DL was more often used in cases of oxygen failure, apnea and bradycardia, absent protective airway reflexes, and surfactant administration. Fellows, neonatal nurse practitioners, physician assistants, and hospitalists were most often the primary airway provider when using VL. Premedication, as a combination of a sedative and a paralytic, was more often used with VL.

This figure presents the proportion of intubations using the videolaryngoscope (VL) per participating site.
Videolaryngoscope use and neonatal intubation outcomes
In the univariate analysis, VL use was associated with higher first attempt success (58% with VL vs. 47% with DL; p < 0.001), lower occurrence of adverse TIAEs (7% with VL vs. 23% with DL, p < 0.001), and lower number of intubation attempts (median 1, interquartile range: IQR 1-2 with VL and 2, IQR 1-3 with DL, p < 0.001), Table 3. The occurrence of severe desaturation was not significantly different (47% with VL vs. 50% with DL, p = 0.098). Among TIAEs, esophageal intubation with either immediate or delayed recognition was more frequent with DL than with VL (Table 4).
After adjusting for covariates, VL use was not associated with higher first attempt success (adjusted Odds Ratio (aOR) 1.18, 95% CI: 0.95–1.47, p = 0.136, Supplemental Table B), but was associated with lower TIAEs (aOR 0.45, 95% CI: 0.31–0.64, p < 0.001, Supplemental Table C). In sensitivity analysis of NICUs with >10 VL TIs (4 NICUs, n = 1469), the aOR were similar for the first attempt success (aOR 1.19, 95% CI 0.93–1.52, p = 0.169), and for the occurrence of TIAEs (aOR 0.43, 95% CI 0.29–0.64, p < 0.001).
In subgroup analysis of tracheal intubations using the videolaryngoscope, use of indirect view (video image) was associated with higher first attempt success (62% with indirect view vs. 54% with direct view; p = 0.043), similar occurrence of adverse TIAEs (6% with indirect view vs. 8% with direct view, p = 0.339), similar number of intubation attempts (median 1, interquartile range: IQR 1-2 with indirect and direct view, p = 0.193), and lower occurrence of severe desaturation (42% with indirect view vs. 53% with direct view, p = 0.025, Supplemental Table D).
Discussion
In this large retrospective study of TIs in 13 NICUs, we evaluated the use and clinical impact of using VL for neonatal TI. We found that only approximately one quarter of TIs were done with VL and its use varied significantly across sites. It was most often used in larger, more mature and older babies, and in those that had a congenital or craniofacial anomaly. After adjusting for covariates, VL use was not associated with higher first attempt success, however it was associated with lower TIAEs.
Our first finding is that VL is seldom used for neonatal TI and its use varies across centers. The benefit in using VL for trainees has been greatly described in three clinical trials showing improved first attempt success rate without increasing time to intubation [14,15,16, 18]. Trainees describe that VL use allowed for better guidance from supervisors throughout the procedure and that it improved their confidence [15, 19]. In our study, as residents attempted only 13% of intubations, VL was also used for TIs performed by other categories of providers. A recent telephone survey study in the United Kingdom identified that 63% of the 169 NICUs surveyed had VL in their unit. Of these, 60% used VL for TIs performed by trainees, 31% as the primary device for all TIs and 63% as a rescue device if initial TI attempt was unsuccessful [20]. The most common obstacles for VL use were lack of confidence and training for all providers and reluctance to move away from the traditional laryngoscope. Depending on the type of VL used in a unit, the size of the baby might be another limiting factor. Indeed, the C-MAC VL (Karl Storz ©,Tuttlingen, Germany) does not have a 00 blade and thus prohibits its use in the smallest babies. Increasing VL use has been described in neonatal and pediatric critical care transport teams [21]. Use of VL has been well established in adults for normal, difficult and emergency TIs [22] and has gained popularity during the COVID-19 pandemic when it was frequently utilized as the first-line device for TI in pediatric and adult patients with suspected or confirmed infection [23]. We expect that over time, allowing for increased training and improvement in providers’ confidence, as well as the growing body of evidence to support its benefit, use of VL for neonatal TI will increase.
