
Abstract
Background
Previous studies demonstrated a relation between takeaway outlet exposure and health outcomes. Individual characteristics, such as eating behaviour traits, could make some people more susceptible to the influence of the food environment. Few studies have investigated this topic. We aimed to investigate the moderating role of eating behaviour traits (cognitive restraint, uncontrolled eating and emotional eating) in the association between neighbourhood exposure to hot food takeaway outlets (hereafter referred to as takeaway outlets), and takeaway food consumption and adiposity.
Methods
We used cross-sectional data from a cohort in Cambridgeshire, UK (The Fenland study). Takeaway outlet exposure was derived using participants’ residential address and data from local authorities and divided into quarters. The Three Factor Eating questionnaire (TFEQ-R18) was used to measure eating behaviour traits. Primary outcomes were consumption of takeaway-like foods (derived from food frequency questionnaire), and body fat percentage (measured using dual-energy X-ray absorptiometry).
Results
Mean age of participants (n = 4791) was 51.0 (SD = 7.2) and 53.9% were female. Higher exposure to takeaway outlets in the neighbourhood and higher eating behaviour trait scores were independently associated with greater takeaway consumption and body fat percentage. Uncontrolled eating did not moderate the associations between takeaway outlet exposure and takeaway consumption or body fat percentage. The association between takeaway outlet exposure and takeaway consumption was slightly stronger in those with higher cognitive restraint scores, and the association between takeaway outlet exposure and body fat percentage was slightly stronger in those with lower emotional eating scores.
Conclusion
Eating behaviour traits and exposure to takeaway outlets were associated with greater takeaway consumption and body fat, but evidence that individuals with certain traits are more susceptible to takeaway outlets was weak. The findings indicate that interventions at both the individual and environmental levels are needed to comprehensively address unhealthy diets.
Trial registry
ISRCTN72077169
Similar content being viewed by others

Introduction
The obesogenic environment has been defined as the “sum of the influences that the surroundings, opportunities or conditions of life have on promoting obesity in individuals and populations” [1]. It contributes to the prevalence of energy-dense food consumption, low levels of energy expenditure, and high levels of overweight and obesity in the United Kingdom (UK) and elsewhere [2]. One aspect of the obesogenic environment is easy access to hot food takeaway outlets (e.g. outlets selling hamburgers and fried chicken; hereafter referred to as takeaway outlets). The prevalence of takeaway outlets has increased significantly in recent years [3, 4]. Evidence from the UK suggests that between 1990 and 2008, takeaway outlets increased by 43% in the most deprived areas, 50% in middle deprived areas and 30% in the least deprived areas [4].
While the evidence base is generally inconclusive [5, 6], studies have found that physical exposure to takeaway outlets around where people live and work is associated with unhealthy dietary behaviour and greater body weight [7,8,9]. More specifically, in a previous analysis of 5442 adults living in Cambridgeshire, UK, we found that exposure to takeaway outlets was associated with greater consumption of takeaway food, higher body mass index (BMI) and greater odds of obesity [7].
Despite the presence of high numbers of takeaway outlets in their environment, some individuals are still able to eat well and maintain a healthy weight [10]. The inconsistent evidence surrounding the influence of the food environment on dietary behaviours and obesity may partly be due to a failure to consider how individual differences in psychological traits interact with food environments [11, 12]. For example, some individuals may be more susceptible to takeaway outlets as environmental “cues” to eat than others. A previous study found a positive association between exposure to takeaway outlets and fast-food consumption, but only among children with higher scores for external eating (a psychological trait characterised by a stronger response to food cues in the environment such as the sight or smell of food) [11].
Eating behaviour traits are characteristics of individuals that influence behaviour and do not tend to fluctuate on a day-to-day basis [10]. External eating is one example; other examples include those commonly measured using the revised Three-Factor Eating Questionnaire (TFEQ-R18) [13]. The TFEQ-R18 assesses one’s conscious and constant effort to restrict food intake to achieve a desirable weight (cognitive restraint), having a heightened appetite (uncontrolled eating) and eating in response to negative emotions (emotional eating) [13, 14]. Previous studies found that higher uncontrolled and emotional eating scores were associated with lower diet quality [15, 16] and higher body weight [17,18,19,20]. The evidence with regards to cognitive restraint is more equivocal [21]. Overall, these eating behaviour traits may result in individual differences in the likelihood of responding to food cues in the environment, yet this has rarely been studied.
In this study we investigated the moderating role of eating behaviour traits in the relationship between exposure to nearby takeaway outlets, individual takeaway consumption and adiposity.
Methods
Study sample
Between 2005 and 2015, adults born between 1950 and 1975 were recruited to the Fenland Study from the population-based registers of general practices in Cambridgeshire, the UK [22]. Participants were asked to complete a general sociodemographic and lifestyle questionnaire, and a semiquantitative food-frequency questionnaire (FFQ) to assess habitual food consumption. Participants also attended a clinical research facility where measurements of body composition were made by trained researchers following standard operating procedures. During phase 1 of this ongoing population-based study, 46,024 individuals were invited to partake in the study and 12,435 adults were recruited (response rate of 27%) [22]. The current study used a sub-sample of the Fenland Study cohort (n = 4791), in whom eating behaviour traits were assessed using the TFEQ-R18. The Fenland study was approved by the Health Research Authority National Research Ethics Service Committee East of England-Cambridge Central.
