
Abstract
Objective
Delivery room (DR) continuous positive airway pressure (CPAP) is increasing. Our study examined the risk for neonatal morbidities after DR CPAP in 35 week neonates.
Study design
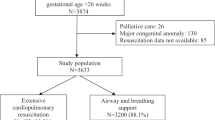
A retrospective study of 259 infants born at 35 weeks gestational age between January 1, 2017–December 31, 2018 at a single center.
Results
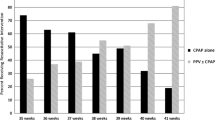
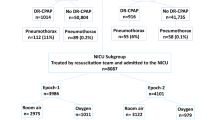
DR resuscitation was administered in 30.5%, with 19.7% receiving CPAP alone. Eighty percent who received DR CPAP were admitted to the NICU. DR CPAP was associated with the highest NICU admission risk, 9.3 times the risk of those without DR positive pressure, and with respiratory conditions (RDS: OR 4.22 {CI 1.46–11.51}, TTN: OR 3.30 {CI 1.36–7.64}). For the DR CPAP group, non-invasive positive pressure was administered post resuscitation in 90%.
Conclusions
In our institution, 35 week infants frequently received DR CPAP. Of these infants, a majority were admitted to the NICU for respiratory disorders.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others
References
Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993–2012. JAMA. 2015;314:1039–51.
Smithhart W, Wyckoff MH, Kapadia V, Jaleel M, Kakkilaya V, Brown LS, et al. Delivery room continuous positive airway pressure and pneumothorax. Pediatrics. 2019;144:e20190756.
Roberts CL, Badgery-Parker T, Algert CS, Bowen JR, Nassar N. Trends in use of neonatal CPAP: a population-based study. BMC Pediatr. 2011;11:89.
Gregory GA, Kitterman JA, Phibbs RH, Tooley WH, Hamilton WK. Treatment of the idiopathic respiratory-distress syndrome with continuous positive airway pressure. N. Engl J Med. 1971;284:1333–40.
Weiner GM. Textbook of neonatal resuscitation. 7th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2016.
Fischer HS, Buhrer C. Avoiding endotracheal ventilation to prevent bronchopulmonary dysplasia: a meta-analysis. Pediatrics. 2013;132:e1351–60.
Subramaniam P, Ho JJ, Davis PG. Prophylactic nasal continuous positive airway pressure for preventing morbidity and mortality in very preterm infants. Cochrane Database Syst Rev. 2016;6:CD001243.
Stevens TP, Finer NN, Carlo WA, Szilagyi PG, Phelps DL, Walsh MC, et al. Respiratory outcomes of the surfactant positive pressure and oximetry randomized trial (SUPPORT). J Pediatr. 2014;165:240–9.
Martin JA, Hamilton BE, Osterman MJK, Driscoll AK. National vital statistic reports, volume 68, Number 13. Births: final data for 2018. Natl Vital Stat Rep. 2019;68:1–47.
Martin J, Osterman MJK. Describing the Increase in Preterm Births in the United States, 2014–2016. Natl Center Health Stat Data Brief. 2018;312:1–8.
Pelaia P. Vermont Oxford Network: Manual of Operations, Part 2, Release 21.0. Burlington, VT: Vermont Oxford Network; 2017.
Stroustrup A, Trasande L, Holzman IR. Randomized controlled trial of restrictive fluid management in transient tachypnea of the newborn. J Pediatr. 2012;160:38–43.
Committee on F, Newborn, Adamkin DH. Postnatal glucose homeostasis in late-preterm and term infants. Pediatrics. 2011;127:575–9.
Fenton TR, Nasser R, Eliasziw M, Kim JH, Bilan D, Sauve R. Validating the weight gain of preterm infants between the reference growth curve of the fetus and the term infant. BMC Pediatr. 2013;13:92.
Hibbard JU, Wilkins I, Sun L, Gregory K, Haberman S, Hoffman M, et al. Respiratory morbidity in late preterm births. JAMA. 2010;304:419–25.
Escobar GJ, Clark RH, Greene JD. Short-term outcomes of infants born at 35 and 36 weeks gestation: we need to ask more questions. Semin Perinatol. 2006;30:28–33.