Our second finding was that VL was used in more mature, larger, and older babies, and in babies with congenital or craniofacial anomalies. Kaplan et al. initially described the use of VL by experienced laryngoscopists in adult patients in whom TI was anticipated to be difficult [5]. Since, the VL has become widely used for anticipated or confirmed difficult intubations in adults, children and newborn [20, 22, 24]. The VL used in the majority of the NICUs in this study is the C-MAC VL (Karl Storz ©,Tuttlingen, Germany) which currently offers Miller blades 0 and 1. Although preliminary experience has shown C-MAC VL use in newborns as small as 530 g [13], the smallest infant intubated in a previous clinical trial was 740 g [15]. The main reason for the weight limit in this trial was related to VL size. The smallest blade (Miller 0) was reportedly too large for the patient’s mouth, resulting in limited space to insert an endotracheal tube. Therefore, it makes sense that VL would be used in more mature, larger, and older babies. In another clinical trial using the Laryflex VL (Laryflex©, Acutronics, Hirzel, Switzerland), which has a 00 blade, the smallest infant intubated was 500 g [14]. Recently, some NICUs are acquiring the Neoview (International Biomedical ©, Austin, Texas, USA) which offers miller blades 000, 00, 0 and 1. This might change the patient population in which VL is used for TI.
Our third finding was that VL use was not associated with higher first attempt success. To our knowledge, this is the first study evaluating VL use by all neonatal providers. In neonates, three clinical trials and a meta-analysis have shown that VL use in trainees is associated with higher first attempt success rate [14,15,16, 18]. In the pediatric population, however, data regarding first attempt success rate using VL is not consistent. Previous studies have demonstrated conflicting results of VL use, with both improvement [25] and lack of improvement in first attempt success in infants and/ or children [26, 27]. Adult studies demonstrated VL improved success rates in patients with difficult airways, but not in those with anatomically normal airways [28].
Our fourth finding was that VL use was associated with lower TIAEs. This is consistent with a recently published single-site observational study by Tippmann et al. where VL use was predictive of an intubation encounter without TIAEs [29]. Our study adds strength to this finding with its larger sample size and multicenter design. One may assume this is because a VL device offers a greater angle of glottic exposure, improved visualization, and easy identification of an esophageal intubation [30, 31]. Previous studies have demonstrated that difficulty visualizing or recognizing the glottis and resultant esophageal intubation are the most common reasons of intubation failure in trainees [15, 31] Our group has also previously demonstrated that the most common TIAE on which VL has an impact is esophageal intubation [32]. Therefore, it stands to reason that by using VL, reducing frequency of esophageal intubation may significantly decrease TIAEs overall [2].
This study has limitations. First, this was a retrospective study subject to selection bias. We attempted to account for the source of bias due to unbalanced patient characteristics using multivariable logistic regression and sensitivity analysis. Second, our study included NICU intubation data from only 13 NICUs and the majority of participating NICUs were within academic institutions. Therefore, our findings may not be generalizable to all NICUs. Third, this analysis used intubation data, which was self-reported by the team at the time of intubation and therefore may be influenced by reporting bias. The NEAR4NEOS collaborative has implemented universal operational definitions and data coordinator education to minimize these reporting bias across the sites.
In this large, multicenter, retrospective study, VL was used in 23% of intubations and its use varied across sites. VL was used more frequently in more mature, larger, and older neonates. VL use was not associated with higher first attempt success, but was associated with lower TIAEs. This is the first study to show patient benefit associated with the use of VL in neonatal TI performed by all neonatal providers. Although clinicians seem to gain experience and confidence in using VL and there is moderate evidence of benefit for trainees learning neonatal TI, its benefits for all neonatal providers, including more senior healthcare professionals, should be studied in a prospective clinical trial.
Data availability
The datasets analysed during the current study are available from the corresponding author on reasonable request.
References
Hatch LD, Grubb PH, Lea AS, Walsh WF, Markham MH, Whitney GM, et al. Endotracheal Intubation in Neonates: A Prospective Study of Adverse Safety Events in 162 Infants. J Pediatr. 2016;168:62–6.e66.
Foglia EE, Ades A, Sawyer T, Glass KM, Singh N, Jung P, et al. Neonatal Intubation Practice and Outcomes: An International Registry Study. Pediatrics 2019;143:e20180902.
