
Abstract
Background
Judicious use of antibiotic therapy in preterm infants is necessary as prolonged and unwarranted use of antibiotics have been associated with adverse short-term and long-term outcomes.
Local problem
Our baseline data review revealed overuse and unnecessary prolonged antibiotic exposure among preterm infants despite a low suspicion for sepsis.
Methods and interventions
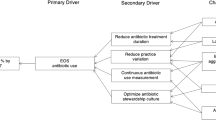
The baseline overall AUR was calculated retrospectively from our pharmacy database for a period of 4 months prior to the quality improvement (QI) initiative (pre-QI phase). The principal QI intervention included the development and implementation of guidance algorithms for evaluation and management of suspected sepsis incorporating key QI measures, such as an emphasis on early discontinuation of antibiotics by 36 h if blood culture remained negative and the introduction of multiplex polymerase chain reaction assay for early identification of causative organisms. This QI initiative was implemented through multiple Plan-Do-Study-Act cycles, starting in February 2016 (QI phase), with an objective to achieve a 10% reduction in the baseline overall AUR by December 2016, in preterm infants with gestational ages between 250/7 and 336/7 weeks. Data for the QI phase of the study were collected prospectively.
Result
The overall AUR (outcome measure) decreased from 154.8 to 138.4 days of treatment per 1000 hospital days (10.6% decrease, p < 0.05) over the 11-month period. However, the overall rate of adherence to guidance algorithm (process measure) remained below the target goal of 90%.
Conclusion
This multiphase QI initiative was able to reduce the overall AUR at our NICU. The beneficial impact of this decrease in AUR in preterm infants remains to be determined.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others

References
Hsieh EM, Hornik CP, Clark RH, Laughon MM, Benjamin DK Jr, Smith PB, Best Pharmaceuticals for Children Act—Pediatric Trials Network. Medication use in the neonatal intensive care unit. Am J Perinatol. 2014;31:811–21.
Clark RH, Bloom BT, Spitzer AR, Gerstmann DR. Reported medication use in the neonatal intensive care unit: data from a large national data set. Pediatrics. 2006;117:1979–87.
Fanaroff AA, Korones SB, Wright LL, Verter J, Poland RL, Bauer CR, et al. Incidence, presenting features, risk factors and significance of late onset septicemia in very low birth weight infants. The National Institute of Child Health and Human Development Neonatal Research Network. Pediatr Infect Dis J. 1998;17:593–8.
Polin RA, Committee on Fetus and Newborn. Management of neonates with suspected or proven early-onset bacterial sepsis. Pediatrics. 2012;129:1006–15.
Schelonka RL, Chai MK, Yoder BA, Hensley D, Brockett RM, Ascher DP. Volume of blood required to detect common neonatal pathogens. J Pediatr. 1996;129:275–8.
Ottolini MC, Lundgren K, Mirkinson LJ, Cason S, Ottolini MG. Utility of complete blood count and blood culture screening to diagnose neonatal sepsis in the asymptomatic at risk newborn. Pediatr Infect Dis J. 2003;22:430–4.
Spitzer AR, Kirkby S, Kornhauser M. Practice variation in suspected neonatal sepsis: a costly problem in neonatal intensive care. J Perinatol. 2005;25:265–69.
Schulman J, Dimand RJ, Lee HC, Duenas GV, Bennett MV, Gould JB. Neonatal intensive care unit antibiotic use. Pediatrics. 2015;135:826–33.
Greenwood C, Morrow AL, Lagomarcino AJ, Altaye M, Taft DH, Yu Z, et al. Early empiric antibiotic use in preterm infants is associated with lower bacterial diversity and higher relative abundance of Enterobacter. J Pediatr. 2014;165:23–29.
Cotten CM, Taylor S, Stoll B, Goldberg RN, Hansen NI, Sánchez PJ, et al. Prolonged duration of initial empirical antibiotic treatment is associated with increased rates of necrotizing enterocolitis and death for extremely low birth weight infants. Pediatrics. 2009;123:58–66.
Kuppala VS, Meinzen-Derr J, Morrow AL, Schibler KR. Prolonged initial empirical antibiotic treatment is associated with adverse outcomes in premature infants. J Pediatr. 2011;159:720–5.
Ting JY, Synnes A, Roberts A, Deshpandey A, Dow K, Yoon EW, et al. Association between antibiotic use and neonatal mortality and morbidities in very low-birth-weight infants without culture-proven sepsis or necrotizing enterocolitis. JAMA Pediatr. 2016;170:1181–7.
Laxminarayan R, Duse A, Wattal C, Zaidi AK, Wertheim HF, Sumpradit N, et al. Antibiotic resistance-the need for global solutions. Lancet Infect Dis. 2013;13:1057–98.
Haimi-Cohen Y, Shafinoori S, Tucci V, Rubin LG. Use of incubation time to detection in BACTEC 9240 to distinguish coagulase-negative staphylococcal contamination from infection in pediatric blood cultures. Pediatr Infect Dis J. 2003;22:968–74.
Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, et al. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics. 2002;110:285–91.
Salimnia H, Fairfax MR, Lephart PR, Schreckenberger P, DesJarlais SM, Johnson JK, et al. Evaluation of the FilmArray blood culture identification panel: results of a multicenter controlled trial. J Clin Microbiol. 2016;54:687–98.
Leber AL, Everhart K, Balada-Llasat JM, Cullison J, Daly J, Holt S, et al. Multicenter evaluation of BioFire FilmArray meningitis/encephalitis panel for detection of bacteria, viruses, and yeast in cerebrospinal fluid specimens. J Clin Microbiol. 2016;54:2251–61.
Kumar Y, Qunibi M, Neal TJ, Yoxall CW. Time to positivity of neonatal blood cultures. Arch Dis Child Fetal Neonatal Ed. 2001;85:F182–6.
Garcia-Prats JA, Cooper TR, Schneider VF, Stager CE, Hansen TN. Rapid detection of microorganisms in blood cultures of newborn infants utilizing an automated blood culture system. Pediatrics. 2000;105:523–7.
National Institute for Heath and Care Excellence. Antibiotics for early-onset neonatal infection: antibiotics for the prevention and treatment of early-onset neonatal infection. London: NICE 2012. http://www.nice.org.uk/cg149. Accessed 1 February 2016.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Ramachandra Bhat and Haidee Custodio contributed equally to this work.
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Bhat, R., Custodio, H., McCurley, C. et al. Reducing antibiotic utilization rate in preterm infants: a quality improvement initiative. J Perinatol 38, 421–429 (2018). https://doi.org/10.1038/s41372-018-0041-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-018-0041-y