Exposure
The exposure of interest was the number of takeaway outlets within the residential neighbourhood, defined as a 1 mile radius around participants’ home address [7]. A description of the methods used for defining food environment exposures at home, as well as the validity of using secondary data sources, has previously been described [7, 23,24,25]. Briefly, participants’ home addresses were mapped by postcode using a geographic information system (ArcGIS 10, ESRI, Redlands, CA, USA) [24]. Data on food outlet (takeaway outlet and supermarket) locations were sourced from 10 local councils covering the study area in December 2011, and again mapped by postcode. Takeaway outlets were classified as those that sell hot food primarily for consumption off the premises, ordered and paid for at the cash register, with no wait staff and no or limited options for dining in. Takeaway outlets included both chains as well as local independent takeaway outlets.
Outcomes
Two primary outcomes were used; consumption of energy dense “takeaway foods” which can be commonly obtained from takeaway food outlets, and adiposity, which in the present analyses were expressed as body fat percentage from dual-energy X-ray absorptiometry (DEXA) measurement. We included both takeaway-like food consumption as well as body fat percentage as outcomes as takeaway consumption is a proximal outcome of takeaway outlet exposure, and takeaway consumption has been shown to be positively associated to body weight and adiposity [26, 27]. Body fat percentage from DEXA as a measure of adiposity was preferred over the widely and previously used measure BMI [7, 28] because 1) BMI is an indirect measure of body fat compared to more direct approaches such as that from DEXA measurement, and 2) BMI is a less accurate obesity classification method. A previous study found that BMI misclassified 25% men and 48% women compared to DEXA measurement of body fat percentage, leading to a significantly underestimated prevalence of obesity [29].
Takeaway consumption was measured using data from a food frequency questionnaire. We calculated intake (g/day) of pizza, burgers, fried fish, and French fries. Together, these foods provide a marker of takeaway-like food consumption (g/day) referred to here as “takeaway consumption”. Procedures for how body fat percentage was measured are described elsewhere [30]. Briefly, participants attended a clinical research facility after an overnight fast, where height (cm) and weight (kg) were measured by trained research assistants. Total body fat mass (g) was determined with standard imaging and positioning protocols.
As secondary outcomes, we included fat mass index (FMI) as a different expression of the DEXA data as well as BMI to allow for comparison with previous results from the same cohort [7]. FMI was calculated as fat mass (kg) divided by height squared (m2), and BMI was calculated as weight (kg) divided by height squared (m2).
Moderators
As eating behaviour traits were introduced part way through the Fenland Study, this was only available in a sub-sample of the Fenland Study cohort (n = 4791). Eating behaviour traits were measured using the TFEQ-R18 [13]. This questionnaire assesses cognitive restraint, uncontrolled eating and emotional eating using 18 items each on a 4-point Likert scale. The structural validity of the TFEQ-18 in the current sample was assessed using confirmatory factor analysis. This confirmed that the 18 items loaded onto the three factors of cognitive restraint (Cronbach’s alpha 0.75; 6 items), uncontrolled eating (Cronbach’s alpha 0.85; 9 items), and emotional eating (Cronbach’s alpha 0.87; 3 items). As in a previous study [31], raw scores were transformed to a 0–100 scale [((raw score − lowest possible raw score)/possible raw score range) × 100]. Higher scores in their respective scales are indicative of greater cognitive restraint, uncontrolled eating, or emotional eating.
Covariates
We included covariates that were hypothesized to be associated with both takeaway outlet exposure as well as the outcomes but not on the causal pathway. Covariates captured in the Fenland Study general lifestyle questionnaire included sex, age, age at completion of full time education, occupation social class (categorized as professional, intermediate or working class [32]) and total combined annual household income (<£20,000, £20,000–£39,999, ≥£40,000). We also included the number of supermarkets within home neighbourhoods defined within a 1-mile Euclidean buffer [7].
Statistical analyses
We reported sample characteristics using the mean (SD) for normally distributed continuous variables, and median (IQR) for skewed continuous variables. We reported sample characteristics for categorical variables as n (%). As outliers can negatively impact regression analyses, we adjusted outliers to the mean ± 3 SD. Data on eating behaviour traits were collected in the latter years (2011–2015) of phase 1 of the Fenland Study (2005–2015).