Haubner LY, Barry JS, Johnston LC, Soghier L, Tatum PM, Kessler D, et al. Neonatal intubation performance: room for improvement in tertiary neonatal intensive care units. Resuscitation. 2013;84:1359–64.
Page NE, Giehl M, Luke S. Intubation complications in the critically ill child. AACN Clin Issues. 1998;9:25–35.
Kaplan MB, Ward DS, Berci G. A new video laryngoscope-an aid to intubation and teaching. J Clin Anesth. 2002;14:620–6.
Weiss M, Schwarz U, Dillier CM, Gerber AC. Teaching and supervising tracheal intubation in paediatric patients using videolaryngoscopy. Paediatr Anaesth. 2001;11:343–8.
Vlatten A, Aucoin S, Litz S, Macmanus B, Soder C. A comparison of the STORZ video laryngoscope and standard direct laryngoscopy for intubation in the Pediatric airway - a randomized clinical trial. Pediatr Anesthesia. 2009;19:1102–7.
Fiadjoe JE, Kovatsis P. Videolaryngoscopes in pediatric anesthesia: What’s new? Minerva anestesiologica. 2014;80:76–82.
Vanderhal AL, Berci G, Simmons CF, Hagiike M. A Videolaryngoscopy Technique for the Intubation of the Newborn: Preliminary Report. Pediatrics. 2009;124:e339–46.
Vanderhal AL, Berci G, Simmons CF. Video Assisted Endotracheal Intubation: Role in Teaching and Acquiring Skills in Era of Decreasing DR and NICU Time during Residency Training. E-PAS2007:617907.2; 2007.
Donoghue AJ, Ades AM, Nishisaki A, Deutsch ES. Videolaryngoscopy versus direct laryngoscopy in simulated pediatric intubation. Ann Emerg Med. 2013;61:271–7.
Assaad M-A, Lachance C, Moussa A. Learning neonatal intubation using the videolaryngoscope: A randomized trial on mannequins. Simul Healthc. 2016;11:190–3.
Vanderhal AL, Berci G, Simmons CF Jr, Hagiike M. A videolaryngoscopy technique for the intubation of the newborn: Preliminary report. Pediatrics 2009;124:e339–346.
O’Shea JE, Thio M, Kamlin CO, McGrory L, Wong C, John J, et al. Videolaryngoscopy to teach neonatal intubation: A randomized trial. Pediatrics 2015;136:912–9.
Moussa A, Luangxay Y, Tremblay S, Lavoie J, Aube G, Savoie E, et al. Videolaryngoscope for teaching neonatal endotracheal intubation: A randomized controlled trial. Pediatrics 2016;137:e20152156.
Volz S, Stevens TP, Dadiz R. A randomized controlled trial: does coaching using video during direct laryngoscopy improve residents’ success in neonatal intubations? J Perinatol. 2018;38:1074–80.
Patel J, Posencheg M, Ades A. Proficiency and retention of neonatal resuscitation skills by pediatric residents. Pediatrics 2012;130:515–21.
Lingappan K, Arnold JL, Fernandes CJ, Pammi M. Videolaryngoscopy versus direct laryngoscopy for tracheal intubation in neonates. Cochrane Database Syst Rev. 2018;6:CD009975.
O’Shea JE, Kirolos S, Thio M, Kamlin COF, Davis PG. Neonatal videolaryngoscopy as a teaching aid: the trainees’ perspective. Arch Dis Child Fetal Neonatal Ed. 2021;106:168–71.
Thomas H, Lugg R, James B, Geeroms C, Risbridger A, Bell R, et al. Survey of the use of videolaryngoscopy in neonatal units in the UK. Arch Dis Child Fetal Neonatal Ed. 2021:fetalneonatal-2021-322813. https://doi.org/10.1136/archdischild-2021-322813.
Abid ES, McNamara J, Hall P, Miller KA, Monuteaux M, Kleinman ME, et al. The Impact of Videolaryngoscopy on Endotracheal Intubation Success by a Pediatric/Neonatal Critical Care Transport Team. Prehosp Emerg Care. 2021;25:325–32.
Xue FS, Li HX, Liu YY, Yang GZ. Current evidence for the use of C-MAC videolaryngoscope in adult airway management: a review of the literature. Ther Clin Risk Manag. 2017;13:831–41.
