
Abstract
Thyroid hormones (THs) are key regulators of cellular growth, development, and metabolism. The thyroid gland secretes two THs, thyroxine (T4) and triiodothyronine (T3), into the plasma where they are almost all bound reversibly to plasma proteins. Free forms of THs are metabolically active, however, they represent a very small fraction of total TH levels. No genome-wide studies have been performed to date on total TH levels, comprising of protein-bound and free forms of THs. To detect genetic variants associated with total TH levels, we carried out the first GWAS meta-analysis of total T4 levels in 1121 individuals from two Croatian cohorts (Split and Korcula). We also performed GWAS analyses of total T3 levels in 577 individuals and T3/T4 ratio in 571 individuals from the Split cohort. The top association in GWAS meta-analysis of total T4 was detected for an intronic variant within SLC22A9 gene (rs12282281, P = 4.00 × 10−7). Within the same region, a genome-wide significant variant (rs11822642, P = 2.50 × 10−8) for the T3/T4 ratio was identified. SLC22A9 encodes for an organic anion transporter protein expressed predominantly in the liver and belongs to the superfamily of solute carriers (SLC), a large group of transport membrane proteins. The transport of THs across the plasma membrane in peripheral tissues is facilitated by the membrane proteins, and all TH transport proteins known to date belong to the same SLC superfamily as SLC22A9. These results suggest a potential role for SLC22A9 as a novel transporter protein of THs.
Similar content being viewed by others


Introduction
The thyroid gland secretes two thyroid hormones (THs), thyroxine (T4) and triiodothyronine (T3), that are essential for the regulation of many metabolic processes throughout the body [1]. The production and secretion of THs are regulated by the combined action of the hypothalamus, pituitary, and thyroid gland known as the hypothalamus–pituitary–thyroid axis [2]. The release of the T4 and T3 into the circulation is under the direct control of the thyroid-stimulating hormone (TSH) from the pituitary gland [1].
Once secreted into the plasma, THs circulate almost entirely bound to plasma proteins (99.8%), and only a small proportion of THs exist as the unbound free fraction [3]. The free T4 (fT4) and free T3 (fT3) are biologically active and affect intracellular metabolism [3], with T3 being 3–4 times more potent than T4. T3 is a major active form of THs that binds to TH receptors in target cells [1], while T4 is thought to act more as a reservoir of THs in the blood. In the euthyroid state, the T4 hormone is secreted by the thyroid gland in much higher concentrations than T3, in a ratio of approximately 17:1 [4] and has a longer half-life than T3 (1 week versus 1 day) [5]. The relationship between T4 and T3 levels in healthy individuals, usually expressed as a T3/T4 ratio, is a finely tuned measure where individuals with the highest T4 tend to have a minimal T3/T4 ratio, and those with lower T4 have an increase in the T3 fraction [6, 7].
Serum thyroid levels have substantial inter-individual variability, while the intra-individual variability is within a narrow range resulting in a specific thyroid set-point for an individual [8]. Estimates show that approximately 45–65% of the inter-individual variation in serum TSH, fT3, and fT4 levels is influenced by genetic factors [8, 9]. Heritability for total THs was estimated to be around 30% [10, 11]. So far, nothing is known about genetic variants influencing total T4 nor T3 levels in the blood. In the last decade, genome-wide association analyses (GWAS) have identified more than 40 genes associated with thyroid function, mostly with TSH and fT4 levels [12, 13], but none has been conducted for total TH levels. Although the free forms of THs are biologically active, identification of genetic background underlying total TH levels may provide important information since they represent total availability of THs in the circulation. The underlying genes related to the total thyroid levels potentially revealed by GWAS can lead to important biological pathways of TH metabolism.
The aim of this study is the identification of genetic loci associated with total TH levels by performing a GWAS meta-analysis of total T4 levels combining results from two Croatian populations (Split and Korcula). A GWAS for total T3 serum levels and the T3/T4 ratio was performed in Split cohort only.
