
Abstract
Background
Limited data exist on the association of obesity with both hospitalization and mortality in patients with heart failure with preserved ejection fraction (HFpEF), especially in the real-world ambulatory setting. We hypothesized that increasing body-mass index (BMI) in ambulatory heart failure with preserved ejection fraction would have a protective effect on these patients leading to decreased mortality and hospitalizations.
Methods
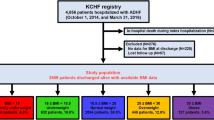
We studied the relationship between BMI and the time to all-cause mortality, time to heart failure (HF) hospitalization, and time to all-cause hospitalization over a 2-year follow-up in a national cohort of 2501 ambulatory HFpEF patients at 153 Veterans Affairs medical centers.
Results
Compared with normal BMI, overweight (HR 0.72; 95% CI 0.57–0.91), obesity class I (HR 0.59; 95% CI 0.45–0.77), obesity class II (HR 0.56; 95% CI 0.40–0.77), and obesity class III (HR 0.53; 95% CI 0.36–0.77) were associated with improved survival after adjustment for demographics and comorbidities. In contrast, the time to HF hospitalization showed an inverse relationship, with shorter time to HF hospitalization with increasing BMI compared with normal BMI; overweight (adjusted HR 1.30; 95% CI 0.88–1.90), obesity class I (HR 1.57; 95% CI 1.05–2.34), obesity class II (HR 1.79; 95% CI 1.15–2.78), and obesity class III (HR 1.96; 95% CI 1.23–3.12). However, time to first all-cause hospitalization was not significantly different by BMI groups.
Conclusions
In a large, national ambulatory HFpEF cohort, despite the presence of the obesity paradox with respect to survival, increasing BMI was independently associated with an increased risk of HF hospitalization and similar risk of all-cause hospitalization. Future longer-term prospective trials evaluating the safety and efficacy of weight loss on morbidity and mortality, in patients with severe obesity and HFpEF are needed.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US adults, 1999–2000. JAMA. 2002;288:1723–7.
Popkin BM, Doak CM. The obesity epidemic is a worldwide phenomenon. Nutr Rev. 1998;56:106–14.
Hales C, Carroll M, Fryar C, Ogden C. Prevalence of obesity among adults and youth: United States. National Health and Nutrition Examination, CDC 2017:288.
Kenchaiah S, Evans J, Levy D, Wilson P, Benjamin E, Larson M, et al. Obesity and the risk of heart failure. N Engl J Med. 2002;347:305–13.
Obokata M, Reddy Y, Pislaru S, Melenovsky V, Borlaug B. Evidence supporting the existence of a distinct obese phenotype of heart failure with preserved ejection fraction. Circulation. 2017;136:6–19.
Kitzman DW, Shah SJ. The HFpEF obesity phenotype: the elephant in the room. J Am Coll Cardiol. 2016;68:200–3.
Aune D, Sen A, Norat T, Janszky I, Romundstad P, Tonstad S, et al. Body mass index, abdominal fatness, and heart failure incidence and mortality. Circulation. 2016;133:639–49.
Horwich T, Fonarow G, Clark A. Obesity and the obesity paradox in heart failure. Prog Cardiovasc Dis. 2018;61:151–6.
Elagizi A, Kachur S, Lavie C, Carbone S, Pandey A, Ortega F, et al. An overview and update on obesity and the obesity paradox in cardiovascular diseases. Prog Cardiovasc Dis. 2018;61:142–50.
Ather S, Chan W, Bozkurt B, Aguilar D, Ramasubbu K, Zachariah A, et al. Impact of noncardiac comorbidities on morbidity and mortality in a predominantly male population with heart failure and preserved versus reduced ejection fraction. J Am Coll Cardiol. 2012;59:998–1005.
Deswal A, Petersen N, Urbauer D, Wright S, Beyth R. Racial variations in quality of care and outcomes in an ambulatory heart failure cohort. Am Heart J. 2006;152:348–54.
Padwal R, McAlister F, McMurray J, Cowie M, Rich M, Pocock S, et al. The obesity paradox in heart failure patients with preserved versus reduced ejection fraction: a meta-analysis of individual patient data. Int J Obes. 2014;38:1110–4.
Kenchaiah S, Pocock S, Wang D, Finn P, Zornoff L, Skali H, et al. Body mass index and prognosis in patients with chronic heart failure: insights from the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) program. Circulation. 2007;116:627–36.
Haass M, Kitzman D, Anand I, Miller A, Zile M, Massie B, et al. Body mass index and adverse cardiovascular outcomes in heart failure patients with preserved ejection fraction: results from the Irbesartan in Heart Failure with Preserved Ejection Fraction (I-PRESERVE) trial. Circ Heart Fail. 2011;4:324–31.
Mandviwala T, Khalid U, Deswal A. Obesity and cardiovascular disease: a risk factor or a risk marker? Curr Atheroscler Rep. 2016;18:21.
Tsujimoto T, Kajio H. Abdominal obesity is associated with an increased risk of all-cause mortality in patients with HFpEF. J Am Coll Cardiol. 2017;70:2739–49.
Flegal KM, Shepherd JA, Looker AC, Graubard BI, Borrud LG, Ogden CL, et al. Comparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adults. Am J Clin Nutr. 2009;89:500–8.