Cook TM, El-Boghdadly K, McGuire B, McNarry AF, Patel A, Higgs A. Consensus guidelines for managing the airway in patients with COVID-19: Guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists. Anaesthesia 2020;75:785–99.
Fiadjoe J, Nishisaki A. Normal and difficult airways in children: “What’s New”-Current evidence. Paediatr Anaesth. 2020;30:257–63.
Garcia-Marcinkiewicz AG, Kovatsis PG, Hunyady AI, Olomu PN, Zhang B, Sathyamoorthy M, et al. First-attempt success rate of video laryngoscopy in small infants (VISI): a multicentre, randomised controlled trial. Lancet 2020;396:1905–13.
Hu X, Jin Y, Li J, Xin J, Yang Z. Efficacy and safety of videolaryngoscopy versus direct laryngoscopy in paediatric intubation: A meta-analysis of 27 randomized controlled trials. J Clin Anesth. 2020;66:109968.
Klabusayová E, Klučka J, Kosinová M, Ťoukálková M, Štoudek R, Kratochvíl M, et al. Videolaryngoscopy vs. Direct Laryngoscopy for Elective Airway Management in Paediatric Anaesthesia: A prospective randomised controlled trial. Eur J Anaesthesiol. 2021;38:1187–93.
Hoshijima H, Mihara T, Maruyama K, Denawa Y, Mizuta K, Shiga T, et al. C-MAC videolaryngoscope versus Macintosh laryngoscope for tracheal intubation: A systematic review and meta-analysis with trial sequential analysis. J Clin Anesth. 2018;49:53–62.
Tippmann S, Haan M, Winter J, Mühler AK, Schmitz K, Schönfeld M, et al. Adverse events and unsuccessful intubation attempts are frequent during neonatal nasotracheal intubations. Front Pediatr. 2021;9:675238.
Vlatten A, Aucoin S, Litz S, Macmanus B, Soder C. A comparison of the STORZ video laryngoscope and standard direct laryngoscopy for intubation in the Pediatric airway-a randomized clinical trial. Paediatr Anaesth. 2009;19:1102–7.
O’Shea JE, Loganathan P, Thio M, Kamlin COF, Davis PG. Analysis of unsuccessful intubations in neonates using videolaryngoscopy recordings. Arch Dis Child Fetal Neonatal Ed. 2018;103:F408–12.
Pouppirt NR, Nassar R, Napolitano N, Nawab U, Nishisaki A, Nadkarni V, et al. Association between video laryngoscopy and adverse tracheal intubation-associated events in the neonatal intensive care unit. J Pediatr. 2018;201:281–4 e281.
Acknowledgements
The authors would like to thank the healthcare teams at participating NEAR4NEOS sites for their diligent completion of NEAR4NEOS data collection forms. They also like to thank Hayley Buffman at Children’s Hospital of Philadelphia as a coordinator for the NEAR4NEOS collaborative.
Funding
This study was supported by Eunice Kennedy Shriver NICHD R21 HD089151.
Author information
Authors and Affiliations
Consortia
Contributions
AM has contributed to conception and design, acquisition of data, analysis and interpretation of data. He has written the first draft of this specific article and modified subsequent drafts until all authors approved the final version of the article. TJ, MPD, EEF, AA, NN, KMG, LJ, PJ, NS, BHQ, JB, JZ, SD, AAM and VN have contributed to acquisition of data and revised the article critically for important intellectual content. AN has contributed to conception and design, acquisition of data, analysis and interpretation of data; and revised the article critically for important intellectual content. All authors agree to be accountable for all aspects of the work. They ensure that questions relating to accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors have approved the final version of the article as sent to Journal of Perinatology.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Moussa, A., Sawyer, T., Puia-Dumitrescu, M. et al. Does videolaryngoscopy improve tracheal intubation first attempt success in the NICUs? A report from the NEAR4NEOS. J Perinatol 42, 1210–1215 (2022). https://doi.org/10.1038/s41372-022-01472-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-022-01472-9
This article is cited by
-
Factors that determine first intubation attempt success in high-risk neonates
Pediatric Research (2024)
-
Manikin to patient intubation: does it translate?
Journal of Perinatology (2023)