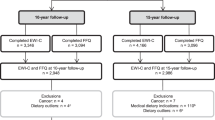
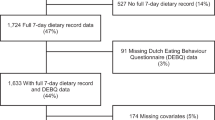
Figure 1 depicts the flow of participants from our full to analytic sample. We excluded participants without eating behaviour trait data. Subsequently, we excluded participants that were not measured using a DEXA machine (n = 68; due to one study site not having a DEXA machine for the first period of data collection) [30]. Missing data on other variables of interest ranged from 0% (e.g. age and sex) to 2.2% (i.e. household income), leading to a sample of n = 4507 (94%) with complete data. Given that we had missing data in at least 1 variable (including body fat percentage) for more than 5% of participants, and there was a reasonable likelihood that data were missing at random, we followed the recommendations of Jakobsen et al. [33], and used multivariate imputation by chained equations (MICE) to impute covariates with missing data as well as body fat percentage (seed set at 1234 and 20 imputed datasets). MICE is a multiple imputation technique that is flexible and can handle categorical as well as continuous variables [34].

Flowchart of participant inclusion to the Fenland phase 1 study up to the analytical sample included in the current study.
We divided exposure to takeaway outlets into quartiles for analysis for two reasons. First, previous analyses showed that the association between takeaway outlet exposure and takeaway consumption is non-linear [7]. Second, environmental exposure misclassification may have occurred as the number of takeaway outlets and the outcomes (takeaway consumption and body fat percentage) were measured at different time points (2011 and 2005–2015, respectively). Operationalising takeaway outlet exposure in this way minimises potential misclassification as assignment to quarters is less sensitive to unmeasured food environment change over time [28]. We used multiple linear regression models to investigate associations between exposure to takeaway outlets and the outcomes takeaway consumption and body fat percentage, and between the three eating behaviour traits and outcomes. We adjusted all models for age, sex, household income, age at highest attained educational level, occupational social class and count of supermarkets in home neighbourhood.
We investigated effect modification by adding multiplicative interaction terms (eating behaviour traits x takeaway outlet exposure quartile) to these models. We tested for evidence of interaction using the F-test (for continuous outcomes) and pooling the p-values of the separate multiple imputed datasets using the Median P Rule [35]. In order to reduce multicollinearity between predictors and interaction terms, eating behaviour traits were mean centred [36]. In line with Aiken and West [37], we probed statistically significant interactions by estimating the conditional effect of takeaway outlet exposure at various values of eating behaviour traits (i.e. mean±1 SD). Considering the lower statistical power of interaction testing in non-experimental research, we set statistical significance at a two-sided α level of 0.10 [11]. We assessed all other results with a two-sided α level of 0.05 and all analyses were conducted in STATA v16.
Results
Mean age of participants was 51.0 (SD 7.2) years and 53.9% were female (Table 1). In the overall analytic sample, median takeaway consumption was 30.0 g/day (IQR 17.5–47.5) and mean body fat percentage was 33.3 (SD 9.2). While unadjusted differences between quarters of takeaway outlet exposure were small, participants in the fourth (highest) quarter of takeaway outlet exposure consumed the least takeaway foods (27.6 g/day (IQR 10.5–41.2)), had the lowest mean body fat percentage (32.6% (95%CI 9.3) and the lowest BMI (26.2 kg/m2 (95%CI 4.4). Median exposure to takeaway outlets in the neighbourhood environment was 2.0 (IQR 0.0–12.0). The analytic sample (n = 4791) is similar to the overall Fenland Study sample (n = 12,325) (Supplementary Table 1).
Associations with takeaway consumption and body fat percentage
After adjustment for sociodemographic characteristics, compared to those living in neighbourhoods in the lowest quarter of takeaway outlet exposure, living in neighbourhoods in the highest two quarters was associated with greater takeaway consumption and body fat percentage (Table 2).
Emotional eating and uncontrolled eating were positively associated with both takeaway consumption and body fat percentage (Table 2). For example, a 10-point higher uncontrolled eating score was associated with a 1.1 (95%CI 0.9; 1.2) higher body fat percentage. A higher cognitive restraint score was associated with lower takeaway consumption, but greater body fat percentage. The results for FMI and BMI are similar to those found for body fat percentage (Supplementary Table 2), as are the results using a complete-case analysis (Supplementary Table 3).
Takeaway consumption and body fat percentage according to eating behaviour traits, socio-demographic characteristics and takeaway outlet exposure
Figures 2 and 3 display the associations between takeaway outlet exposure, and takeaway consumption and body fat percentage stratified by eating behaviour traits. Only cognitive restraint moderated the association between takeaway outlet exposure and takeaway consumption (p-value F-statisticcognitive restraint = 0.03, p-value F-statisticemotional eating = 0.72 and p-value F-statisticuncontrolled eating = 0.80 and). While for body fat percentage, both emotional eating and uncontrolled eating seem to have a similar effect on the association between takeaway outlet exposure and body fat percentage, only emotional eating statistically significantly moderated this association (p-value F-statisticcognitive restraint = 0.40, p-value F-statisticemotional eating = 0.05 and p-value F-statisticuncontrolled eating = 0.14).