Materials and methods
Study population
This study included 1121 individuals from two Croatian cohorts: from the city of Split and the island of Korcula. The individuals were derived from the population-based “10 001 Dalmatians project”, which is a part of the Croatian Biobank program [14]. The baseline characteristics of the study population are presented in Table 1. The study was approved by Ethics Committee from the University of Split, School of Medicine (Classification No. 003-08/11-03/0005; Registry No. 2181-198-03-04/10-11-0008), and it is in accordance with the provisions of the Code of Ethics and the Helsinki Declaration. Written informed consent was obtained from all study participants.
Genotyping and imputation
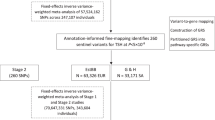
Genotyping, imputation details, and quality control procedures for individual cohorts are described in the previous studies of Matana et al. [15, 16]. All single nucleotide polymorphisms (SNPs) with a minor allele frequency <0.01 or having an imputation quality <0.4 in any of the two cohorts, were removed from the analyses. After exclusions, the final number of SNPs included in the analyses were 7,597,900 for T4 levels present in the Split and Korcula cohort, 8,753,628 for T3 levels and 8,752,746 for T3/T4 levels present in the Split cohort only.
Biochemical measurements
Serum levels of total T4 and total T3 were determined by a chemiluminescence immunoassay method using a fully automated instrument “Liaison” Biomedica Chemiluminescence Analyzer in the Laboratory of Biochemistry, Department of Nuclear Medicine, University Hospital Split. The reference ranges for serum levels were T4: 57–161 nmol/L and T3: 1.3–3.6 nmol/L. Individuals taking thyroid medication, who underwent thyroid surgery, who had positive thyroglobulin autoantibody (TgAb) or thyroid peroxidase autoantibody (TPOAb), or had serum T4, TSH, fT3, fT4 levels outside the normal range, were excluded from the analysis. Total T4 serum levels were measured in both cohorts, Split and Korcula. Total T3 serum levels were measured in Split cohort only. After applying above described exclusion criteria, the number of individuals with genotyped data available was 623 in the Split cohort, and 498 in the Korcula cohort for T4 levels, and 577 individuals in the Split cohort for T3 levels. We also created a variable of the T3/T4 ratio for all individuals where both T3 and T4 were available (N = 571).
Genome-wide association analyses
Total T4 levels were analyzed in Split and Korcula cohorts separately and later combined by meta-analysis. Total T3 levels and T3/T4 ratio were analyzed in Split cohort only. Prior to analyses, each trait was adjusted for fixed effects of age, sex, and body mass index (BMI) [17] using linear regression analysis, and the obtained residuals were inverse-Gaussian-transformed to achieve a normal distribution. Association analyses of adjusted trait levels were performed using a linear mixed model, which accounts for population structure and relatedness, assuming an additive genetic model. For the Split cohort, the analyses were performed using GenABEL R statistical package and SNPTEST, and for the Korcula cohort using GenABEL and VariABEL [18, 19]. All GWAS inflation factors (lambda values) were close to 1 (λ > 0.99), so no genomic correction was applied.
Meta-analysis
Association results of total T4 levels for two cohorts, Split and Korcula, were combined using an inverse-variance fixed-effect meta-analysis performed in the R-package MetABEL, version 3.3.1 (available from http://www.R-project.org/), using estimates of the allelic effect size and standard error. Genomic control inflation factor (lambda) for the meta-analysis was λ = 1.00.
To evaluate heterogeneity in effect sizes between two cohorts, we used I2 statistic for heterogeneity implemented in METAL [20], but no heterogeneity was detected (HetI2 = 0.0%, HetP = 0.589). The UCSC Genome Browser, Ensembl, and Locus Zoom were used to identify genes in the regions where significant SNPs were identified [21, 22]. Manhattan plots and quantile–quantile plots were created to visualize association results using the R package qqman [23]. Cluster plots of all prioritized SNPs were examined using the Illumina GenomeStudio software package, to minimize the possibility of spurious association due to genotyping error. Associations were considered genome-wide significant if P-values were below 5 × 10−8 and suggestive if P-values were below 5 × 10−7.
Results
In the GWAS meta-analysis of total T4 levels across Split and Korcula cohorts (Fig. 1), the top finding was shown for an intron variant rs12282281 with suggestive evidence of association (P = 4.00 × 10−7, β = −0.88, SE = 0.17, MAF = 0.02, Table 2). SNP rs12282281 is located on chromosome 11 in the SLC22A9 gene. The regional association plot for rs12282281 is presented in Fig. 2.