Shapiro-Mendoza CK, Tomashek KM, Kotelchuck M, Barfield W, Nannini A, Weiss J, et al. Effect of late-preterm birth and maternal medical conditions on newborn morbidity risk. Pediatrics. 2008;121:e223–32.
Raju TN. Late-preterm births: challenges and opportunities. Pediatrics. 2008;121:402–3.
Fleming PF, Arora P, Mitting R, Aladangady N. A national survey of admission practices for late preterm infants in England. BMC Pediatr. 2014;14:150.
Ringer SA, Aziz K. Neonatal stabilization and postresuscitation care. Clin Perinatol. 2012;39:901–18.
Gyamfi-Bannerman C, Zupancic JAF, Sandoval G, Grobman WA, Blackwell SC, Tita ATN, et al. Cost-effectiveness of antenatal corticosteroid therapy vs no therapy in women at risk of late preterm delivery: a secondary analysis of a randomized clinical trial. JAMA Pediatr. 2019;173:462–8.
Akinloye O, O’Connell C, Allen AC, El-Naggar W. Post-resuscitation care for neonates receiving positive pressure ventilation at birth. Pediatrics. 2014;134:e1057–62.
Frazier MD, Werthammer J. Post-resuscitation complications in term neonates. J Perinatol. 2007;27:82–4.
Escobar GJ, Greene JD, Hulac P, Kincannon E, Bischoff K, Gardner MN, et al. Rehospitalisation after birth hospitalisation: patterns among infants of all gestations. Arch Dis Child. 2005;90:125–31.
Kuzniewicz MW, Parker SJ, Schnake-Mahl A, Escobar GJ. Hospital readmissions and emergency department visits in moderate preterm, late preterm, and early term infants. Clin Perinatol. 2013;40:753–75.
Shapiro-Mendoza CK, Tomashek KM, Kotelchuck M, Barfield W, Weiss J, Evans S. Risk factors for neonatal morbidity and mortality among “healthy,” late preterm newborns. Semin Perinatol. 2006;30:54–60.
Spillane NT, Chivily C, Andrews T. Short term outcomes in term and late preterm neonates admitted to the well-baby nursery after resuscitation in the delivery room. J Perinatol. 2019;39:983–9.
Sharma D, Padmavathi IV, Tabatabaii SA, Farahbakhsh N. Late preterm: a new high risk group in neonatology. J Matern Fetal Neonatal Med. 2019;1:1–14.
Hansen AK, Wisborg K, Uldbjerg N, Henriksen TB. Elective caesarean section and respiratory morbidity in the term and near-term neonate. Acta Obstet Gynecol Scand. 2007;86:389–94.
Levine EM, Ghai V, Barton JJ, Strom CM. Mode of delivery and risk of respiratory diseases in newborns. Obstet Gynecol. 2001;97:439–42.
De Luca R, Boulvain M, Irion O, Berner M, Pfister RE. Incidence of early neonatal mortality and morbidity after late-preterm and term cesarean delivery. Pediatrics. 2009;123:e1064–71.
Acknowledgements
Elli Gourna Paleoudis, PhD for her assistance in protocol development and IRB submission.
Author information
Authors and Affiliations
Contributions
Dr. Nicole Spillane conceptualized and designed the study, analyzed data, performed statistical analyses, and drafted the initial manuscript and reviewed and revised the manuscript. Francesca Macalintal designed data collection instruments, performed data collection, carried out initial analyses, and critically reviewed the manuscript. Dr. Themba Nyirenda provided biostatistical support, assisted in study design, and critically reviewed the manuscript. Dr. Sergio Golombek interpreted data and critically reviewed and revised the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest or financial disclosures relevant to this article to disclose. This study was approved by the IRB of Hackensack University Medical Center and a waiver of consent and assent was granted. It was performed in accordance with the Declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Spillane, N.T., Macalintal, F., Nyirenda, T. et al. What happens to 35 week infants that receive delivery room continuous positive airway pressure?. J Perinatol 41, 1575–1582 (2021). https://doi.org/10.1038/s41372-020-00883-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-020-00883-w
This article is cited by
-
Association of delayed initiation of non-invasive respiratory support with pulmonary air leakage in outborn late-preterm and term neonates
European Journal of Pediatrics (2022)
