
Abstract
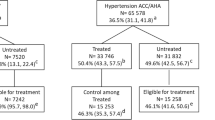
Hypertension is a major modifiable risk factor for cardiovascular disease. Autoimmune rheumatic diseases confer increased cardiovascular risk, which is at least partially mediated by traditional cardiovascular risk factors. We examined the prevalence, awareness, treatment, and control rates of hypertension in a large cohort of patients with rheumatic diseases. Consecutive patients attending the Rheumatology Οutpatient Clinics were studied. Hypertension was defined by both the 2018 European Society of Cardiology/European Society of Hypertension (ESC/ESH) guidelines and the 2017 American College of Cardiology/American Heart Association (ACC/AHA). In a total of 622 individuals, hypertension prevalence reached 54.5% according to the 2018 ESH/ESC guideline, with the highest rates observed in patients with osteoarthritis (69.6%), rheumatoid arthritis (60.9%), and psoriatic arthritis (57.8%). Among hypertensive individuals, 21.7% were unaware of high blood pressure levels, while 67.2% were treated. Only 48.6% of treated hypertensives reached the 2018 ESC/ESH treatment goals. Applying the 2017 ACC/AHA criteria would result in a substantial increase of hypertension prevalence (72.4%) for both genders and especially among younger individuals, accompanied by a dramatic drop in control rates among treated patients (16.7%). In conclusion, comorbid hypertension was highly prevalent in a large cohort of patients with rheumatic diseases according to ESH/ESC and especially, ACC/AHA guidelines. However, it remains underdiagnosed and undertreated in a significant portion, while control rates are far from optimal. Our findings highlight the importance of systematic screening and more aggressive treatment of hypertension among patients with rheumatic diseases.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others


References
Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension–analysis of worldwide data. Lancet. 2005;365:217–23.
Zhou B, Bentham J, Di Cesare M, Bixby H, Danaei G, Cowan MJ, et al. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19.1 million participants. Lancet. 2017;389:37–55.
Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J. 2016;37:3232–45.
World Health Organization. A global brief on hypertension: silent killer, global public health crisis: World Health Day 2013. World Health Organization. 2013. http://www.who.int/iris/handle/10665/%0A79059.
Anyfanti P, Triantafyllou A, Gkaliagkousi E, Koletsos N, Athanasopoulos G, Zabulis X, et al. Retinal vessel morphology in rheumatoid arthritis: association with systemic inflammation, subclinical atherosclerosis and cardiovascular risk. Microcirculation. 2017;24. https://doi.org/10.1111/micc.12417.
Anyfanti P, Gkaliagkousi E, Triantafyllou A, Zabulis X, Dolgyras P, Galanopoulou V, et al. Dermal capillary rarefaction as a marker of microvascular damage in patients with rheumatoid arthritis: association with inflammation and disorders of the macrocirculation. Microcirculation. 2018;25:e12451.
Anyfanti P, Triantafyllou A, Gkaliagkousi E, Triantafyllou G, Koletsos N, Chatzimichailidou S, et al. Subendocardial viability ratio in patients with rheumatoid arthritis: comparison with healthy controls and identification of prognostic factors. Clin Rheumatol. 2017;36:1229–36.
Anyfanti P, Triantafyllou A, Gkaliagkousi E, Koletsos N, Aslanidis S, Douma S. Association of non-invasive hemodynamics with arterial stiffness in rheumatoid arthritis. Scand Cardiovasc J. 2018;52:171–6.
Anyfanti P, Gkaliagkousi E, Gavriilaki E, Triantafyllou A, Dolgyras P, Galanopoulou V, et al. Association of galectin-3 with markers of myocardial function, atherosclerosis, and vascular fibrosis in patients with rheumatoid arthritis. Clin Cardiol. 2018;42:62–8.
Alenghat FJ. The prevalence of atherosclerosis in those with inflammatory connective tissue disease by race, age, and traditional risk factors. Sci Rep. 2016;6:20303.
Bartoloni E, Alunno A, Gerli R. Hypertension as a cardiovascular risk factor in autoimmune rheumatic diseases. Nat Rev Cardiol. 2018;15:33–44.
Baghdadi LR, Woodman RJ, Shanahan EM, Mangoni AA. The impact of traditional cardiovascular risk factors on cardiovascular outcomes in patients with rheumatoid arthritis: a systematic review and meta-analysis. PLoS ONE. 2015;10:1–18.
Panoulas VF, Metsios GS, Pace AV, John H, Treharne GJ, Banks MJ, et al. Hypertension in rheumatoid arthritis. Rheumatology. 2008;47:1286–98.
Sattar N, Nurmohamed MT, Jamnitski A, MciInnes I, Symmons D, Peters MJL. Cardiovascular comorbidities in patients with psoriatic arthritis: a systematic review. Ann Rheum Dis. 2012;72:211–6.
Hanih M, Milas-Ahić J, Štiglić-Rogoznica N, Badovinac O, Novak S, Prus V, et al. Is the prevalence of arterial hypertension in rheumatoid arthritis and osteoarthritis associated with disease? Rheumatol Int. 2012;33:1185–92.
Thomas RJ, Jones DW, Ovbiagele B, Stafford RS, Spencer CC, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults. J Am Coll Cardiol. 2017;71:e127–248.
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension. J Hypertens. 2018;36:1953–2041.
Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Böhm M, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34:2159–219.
Muntner P, Carey RM, Gidding S, Jones DW, Taler SJ, Wright JT, et al. Potential U.S. population impact of the 2017 ACC/AHA high blood pressure guideline. J Am Coll Cardiol. 2018;71:109–18.