a Manhattan plot of all SNPs in the meta-analysis with T4 levels. b Manhattan plot of all SNPs in GWAS analysis with T3/T4 ratio. c Manhattan plot of all SNPs in GWAS analysis with T3 levels. The y-axis shows the −log10 P values, and the x-axis shows their chromosomal positions. The red line indicates the threshold for significant hits (P = 5 × 10−8) while the blue line indicates the threshold for suggestive hits (P = 5 × 10−7)

Regional association plot showing suggestive locus for T4 serum levels in the SLC22A9 gene region. The most significant SNP is indicated in purple circle. The SNPs surrounding the most significant SNP are color-coded to reflect their LD with this SNP as in the inset (taken from pairwise r2 values from hg19/1000 Genomes Mar 2012 EUR database)
Within the same region, we detected a genome-wide significant variant (rs11822642) for T3/T4 ratio (P = 2.50 × 10−8, β = 0.83, SE = 0.15, MAF = 0.04, Table 2). SNP rs11822642 is located ~56 kb apart from the top SNP detected in T4 meta-analysis (rs12282281). Linkage disequilibrium (LD) between those two SNPs is r2 = 0.42. SNP rs11822642 is located between SLC22A9 and HRASLS5 genes on chromosome 11. The regional association plot for rs11822642 is presented in Fig. 3.

Regional association plot showing genome-wide significant locus in the SLC22A9 and HRASLS5 region. The most significant SNP is indicated in purple circle. The SNPs surrounding the most significant SNP are color-coded to reflect their LD with this SNP as in the inset (taken from pairwise r2 values from hg19/1000 Genomes Mar 2012 EUR database)
There were no other genome-wide significant loci for the T3/T4 ratio, but two suggestive ones were identified: rs4941659 (P = 1.26 × 10−7, β = 0.30, SE = 0.06) near KPNA3 gene, and rs12360138 (P = 3.59 × 10−7, β = −0.83, SE = 0.16) in ZMIZ1 gene. Their regional associations plots are presented in Supplemental Fig. 1.
For the T3 levels, we revealed 3 variants with suggestive evidence of association: rs4712793 (P = 6.09 × 10−8, β = 0.23, SE = 0.04) in intergenic region, rs116951285 (P = 6.25 × 10−8, β = −1.17, SE = 0.22) in RAB38 gene, rs101920634 (P = 2.65 × 10−7, β = −0.31, SE = 0.06) in PRKCE gene (Table 2). Their regional associations plots are presented in Supplemental Fig. 2.
Distributions of T4, T3, and T3/T4 per genotype of rs11822642 (genome-wide significant SNP in the T3/T4 analysis) and rs12282281 (suggestively associated SNP in the T4 analysis), both located in SLC22A9 region, are presented as box plots in Supplemental Fig. 3. Data shown in Supplemental Fig. 3 were derived from Split cohort where individuals with measures for both phenotypes, T4 and T3, were available. Genotype counts and mean values for all reported SNPs shown in Table 2 are presented in Supplementary Table 1.
Discussion
In this study, we performed the first GWAS meta-analysis of total T4 levels and identified a suggestive association with a locus encompassing SLC22A9 gene. In the same region, the genome-wide significant association was detected for the T3/T4 ratio in the Split cohort.
The variant showing the most significant association with T4 was an intron variant (rs12282281) within SLC22A9 gene. The allele G of the rs12282281 was associated with decreased levels of T4 in the serum. The SNP (rs11822642) showing the genome-wide significant association with the T3/T4 ratio is located ~56 kb apart and is in a moderate LD (r2 = 0.42 for the CEU population) with the T4-associated top SNP (rs12282281). The allele T of the rs11822642 was associated with the higher T3/T4 ratio (P = 2.11 × 10−8) and decreased levels of T4 levels (P = 0.00066). Individuals with T allele also tend to have increased T3 levels, although this was not shown to be significant.