Beta regression coefficient and 95% coefficient interval in the association between takeaway outlet exposure (taking Q1 as the reference group) and takeaway consumption stratified by eating behaviour traits. Asterisk indicates a statistically significant interaction by eating behaviour trait in the association between takeaway outlet exposure and takeaway consumption.

Beta regression coefficient and 95% coefficient interval in the association between takeaway outlet exposure (taking Q1 as the reference group) and body fat percentage stratified by eating behaviour traits. Asterisk indicates a statistically significant interaction by eating behaviour trait in the association between takeaway outlet exposure and body fat percentage.
To gain a better understanding of the moderating role of eating behaviour traits, Figs. 4 and 5 show the mean takeaway consumption or body fat percentage per quartile of takeaway outlet exposure stratified only for the models with statistically significant interaction terms. At all levels of takeaway outlet exposure, those with lower cognitive restraint scores had greater takeaway food consumption (Fig. 4). The association between takeaway outlet exposure and takeaway consumption was not statistically significant for participants with low cognitive restraint scores, and strongest in participants with high cognitive restraint scores (Fig. 4 and Supplementary Table 4). Furthermore, while the difference in takeaway consumption between low, mean and high cognitive restraint was statistically significant in the first three quarters of takeaway outlet exposure (as indicated by the non-overlapping 95% confidence intervals), this was no longer the case in quarter 4 of takeaway outlet exposure. In other words, the association between cognitive restraint and takeaway consumption present at lower levels of takeaway exposure was absent at the highest level of takeaway outlet exposure.

Mean and 95% confidence interval takeaway consumption per quartile of takeaway outlet exposure in the Fenland Study (n = 4791) stratified by cognitive restraint (low = 1SD – mean; high = 1SD + mean) adjusted for age, sex, household income, occupation, age at highest educational qualification and counts of supermarkets in home neighbourhoods.

Mean and 95% confidence interval body fat percentage per quartile of takeaway outlet exposure in the Fenland Study (n = 4791) stratified by emotional eating (low = 1SD – mean, high = 1SD + mean) adjusted for age, sex, household income, occupation, age at highest educational qualification and counts of supermarkets in home neighbourhoods.
The results in Fig. 5 indicate that at all levels of takeaway outlet exposure, those with higher emotional eating scores had a greater body fat percentage than those with lower emotional eating scores. We also found that the positive association between takeaway outlet exposure and body fat percentage was present at all levels of emotional eating, but strongest for low emotional eaters. For example, low emotional eaters most exposed to takeaway outlets had a 2.8% (95%CI 1.6; 4.0) greater body fat percentage than those least exposed to takeaway outlets (Supplementary Table 4). For high emotional eaters, this difference was 1.5% (95%CI 0.3; 2.7). Similar to cognitive restraint, the absolute difference in body fat percentage between those with low, mean and high emotional eating was smallest at highest levels of takeaway outlet exposure.
Discussion
In a sample of almost 5000 UK adults, we found that takeaway outlet exposure as well as emotional eating and uncontrolled eating were positively associated to both takeaway consumption and body fat percentage. We also found that cognitive restraint was negatively associated with takeaway consumption, but positively associated with body fat percentage. Eating behaviour traits partly moderated the association between takeaway outlet exposure and takeaway consumption and body fat percentage. Specifically, uncontrolled eating did not moderate the association between takeaway outlet exposure, and takeaway consumption and body fat percentage. Cognitive restraint moderated the association between takeaway outlet exposure and takeaway consumption, and emotional eating moderated the association between takeaway outlet exposure and body fat percentage. Namely, the association between takeaway outlet exposure and takeaway consumption was somewhat stronger for individuals with high cognitive restraint scores compared to lower cognitive restraint scores. Furthermore, the association between takeaway outlet exposure and body fat percentage was somewhat stronger for individuals with low emotional eating scores compared to higher emotional eating scores. However, these effects were small in all cases.
While the evidence base with regards to the association between exposure to food outlets in residential neighbourhoods and dietary behaviours is generally mixed [5, 6], the current study findings are in line with previous studies conducted in the UK [8, 9, 38]. As here, previous studies have found that having higher emotional and uncontrolled eating tendencies were associated with lower diet quality [15, 16] and higher body weight [17,18,19,20]. Some previous studies also found that higher cognitive restraint scores were associated with higher diet quality [39] and lower energy intake [18]. Comparing our interaction findings to the wider literature is difficult as very few studies have investigated the influence of psychological factors in the association between the food environment, and dietary measures or health outcomes in adults. One previous study found that the positive association between takeaway outlet exposure and takeaway consumption was stronger amongst those with higher reward sensitivity (i.e. being prone to experiencing a positive effect in response to incentives or appetitive stimuli) [12].
We found some evidence of effect modification by cognitive restraint and emotional eating, but not uncontrolled eating. Furthermore, the moderating role of emotional eating and cognitive restraint on the association between takeaway outlet exposure, and takeaway consumption and adiposity was relatively small. As the evidence for interaction was not consistent across potential moderators and outcomes, and given the number of tests performed, it is possible that our findings are based on chance. The small moderating role of cognitive restraint and emotional eating is, however, not surprising as takeaway outlets are responsible for only a small amount of the variance in adiposity. Also, the direction of the effect modification is not surprising, which we explain in the following paragraphs.