Li D, Zeng X, Huang Y, Lei H, Li G, Zhang N, et al. Increased risk of hypertension in young adults in Southwest China: impact of the 2017 ACC/AHA high blood pressure guideline. Curr Hypertens Rep. 2019;21:21.
Anyfanti P, Gavriilaki E, Pyrpasopoulou A, Triantafyllou G, Triantafyllou A, Chatzimichailidou S, et al. Depression, anxiety, and quality of life in a large cohort of patients with rheumatic diseases: common, yet undertreated. Clin Rheumatol. 2016;35. https://doi.org/10.1007/s10067-014-2677-0.
Anyfanti P, Pyrpasopoulou A, Triantafyllou A, Doumas M, Gavriilaki E, Triantafyllou G, et al. The impact of frequently encountered cardiovascular risk factors on sexual dysfunction in rheumatic disorders. Andrology. 2013;1:556–62.
Anyfanti P, Pyrpasopoulou A, Triantafyllou A, Triantafyllou G, Gavriilaki E, Chatzimichailidou S, et al. Association between mental health disorders and sexual dysfunction in patients suffering from rheumatic diseases. J Sex Med. 2014;11. https://doi.org/10.1111/jsm.12672.
Anyfanti P, Triantafyllou A, Panagopoulos P, Triantafyllou G, Pyrpasopoulou A, Chatzimichailidou S, et al. Predictors of impaired quality of life in patients with rheumatic diseases. Clin Rheumatol. 2016;35:1705–11.
Panoulas V, Douglas K, Milionis H, Stavropoulos-Kalinglou A, Nightingale P, Kita M, et al. Prevalence and associations of hypertension and its control in patients with rheumatoid arthritis. Rheumatology. 2007;46:1477–82.
Gonzalez A, Maradit Kremers H, Crowson C, Ballman K, Roger V, Jacobsen S, et al. Do cardiovascular risk factors confer the same risk for cardiovascular outcomes in rheumatoid arthritis patients as in non-rheumatoid arthritis patients? Ann Rheum Dis. 2008;67:64–9.
Chung CP, Oeser A, Solus JF, Avalos I, Gebretsadik T, Shintani A, et al. Prevalence of the metabolic syndrome is increased in rheumatoid arthritis and is associated with coronary atherosclerosis. Atherosclerosis. 2008;196:756–63.
Del Rincón I, Freeman GL, Haas RW, O’Leary DH, Escalante A. Relative contribution of cardiovascular risk factors and rheumatoid arthritis clinical manifestations to atherosclerosis. Arthritis Rheum. 2005;52:3413–23.
Cook MJ, Bellou E, Bowes J, Sergeant JC, O’Neill TW, Barton A, et al. The prevalence of co-morbidities and their impact on physical activity in people with inflammatory rheumatic diseases compared with the general population: results from the UK Biobank. Rheumatol. 2018;57:2172–82.
Jafri K, Bartels CM, Shin D, Gelfand JM, Ogdie A. The Incidence and management of cardiovascular risk factors in psoriatic arthritis and rheumatoid arthritis: a population-based study. Arthritis Care Res. 2017;69:51–7.
Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. Heart disease and stroke statistics—2018 update: a report from the American Heart Association. Circulation. 2018;137:e67–492.
Jaussent A, Picot M-C, Fesler P, Tubery A, Cohen J-D, du Cailar G, et al. Relevance and feasibility of a systematic screening of multimorbidities in patients with chronic inflammatory rheumatic diseases. Jt Bone Spine. 2018;86:49–54.
Castro LL, Lanna CCD, Rocha MP, Ribeiro ALP, Telles RW. Recognition and control of hypertension, diabetes, and dyslipidemia in patients with rheumatoid arthritis. Rheumatol Int. 2018;38:1437–42.
Van Breukelen-van der Stoep DF, Van Zeben D, Klop B, Van de Geijn GJM, Janssen HJW, Meulen Nvander, et al. Marked underdiagnosis and undertreatment of hypertension and hypercholesterolaemia in rheumatoid arthritis. Rheumatol. 2016;55:1210–6.
Bartels C, Roberts T, Hansen K, Jacobs E, Gilmore A, Maxcy C, et al. Rheumatologist and primary care management of cardiovascular disease risk in rheumatoid arthritis: patient and provider perspectives. Arthritis Care Res. 2016;68:415–23.
Protogerou AD, Panagiotakos DB, Zampeli E, Argyris AA, Arida K, Konstantonis GD, et al. Arterial hypertension assessed ‘out-of-office’ in a contemporary cohort of rheumatoid arthritis patients free of cardiovascular disease is characterized by high prevalence, low awareness, poor control and increased vascular damage-associated ‘white coat’. Arthritis Res Ther. 2013;15:R142.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was conducted in accordance with the Helsinki declaration and was approved by the institutional ethics committee.
Informed consent
Written informed consent was provided before inclusion in the study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Anyfanti, P., Gkaliagkousi, E., Triantafyllou, A. et al. Hypertension in rheumatic diseases: prevalence, awareness, treatment, and control rates according to current hypertension guidelines. J Hum Hypertens 35, 419–427 (2021). https://doi.org/10.1038/s41371-020-0348-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41371-020-0348-y
This article is cited by
-
Autonomic dysfunction and cardiovascular risk in psoriatic arthritis
Clinical Rheumatology (2023)
-
Hypertension in connective tissue disease
Journal of Human Hypertension (2022)