SLC22A9 (also known as OAT7) is an organic anion transporter (OAT) that belongs to a superfamily of solute carriers (SLC) and mediates transport of a wide spectrum of molecules across cells, with predominant expression in the liver [24]. SLC22A9 was shown to transport steroid conjugates, estrone-3-sulfate (E3S) and dehydroepiandrosterone sulfate (DHEAS) in exchange for butyrate, and can mediate the exchange of sulfated organic components against short-chain fatty acids in hepatocytes [25]. Interestingly, all known TH transporter proteins are members of the same SLC gene superfamily as SLC22A9 [26], including organic anion transporter polypeptides (OATPs), monocarboxylate transporters MCT (SLC10A2 and SLC16A10), and the sodium/taurocholate cotransporting polypeptide (SLC10A1) [27, 28]. However, SLC22A9 has not yet been reported. SLC22A9, like other OATs, is predicted to have 12 α-helical transmembrane domains with intracellular termini showing a similar structure to SLC members OATPs [29]. Majority of OATPs facilitate uptake of THs. They are liver-specific proteins localized in the basolateral membrane of hepatocytes [30, 31], as well as SLC22A9. OATPs facilitate not only the transport of T4, T3, and rT3 but also their sulfates—T4S, T3S, and rT3S [32,33,34] as well as steroid conjugates (E3S and DHEAS) [35, 36], showing substrate similarity to SLC22A9. Compared to other OAT subtypes, SLC22A9 exhibits more specific substrates selectivity, specifically sulfate conjugates [25], and sulfation of THs is shown to be an important part of TH metabolism [37].
Polymorphisms in genes encoding TH transporters are likely to affect the transport function of these proteins and consequentially the TH concentrations [28]. However, most of the studies exploring the association of genetic polymorphisms of the TH transporters, and TH concentrations had limited sample sizes and inconsistent results [36,37,38,39]. Some basic and clinical studies suggest that although many TH transporters have been identified, there are other TH transports yet to be discovered [28]. The association of variants within SLC22A9 gene with T4 levels and T3/T4 ratio implies that SLC22A9 could be a novel TH transporter protein. However, its relevance in vivo needs to be shown. Moreover, the SLC22A9 is predominantly expressed in the liver where a large proportion of T4 is uptaken and being converted to T3 in hepatocytes [5]. Further analysis will be needed to clarify our findings. It should also be stressed that detected SNPs are low-frequency variants and studies with bigger sample size will be beneficial. Unfortunately, as we are not aware of any other genotyped cohorts with measurements of the T4 hormone, we could not replicate our findings.
This region includes other solute carrier genes—SLC22A10, SLC22A24, and SLC22A25—that are all part of the SLC gene superfamily. All these transporter genes, including SLC22A9, are encoded by the same gene cluster and are highly similar by sequence comparisons [40, 41]. SLC22A10 and SLC22A25 genes have restricted expression to the liver, while SLC22A24 was identified in the kidney [40, 42]. Exact substrates and functions of transporter proteins they encode remain to be clarified [43]. Ruth et al. reported an upstream genetic variant from SLC22A9 gene, located in SLC22A10, suggestively associated with progesterone levels in a GWAS of sex hormone-related phenotypes [44].
Apart from our main finding, we detected two suggestively associated loci with T3/T4 ratio and three with T3 levels. PRKCE encodes for a protein that belongs to a family of serine- and threonine-specific protein kinases. High PRKCE expression showed an association with papillary thyroid tumor development [45]. ZMIZ1 encodes a member of the PIAS (protein inhibitor of activated STAT) family of proteins that regulate the activity of various transcription factors [46]. Tuccilli et al. demonstrated that the expression of ZMIZ1 was deregulated in most PTC tissues, likely contributing to the tumor progression [47]. Other suggestively associated genes do not have a clear connection with the physiology of the thyroid gland. RAB38 plays an important role in the control of melanin production and melanosome biogenesis [48] and the maturation of phagosomes [49]. KPNA3 encodes a protein that belongs to the importin alpha family and is involved in nuclear protein import [50].
The main limitations of our study are the absence of a suitable replication cohort for the total TH analyses and modest sample size. On the other hand, the strength of our study represents the careful selection of participants. Since we had available phenotype information on measurements of fT3, fT4, TSH, Tg, TgAb, and TPOAb, we excluded all individuals whose hormone values were not within the reference range, or had positive TPO or Tg autoantibodies, leaving only healthy individuals with no thyroid dysfunction. Likewise, the study sample represented the ethnically homogeneous Croatian population. In any case, further research is needed to confirm our findings and to discover additional genetic variants underlying total TH levels.