Cognitive restraint was negatively associated with reported takeaway consumption, but positively associated with body fat percentage. Given the positive association between takeaway consumption and body weight [26, 27], we expected the associations between cognitive restraint, and takeaway consumption and body fat to be in the same direction (unless differential bias by restraint was present in the reporting of food intake). The current study findings together with previous findings suggest that the association between cognitive restraint and adiposity is likely bi-directional. Previous longitudinal studies found that high baseline adiposity or BMI was more likely to be associated with increased, rather than decreased, cognitive restraint [40, 41], suggesting that exerting cognitive restraint is likely to be a consequence of increased body weight instead of a cause. This bi-directionality may explain our study findings; we found that the association between takeaway outlet exposure and takeaway consumption (but not body fat percentage) was somewhat stronger among individuals with higher cognitive restraint scores. Individuals with high cognitive restraint scores may be actively trying to eat less, which is more difficult in areas with high takeaway outlet exposure compared to lower exposure.
In the current analysis, emotional eating was positively associated with both takeaway consumption and body fat percentage. Contrary to the aforementioned study [12], the results seem to suggest that the association between takeaway outlet exposure and body fat percentage is stronger for individuals with lower emotional eating scores, albeit at lower absolute levels of adiposity. This finding may suggest that the close environment matters more for those with less individual tendencies of partaking in unhealthy dietary behaviours. The findings may additionally suggest that high emotional eaters will find takeaway food if they want it, regardless of the local density of takeaway outlets. Previous studies found that eating behaviour traits are partly hereditary [42, 43], and that genetic risk for obesity was positively associated with emotional eating [31]. In a previous analysis conducted in the Fenland cohort, we found that the association between takeaway outlet exposure and BMI for those with a high and low genetic risk of obesity did not differ statistically significantly [28]. Nevertheless, we did find a somewhat weaker association between the food environment and BMI among those with higher genetic risk of obesity compared to those with lower genetic risk, indicating that the local environment mattered less for those at high individual risk of obesity. We argued in that study that the findings are consistent with Rothman’s component cause model [44], which suggests that for multiple cause outcomes, the strength of one causal factor is influenced by the relative prevalence of other causal factors [28].
The current study results suggest that those exposed to the most takeaway outlets are at an increased risk of adiposity than those exposed to the least takeaway outlets. Thus, intervening on eating behaviour traits alone to improve health outcomes will not remove the negative influence the current obesogenic environment has on these health outcomes. The reverse is also true; intervening only on the food environment will not remove all individual differences in dietary behaviours and adiposity. As such, there is a need to implement integrated strategies addressing both individual and environmental influences on dietary behaviours. Multiple interventions at different levels of influence need to be implemented to reduce unhealthy dietary behaviours and obesity levels, including downstream approaches targeting individuals most at risk (e.g. mindfulness meditation for high emotional eaters [45]), as well as more upstream approaches targeting the food environment at the population-level (e.g. restricting the number of takeaway outlets around schools [46]).
Our study has several strengths including having extensively measured diet, body weight, adiposity and the food environment. In particular, we used an objective imaging method to measure adiposity instead of BMI which is, among other things, unable to differentiate between fat mass and muscle mass [47]. Furthermore, we included a relatively large sample of individuals from multiple areas across Cambridgeshire, UK, and with characteristics that are broadly representative of the regional population. However, the sample may be less representative of other regions of the UK, particularly in terms of ethnic diversity. Given that our Fenland Study sample was constituted of relatively older adult participants, the current study findings may also not be generalizable to younger adults. Another limitation is the cross-sectional study design, which does not allow for strong inferences about causality. A third limitation includes the reliability and validity of some of the measures. While previous research found that the TFEQ-R18 has good reliability and validity [48], emotional eating scores may be subject to floor and ceiling effects as they are derived from only three items [14]. Furthermore, it is possible that we failed to capture some foods commonly consumed outside of the home (e.g. fried chicken and Asian dishes) resulting in an underestimation of takeaway consumption. It is also possible that we have misclassified foods such those bought from supermarkets, as takeaway foods, resulting in an overestimation of takeaway consumption. However, we found a positive association between our measure of takeaway consumption and the frequency of consuming take-away meals at home (data not shown). Moreover, similar results were found for both outcomes (takeaway consumption and body fat percentage), while any under- or overestimations of takeaway consumption are unlikely to have impacted the moderation of eating behaviours we observed. As discussed in previous work [7], another limitation is the temporal mismatch between data sources, arising from capture of food outlet data at only one time point (2011) within the period of participant data collection (2005–2015). Takeaway consumption and body fat percentage for some participants predated their takeaway outlet exposure, and it is unknown how long participants had been exposed to takeaway food outlets in their home environment. This is a common consideration in research of this type.
