
Abstract
Understanding human behaviour is essential to the successful adoption of new technologies, and for the promotion of safer care. This requires capturing the detail of clinical workflows to inform the design of new human–technology interactions. We are interested particularly in the possibilities for touchless technologies that can decipher human speech, gesture and motion and allow for interactions that are free of contact. Here, we employ a new approach by installing a single 360° camera into a clinical environment to analyse touch patterns and human–environment interactions across a clinical team to recommend design considerations for new technologies with the potential to reduce avoidable touch.
Similar content being viewed by others


There is increasing interest in how healthcare workers interact with technology and the cognitive processes that underpin these interactions. One example is gesture-based control of image manipulation within medical scans [1], but many other healthcare settings involve complex human/technology interactions. While medical devices and information technologies continue to improve outcomes, their proliferation has reduced standardisation compared to other safety-critical industries, which has implications for team performance and potentially patient outcomes.
Human factors and ergonomic (HFE) principles arose from endeavours to improve the safety of military and transport systems and are also important in understanding human–environment interactions in healthcare [2]. Our focus is on human/technology interactions within the neonatal intensive care unit (NICU) [3], wherever more sophisticated technology is regularly introduced.
Clinical simulation offers an ideal approach to examine interactions in an acute clinical scenario in a safe and controlled setting. The scenario can be observed using an unobtrusive 360° camera and viewed on a 360° media player using a virtual reality (VR) headset. The remote but immersive observation of a clinical team managing a high-fidelity simulation of a deteriorating preterm infant provides a new perspective to consider optimum conditions for the touchless technologies with the potential to reduce avoidable touch, whilst minimising the effect of an observer’s presence.
A clinical team (three nurses, one doctor; all-female) participated in a simulated scenario lasting 17 min. Analysis revealed 437 episodes and 68 sequence pairs of touch across 17 surfaces. Touch patterns differed across the clinical team, who worked in pairs as a safety system to identify, investigate, manage and record the clinical deterioration. Assessment of vital signs, clinical examination, and equipment for ultrasound and transillumination was contained in a restricted incubator space, interrupted by retrieval of equipment requiring assembly and disassembly and diversions of focus to multiple in-room monitors. At a second focal point, medication preparation involves hand-offs of medications and ancillaries and manual initiation of infusion pumps.
We developed a coding system comprising sequences and episodes of touch enabling classifications of human–environment interactions. This included recording touch frequency by a single touch, sequential touch incidents and patterns of touch across individual team members. From this, we developed a classification of avoidable touch during tasks. Four types of potentially avoidable touch were analysed: ‘repeated touch’, ‘obstructions to touch’ ‘touch that cause delays’ and ‘unplanned touch’. Unavoidable touch for care provision was also identified.
This preliminary study of a high-fidelity simulation representative of a clinical environment characterised by complex and frequent flows of decisions focused on the translation of hand touch patterns across a clinical team. Detailed touch analysis of a simulated clinical scenario enabled exploration of the implications of different configurations of touchless technologies were introduced, with potential positive impacts on efficiency, effectiveness, and potential for infection transmission [4]. This study also highlighted the importance of understanding team behaviours in terms of interactions that make up clinical workflows, as well as traditional ergonomic aspects of the environment, such as effective use of space, suitable lighting, minimising obstructions and limiting ambient noise to improve integration as summarised in Fig. 1. It suggests that new technology must also match the reliability of traditional methods and add value to the clinical team as part of a clinical workflow.

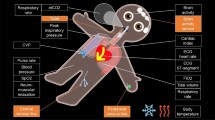
(a) Aerial placement of a 360° camera in NICU to emulate the viewpoint of an observer, to conduct an interaction analysis including touch frequency, as illustrated by (b) Sankey chart of the top 10 most commonly touched equipment by the individual, accounting for 410 of the episodes of touch, and thereafter to infer (c) optimal conditions for touchless technologies by space, lighting, obstructions, and ambient noise in NICU (SLOAN framework) EHR refers to Electronic Health Record and PACS refers to Picture archiving and communications system. *Derived from White [5].
Touch forms the basis of the relationship between healthcare workers, their tasks, the tools they use, and the physical environment they work in. This analysis of touch patterns offers new insight into the working of clinical teams using an unobtrusive 360° camera to capture and enable rich touch pattern analysis. It provides a potential paradigm for future evaluations of healthcare environments when assessing the potential of new technologies for healthcare.
References
Madapana N, Gonzalez G, Rodgers R, Zhang L, Wachs JP. Gestures for Picture Archiving and Communication Systems (PACS) operation in the operating room: is there any standard? PLoS ONE. 2018;13:e0198092.
Carayon P, Wetterneck TB, Rivera-Rodriguez AJ, Hundt AS, Hoonakker P, Holden R, et al. Human factors systems approach to healthcare quality and patient safety. Appl Ergon. 2014;45:14–25.
Ferris TK, Shepley MM. The design of neonatal incubators: a systems-oriented, human-centered approach. J Perinatol. 2013;33:S24–S31.
Trudel C, Cobb S, Momtahan K, Brintnell J, Mitchell A. Disconnects in design and infection prevention and control—how the design of products and the environment in neonatal intensive care may be undermining infection prevention practice. Proc Int Symp Hum Factors Ergon Health Care. 2016;5:44–9.
White RD. Recommended standards for newborn ICU design, 9th edition. J Perinatol. 2020;40:2–4.
Funding
SV acknowledges doctoral funding from Great Ormond Street Hospital for children Charity. This study was approved for ethics by University College London under REC ID: 18579.001.
Author information
Authors and Affiliations
Contributions
SV, PN conceived the project. LP, EB, LC were involved with the simulation design. LP led the simulation session and filming. SV provided the camera equipment, conducted the analysis and reported on findings creating Fig. 1. NJS, YR provided supervisory oversight of the project and revisions on early drafts of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Visram, S., Potts, L., Sebire, N.J. et al. Making the invisible visible: New perspectives on the intersection of human–environment interactions of clinical teams in intensive care. J Perinatol 42, 503–504 (2022). https://doi.org/10.1038/s41372-021-01160-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-021-01160-0