In conclusion, our study revealed a novel association of SLC22A9 genetic variants with T4 levels and T3/T4 ratio. This is an interesting finding from a biological perspective since SLC22A9 encodes for a transport protein found predominantly in the liver where a large amount of T4 is uptaken by tissue cells to be converted to T3. Moreover, all known TH transport proteins belong to the same superfamily as SLC22A9. To clarify SLC22A9 role in TH transport, replication of our findings is needed as well as studies exploring its relevance in vivo.
References
Panicker V. Genetics of thyroid function and disease. Clin Biochem Rev. 2011;32:165–75.
Mondal S, Raja K, Schweizer U, Mugesh G. Chemistry and biology in the biosynthesis and action of thyroid hormones. Angew Chem Int Ed Engl. 2016;55:7606–30.
Hoermann R, Midgley JE, Larisch R, Dietrich JW. Relational stability in the expression of normality, variation, and control of thyroid function. Front Endocrinol. 2016;7:142.
Dayan CM, Panicker V. Novel insights into thyroid hormones from the study of common genetic variation. Nat Rev Endocrinol. 2009;5:211–8.
Larsen PR, Zavacki AM. Role of the iodothyronine deiodinases in the physiology and pathophysiology of thyroid hormone action. Eur Thyroid J. 2013;1:232–42.
Wilkin TJ, Isles TE. The behavior of the triiodothyronine/thyroxine (T3/T4) ratio in normal individuals, and its implications for the regulation of euthyroidism. J Endocrinol Investig. 1984;7:319–22.
Mortoglou A, Candiloros H. The serum triiodothyronine to thyroxine (T3/T4) ratio in various thyroid disorders and after Levothyroxine replacement therapy. Hormones. 2004;3:120–6.
Medici M, van der Deure WM, Verbiest M, Vermeulen SH, Hansen PS, Kiemeney LA, et al. A large-scale association analysis of 68 thyroid hormone pathway genes with serum TSH and FT4 levels. Eur J Endocrinol. 2011;164:781–8.
Panicker V, Wilson SG, Spector TD, Brown SJ, Falchi M, Richards JB, et al. Heritability of serum TSH, free T4 and free T3 concentrations: a study of a large UK twin cohort. Clin Endocrinol. 2008;68:652–9.
Martin LJ, Crawford MH. Genetic and environmental components of thyroxine variation in Mennonites from Kansas and Nebraska. Hum Biol. 1998;70:745–60.
Samollow PB, Perez G, Kammerer CM, Finegold D, Zwartjes PW, Havill LM, et al. Genetic and environmental influences on thyroid hormone variation in Mexican Americans. J Clin Endocrinol Metab. 2004;89:3276–84.
Nielsen TR, Appel EV, Svendstrup M, Ohrt JD, Dahl M, Fonvig CE, et al. A genome-wide association study of thyroid stimulating hormone and free thyroxine in Danish children and adolescents. PLoS One. 2017;12:e0174204.
Porcu E, Medici M, Pistis G, Volpato CB, Wilson SG, Cappola AR, et al. A meta-analysis of thyroid-related traits reveals novel loci and gender-specific differences in the regulation of thyroid function. PLoS Genet. 2013;9:e1003266.
Rudan I, Marušić A, Janković S, Rotim K, Boban M, Lauc G, et al. “10 001 Dalmatians:” Croatia launches its national biobank. Croat Med J. 2009;50:4–6.
Matana A, Brdar D, Torlak V, Boutin T, Popović M, Gunjača I, et al. Genome-wide meta-analysis identifies novel loci associated with parathyroid hormone level. Mol Med. 2018;24:15.
Matana A, Popovic M, Boutin T, Torlak V, Brdar D, Gunjaca I, et al. Genome-wide meta-analysis identifies novel gender specific loci associated with thyroid antibodies level in Croatians. Genomics. 2018;18:30242–8.