Besides longitudinal studies, further research is needed in different populations to confirm the current study results. This research may use other, more reliable or complementary, eating behaviour trait measurements such as the new version of the TFEQ (TFEQ-R21 [49]), which further improved TFEQ’s psychometric properties, or Ecological Momentary Assessments that are able to reduce biases associated with retrospective recall [50]. Future studies may also want to investigate the moderating role of other psychological factors such as external eating, emotional eating in response to positive emotions, emotional under-eating and food-responsiveness (e.g. as assessed by the Adult Eating Behaviour Questionnaire [51]). Studies may also include other outcomes such as general energy-dense food consumption.
Conclusion
Individual differences in eating behaviour traits and exposure to takeaway outlets were both associated with takeaway consumption and adiposity. The evidence that individuals with certain eating behaviour traits are more susceptible to takeaway outlets was weak; there was no evidence that the association between takeaway outlet exposure and takeaway consumption or body fat varied by uncontrolled eating. While the magnitude of other effects were small, we found that the positive association between takeaway outlet exposure and body fat percentage was strongest for low emotional eaters, and the positive association between takeaway outlet exposure and takeaway consumption was strongest for those with high cognitive restraint scores. Our findings indicate that it is important to implement integrated strategies addressing both individual and environmental influences of dietary behaviours to tackle the current obesity epidemic.
Data availability
While the Fenland Study (https://www.mrc-epid.cam.ac.uk/research/studies/fenland/) data is not publicly available for reasons of confidentiality, it may be available upon reasonable request by emailing datasharing@mrc-epid.cam.ac.uk.
References
Swinburn B, Egger G, Raza F. Dissecting obesogenic environments: the development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev Med. 1999;29:563–70.
Lake A, Townshend T. Obesogenic environments: exploring the built and food environments. J R Soc Promot Health. 2006;126:262–7.
Pinho MGM, Mackenbach JD, den Braver NR, Beulens JJ, Brug J, Lakerveld J. Recent changes in the Dutch foodscape: socioeconomic and urban-rural differences. Int J Behav Nutr Phys Act. 2020;17:1–11.
Maguire ER, Burgoine T, Monsivais P. Area deprivation and the food environment over time: A repeated cross-sectional study on takeaway outlet density and supermarket presence in Norfolk, UK, 1990–2008. Health Place. 2015;33:142–7.
Cobb LK, Appel LJ, Franco M, Jones‐Smith JC, Nur A, Anderson CA. The relationship of the local food environment with obesity: a systematic review of methods, study quality, and results. Obesity. 2015;23:1331–44.
Caspi CE, Sorensen G, Subramanian S, Kawachi I. The local food environment and diet: a systematic review. Health Place. 2012;18:1172–87.
Burgoine T, Forouhi NG, Griffin SJ, Wareham NJ, Monsivais P. Associations between exposure to takeaway food outlets, takeaway food consumption, and body weight in Cambridgeshire, UK: population based, cross sectional study. Bmj. 2014;348:g1464.
Burgoine T, Sarkar C, Webster CJ, Monsivais P. Examining the interaction of fast-food outlet exposure and income on diet and obesity: evidence from 51,361 UK Biobank participants. Int J Behav Nutr Phys Act. 2018;15:1–12.
Mason KE, Pearce N, Cummins S. Associations between fast food and physical activity environments and adiposity in mid-life: cross-sectional, observational evidence from UK Biobank. Lancet Public Health. 2018;3:e24–e33.
Blundell JE, Stubbs R, Golding C, Croden F, Alam R, Whybrow S, et al. Resistance and susceptibility to weight gain: individual variability in response to a high-fat diet. Physiol Behav. 2005;86:614–22.
Paquet C, de Montigny L, Labban A, Buckeridge D, Ma Y, Arora N, et al. The moderating role of food cue sensitivity in the behavioral response of children to their neighborhood food environment: a cross-sectional study. Int J Behav Nutr Phys Act. 2017;14:1–12.
Paquet C, Daniel M, Knäuper B, Gauvin L, Kestens Y, Dubé L. Interactive effects of reward sensitivity and residential fast-food restaurant exposure on fast-food consumption. Am J Clin Nutr. 2010;91:771–6.
Karlsson J, Persson L-O, Sjöström L, Sullivan M. Psychometric properties and factor structure of the Three-Factor Eating Questionnaire (TFEQ) in obese men and women. Results from the Swedish Obese Subjects (SOS) study. Int J Obes. 2000;24:1715–25.
Duarte PA, Palmeira L, Pinto-Gouveia J. The Three-Factor Eating Questionnaire-R21: A confirmatory factor analysis in a Portuguese sample. Eat Weight Disord. 2020;25:247–56.
Aguirre TM, Kuster JT, Koehler AE. Relationship between eating behavior and dietary intake in rural Mexican-American mothers. J Immigr Minor Health. 2017;19:225–7.
Bernstein EE, Nierenberg AA, Deckersbach T, Sylvia LG. Eating behavior and obesity in bipolar disorder. Aust N Z J Psychiatr. 2015;49:566–72.