Blew RM, Sardinha LB, Milliken LA, Teixeira PJ, Going SB, Ferreira DL, et al. Assessing the validity of body mass index standards in early postmenopausal women. Obes Res. 2002;10:799–808.
Clark AL, Fonarow GC, Horwich TB. Waist circumference, body mass index, and survival in systolic heart failure: the obesity paradox revisited. J Cardiac Fail. 2011;17:374–80.
Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B, et al. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med. 2014;370:1383–92.
Alexander JK, Dennis EW, Smith WG, Amad KH, Duncan WC, Austin RC. Blood volume, cardiac output, and distribution of systemic blood flow in extreme obesity. Cardiovasc Res Cent Bull. 1962;1:39–44.
Nagarajan V, Cauthen C, Starling R, Tang W. Prognosis of morbid obesity patients with advanced heart failure. Congest Heart Fail. 2013;19:160–4.
Haykowsky M, Kouba E, Brubaker P, Nicklas B, Eggebean J, Kitzman D. Skeletal muscle composition and its relation to exercise intolerance in older patients with heart failure and preserved ejection fraction. J Am Coll Cardiol. 2014;7:1211–6.
Paulus W, Tschope C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol. 2013;62:263–71.
Dalos D, Mascherbauer J, Zotter-Tufaro C, Duca F, Kammerlander A, Aschauer S, et al. Functional status, pulmonary artery pressure, and clinical outcomes in heart failure with preserved ejection fraction. J Am Coll Cardiol. 2016;68:189–99.
Kitzman D, Brubaker P, Morgan T. The effect of calortic restriction or aerobic exercise training on peak oxygen consumption and quality of life in older obese patients with heart failure with preserved ejection fraction. JAMA. 2016;315:36–46.
Miranda W, Batsis J, Sarr M, Collazo-Clavell M, Clark M, Somers V. Impact of bariatric surgery on quality of life, functional capacity, and symptoms in patients with heart failure. Obes Surg. 2013;23:1011–115.
Shimada Y, Tsugawa Y, Brown D, Hasegawa K. Bariatric surgery and emergency department visits and hospitalizatins for heart failure exacerbation: population-based, self-controlled series. J Am Coll Cardiol. 2016;67:895–903.
Kapoor J, Heidenreich P. Obesity and survival in patients with heart failure and preserved systolic function: a U-shaped relationship. Am Heart J. 2010;159:75–80.
Oreopoulos A, Padwal R, Kalantar-Zadeh K, Fonarow G, Norris C, McAlister F. Body mass index and mortality in heart failure: a meta-analysis. Am Heart J. 2008;156:13–22.
Stavrakis S, Pakala A, Thomas J, Chaudhry M, Thadani U. Obesity, brain natriuretic peptide levels and mortality in patients hospitalized with heart failure and preserved left ventricular systolic function. Am J Med Sci. 2013;345:211–7.
Lavie C, Ventura H. Weighing in on obesity and the obesity paradox in heart failure. J Card Fail. 2011;17:381–3.
Wolk R, Bertolet M, Singh P, Brooks M, Pratley R, Frye R, et al. Prognostic value of adipokines in predicting cardiovascular outcome: explaining the obesity paradox. Mayo Clin Proc. 2016;91:858–66.
Heo S, Moser D, Pressler S, Dunbar S, Lee K, Kim J, et al. Association between obesity and heart failure symptoms in male and female patients. Clin Obes. 2017;7:77–85.
Pocock S, McMurray J, Dobson J, Yusuf S, Granger C, Michelson E, et al. Weight loss and mortality risk in patients with chronic heart failure in the candesartan in heart failure: assessment of reduction in mortality and morbidity (CHARM) programme. Eur Heart J. 2008;29:2641–50.
Lavie C, Cahalin L, Chase P, Myers J, Bensimhon D, Peberdy M, et al. Impact of cardiorespiratory fitness on the obesity paradox in patients with heart failure. Mayo Clinic Proc. 2013;88:251–8.
Hegde SM, Claggett B, Shah AM, Lewis EF, Anand I, Shah SJ, et al. Physical activity and prognosis in the TOPCAT Trial (Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist). Circulation. 2017;136:982–92.
Acknowledgements
The authors thank the Office of Quality and Performance of the Veterans Health Administration for providing EPRP data. The views expressed in this report are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs.
Funding
This study was supported in part by VA Health Services Research & Development Service #IIR 02-082-1.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None of the authors have any financial or other relations that could lead to a conflict of interest. AD is supported in part by the Ting Tsung and Wei Fong Chao Distinguished Chair at the MD Anderson Cancer Center.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mandviwala, T.M., Basra, S.S., Khalid, U. et al. Obesity and the paradox of mortality and heart failure hospitalization in heart failure with preserved ejection fraction. Int J Obes 44, 1561–1567 (2020). https://doi.org/10.1038/s41366-020-0563-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-020-0563-1
This article is cited by
-
Influence of diabetes and obesity on ten-year outcomes after coronary artery bypass grafting in the arterial revascularisation trial
Clinical Research in Cardiology (2023)
-
Distinct implications of body mass index in different subgroups of nonobese patients with heart failure with preserved ejection fraction: a latent class analysis of data from the TOPCAT trial
BMC Medicine (2022)
-
Obesity paradox and heart failure
Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity (2021)
-
Disparate effects of obesity on survival and hospitalizations in heart failure with preserved ejection fraction
International Journal of Obesity (2020)