Löffler A, Luck T, Then FS, Sikorski C, Kovacs P, Böttcher Y, et al. Eating behaviour in the general population: an analysis of the factor structure of the German version of the three-factor-eating-questionnaire (TFEQ) and its association with the body mass index. PloS One. 2015;10:e0133977.
French SA, Mitchell NR, Finlayson G, Blundell JE, Jeffery RW. Questionnaire and laboratory measures of eating behavior. Associations with energy intake and BMI in a community sample of working adults. Appetite. 2014;72:50–58.
Porter Starr K, Fischer JG, Johnson MA. Eating behaviors, mental health, and food intake are associated with obesity in older congregate meal participants. J Nutr Gerontol Geriatr. 2014;33:340–56.
Iceta S, Julien B, Seyssel K, Lambert-Porcheron S, Segrestin B, Blond E, et al. Ghrelin concentration as an indicator of eating-disorder risk in obese women. Diabet Metab. 2019;45:160–6.
Bryant EJ, Rehman J, Pepper LB, Walters ER. Obesity and eating disturbance: The role of TFEQ restraint and disinhibition. Cur Obes Rep. 2019;8:363–72.
Lindsay T, Westgate K, Wijndaele K, Hollidge S, Kerrison N, Forouhi N, et al. Descriptive epidemiology of physical activity energy expenditure in UK adults (The Fenland study). Int J Behav Nutr Phys Act. 2019;16:1–13.
Burgoine T, Monsivais P. Characterising food environment exposure at home, at work, and along commuting journeys using data on adults in the UK. Int J Behav Nutr Phys Act. 2013;10:1–11.
Burgoine T, Mackenbach JD, Lakerveld J, Forouhi NG, Griffin SJ, Brage S, et al. Interplay of socioeconomic status and supermarket distance is associated with excess obesity risk: a UK cross-sectional study. Int J Environ Res Public Health. 2017;14:1290.
Lake AA, Burgoine T, Greenhalgh F, Stamp E, Tyrrell R. The foodscape: classification and field validation of secondary data sources. Health Place. 2010;16:666–73.
Fraser LK, Clarke GP, Cade JE, Edwards KL. Fast food and obesity: a spatial analysis in a large United Kingdom population of children aged 13–15. Am J Prev Med. 2012;42:e77–e85.
Pieroni L, Salmasi L. Fast-food consumption and body weight. Evidence from the UK. Food Policy. 2014;46:94–105.
Burgoine T, Monsivais P, Sharp SJ, Forouhi NG, Wareham NJ. Independent and combined associations between fast-food outlet exposure and genetic risk for obesity: a population-based, cross-sectional study in the UK. BMC Med. 2021;19:1–9.
Shah NR, Braverman ER. Measuring adiposity in patients: the utility of body mass index (BMI), percent body fat, and leptin. PloS One. 2012;7:e33308.
Lindsay T, Wijndaele K, Westgate K, Dempsey P, Strain T, Rolfe EDL, et al. Joint associations between objectively measured physical activity volume and intensity with body-fatness. The Fenland Study. Int J Obes. 2022;46:169–77.
de Lauzon-Guillain B, Clifton EA, Day FR, Clément K, Brage S, Forouhi NG, et al. Mediation and modification of genetic susceptibility to obesity by eating behaviors. Am J Clin Nutr. 2017;106:996–1004.
Social Mobility Commission. Simplifying how employers measure socio-economic background [Internet]. 2021. Cited August 1st 2022. Available from: https://socialmobilityworks.org/wp-content/uploads/2021/05/Summary-report-on-measurement-changes_FINAL-Updated-May-2021.pdf.
Jakobsen JC, Gluud C, Wetterslev J, Winkel P. When and how should multiple imputation be used for handling missing data in randomised clinical trials–a practical guide with flowcharts. BMC Med Res Methodol. 2017;17:1–10.
Azur MJ, Stuart EA, Frangakis C, Leaf PJ. Multiple imputation by chained equations: what is it and how does it work? Int J Methods Psychiatr Res. 2011;20:40–49.
Eekhout I, Van De Wiel MA, Heymans MW. Methods for significance testing of categorical covariates in logistic regression models after multiple imputation: power and applicability analysis. BMC Med Res Methodol. 2017;17:1–12.
Holmbeck GN. Post-hoc probing of significant moderational and mediational effects in studies of pediatric populations. J Pediatr Psychol. 2002;27:87–96.
Aiken LS, West SG, Reno RR. Multiple regression: Testing and interpreting interactions. Sage; 1991.
Vogel C, Lewis D, Ntani G, Cummins S, Cooper C, Moon G, et al. The relationship between dietary quality and the local food environment differs according to level of educational attainment: A cross-sectional study. PloS one. 2017;12:e0183700.
Hoenink JC, Waterlander WE, Beulens JJ, Mackenbach JD. The role of material and psychosocial resources in explaining socio-economic inequalities in diet: A structural equation modelling approach. SSM Popul Health. 2022;17:101025.
Snoek HM, van Strien T, Janssens JM, Engels RC. Restrained eating and BMI: a longitudinal study among adolescents. Health Psychol. 2008;27:753.
Chavance M, Escolano S, Romon M, Basdevant A, de Lauzon-Guillain B, Charles MA. Latent variables and structural equation models for longitudinal relationships: an illustration in nutritional epidemiology. BMC Med Res Methodol. 2010;10:1–10.
Herle M, Madrid-Valero JJ, Morosoli JJ, Colodro-Conde L, Ordoñana J. The role of the environment in overweight and eating behavior variability: insights from a multivariate twin study. Twin Res Hum Genet. 2020;23:338–44.
Keskitalo K, Tuorila H, Spector TD, Cherkas LF, Knaapila A, Kaprio J, et al. The Three-Factor Eating Questionnaire, body mass index, and responses to sweet and salty fatty foods: a twin study of genetic and environmental associations. Am J Clin Nutr. 2008;88:263–71.
Rothman KJ. Causes. Am J Epidemiol. 1976;104:587–92.
Katterman SN, Kleinman BM, Hood MM, Nackers LM, Corsica JA. Mindfulness meditation as an intervention for binge eating, emotional eating, and weight loss: a systematic review. Eating Behav. 2014;15:197–204.
Keeble M, Burgoine T, White M, Summerbell C, Cummins S, Adams J. How does local government use the planning system to regulate hot food takeaway outlets? A census of current practice in England using document review. Health Place. 2019;57:171–8.
Stevens J, McClain J, Truesdale K. Selection of measures in epidemiologic studies of the consequences of obesity. Int J Obes. 2008;32:S60–S66.
Anglé S, Engblom J, Eriksson T, Kautiainen S, Saha M-T, Lindfors P, et al. Three factor eating questionnaire-R18 as a measure of cognitive restraint, uncontrolled eating and emotional eating in a sample of young Finnish females. Int J Behav Nutr Phys Act. 2009;6:1–7.
Cappelleri J, Bushmakin A, Gerber R, Leidy N, Sexton C, Lowe M, et al. Psychometric analysis of the Three-Factor Eating Questionnaire-R21: results from a large diverse sample of obese and non-obese participants. Int J Obes. 2009;33:611–20.
Bongers P, Jansen A. Emotional eating is not what you think it is and emotional eating scales do not measure what you think they measure. Front Psychol. 2016;7:1932.
Hunot C, Fildes A, Croker H, Llewellyn CH, Wardle J, Beeken RJ. Appetitive traits and relationships with BMI in adults: Development of the Adult Eating Behaviour Questionnaire. Appetite. 2016;105:356–63.
Acknowledgements
We would like to thank the Fenland participants for participating in the study, as well as the Fenland Study Coordination, Field Epidemiology and Data Management teams for supplying the data. We also thank David Collins for his statistical advice and Stephen Sharp for his help interpreting and presenting the results.
Funding
The Fenland Study is funded by the MRC and the study PIs (NJW, SB, NGF and SG) acknowledge this support (grant numbers MC_UU_00006/1, MC_UU_00006/3, MC_UU_00006/6). JCH, JA and TB are currently supported by the Medical Research Council [Unit Programme number MC_UU_00006/7]. PM received support from the Health Equity Research Center at Washington State University. SB, NGF and NJW acknowledge support from the National Institute of Health Research (NIHR) Cambridge Biomedical Research Centre (BRC) Nutrition, Diet, and Lifestyle Research Theme (IS-BRC-1215-20014). NGF is an NIHR Senior Investigator. The University of Cambridge has received salary support in respect of SG from the NHS in the East of England through the Clinical Academic Reserve. The funders played no role in the design of the study, the collection, analysis, and interpretation of data, or the writing of the manuscript. For the purpose of Open Access, the authors have applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising.
Author information
Authors and Affiliations
Contributions
JA, TB and AA conceived the idea for the work. The analysis plan was designed by JCH, TB and JA. TB led the takeaway outlet data collection from local councils. JCH led the data analysis, in consultation with TB, AA, SB, PM and JA. Principal investigators of the Fenland study who were responsible for its overall design, management and supervision of data collection are SB, NGF, SG and NJW. JCH drafted the manuscript and JCH, TB and JA interpreted the results. All authors reviewed and edited the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study complies with the Declaration of Helsinki and was approved by the Health Research Authority National Research Ethics Service Committee East of England-Cambridge Central. Informed consent was obtained from all the participants before starting the study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hoenink, J.C., Burgoine, T., Brage, S. et al. The moderating role of eating behaviour traits in the association between exposure to hot food takeaway outlets and body fatness. Int J Obes 47, 496–504 (2023). https://doi.org/10.1038/s41366-023-01290-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-023-01290-9
This article is cited by
-
Impact of the Neighborhood Food Environment on Dietary Intake and Obesity: a Review of the Recent Literature
Current Diabetes Reports (2023)