Reinehr T, Andler W. Thyroid hormones before and after weight loss in obesity. Arch Dis Child. 2002;87:320–3.
Aulchenko YS, Ripke S, Isaacs A, van Duijn CM. GenABEL: an R library for genome-wide association analysis. Bioinformatics. 2007;23:1294–6.
Marchini J, Howie B, Myers S, McVean G, Donnelly P. A new multipoint method for genome-wide association studies by imputation of genotypes. Nat Genet. 2007;39:906–13.
Willer CJ, Li Y, Abecasis GR. METAL: fast and efficient meta-analysis of genomewide association scans. Bioinformatics. 2010;26:2190–1.
Pruim RJ, Welch RP, Sanna S, Teslovich TM, Chines PS, Gliedt TP, et al. LocusZoom: regional visualization of genome-wide association scan results. Bioinformatics. 2010;26:2336–7.
Ruffier M, Kähäri A, Komorowska M, Keenan S, Laird M, Longden I, et al. Ensembl core software resources: storage and programmatic access for DNA sequence and genome annotation. Database. 2017;2017:bax020.
Turner SD. qqman: an R package for visualizing GWAS results using Q–Q and Manhattan plots. J Open Source Softw. 2014;3:731.
Koepsell H. The SLC22 family with transporters of organic cations, anions and zwitterions. Mol Asp Med. 2013;34:413–35.
Shin HJ, Anzai N, Enomoto A, He X, Kim DK, Endou H, et al. Novel liver-specific organic anion transporter OAT7 that operates the exchange of sulfate conjugates for short chain fatty acid butyrate. Hepatology. 2007;45:1046–55.
Schweizer U, Johannes J, Bayer D, Braun D. Structure and function of thyroid hormone plasma membrane transporters. Eur Thyroid J. 2014;3:143–53.
Bernal J, Guadano-Ferraz A, Morte B. Thyroid hormone transporters—functions and clinical implications. Nat Rev. 2015;11:406–17.
Visser WE, Friesema EC, Visser TJ. Minireview: thyroid hormone transporters: the knowns and the unknowns. Mol Endocrinol. 2011;25:1–14.
Roth M, Obaidat A, Hagenbuch B. OATPs, OATs and OCTs: the organic anion and cation transporters of the SLCO and SLC22A gene superfamilies. Br J Pharmacol. 2012;165:1260–87.
Hsiang B, Zhu Y, Wang Z, Wu Y, Sasseville V, Yang WP, et al. A novel human hepatic organic anion transporting polypeptide (OATP2). Identification of a liver-specific human organic anion transporting polypeptide and identification of rat and human hydroxymethylglutaryl-CoA reductase inhibitor transporters. J Biol Chem. 1999;274:37161–8.
Konig J, Cui Y, Nies AT, Keppler D. A novel human organic anion transporting polypeptide localized to the basolateral hepatocyte membrane. Am J Physiol Gastrointest Liver Physiol. 2000;278:G156–64.
Fujiwara K, Adachi H, Nishio T, Unno M, Tokui T, Okabe M, et al. Identification of thyroid hormone transporters in humans: different molecules are involved in a tissue-specific manner. Endocrinology. 2001;142:2005–12.
Kullak-Ublick GA, Ismair MG, Stieger B, Landmann L, Huber R, Pizzagalli F, et al. Organic anion-transporting polypeptide B (OATP-B) and its functional comparison with three other OATPs of human liver. Gastroenterology. 2001;120:525–33.
van der Deure WM, Peeters RP, Visser TJ. Molecular aspects of thyroid hormone transporters, including MCT8, MCT10, and OATPs, and the effects of genetic variation in these transporters. J Mol Endocrinol. 2010;44:1–11.
Pizzagalli F, Varga Z, Huber RD, Folkers G, Meier PJ, St-Pierre MV. Identification of steroid sulfate transport processes in the human mammary gland. J Clin Endocrinol Metab. 2003;88:3902–12.
van der Deure WM, Hansen PS, Peeters RP, Kyvik KO, Friesema ECH, Hegedüs L, et al. Thyroid hormone transport and metabolism by organic anion transporter 1C1 and consequences of genetic variation. Endocrinology. 2008;149:5307–14.
van der Deure WM, Friesema ECH, de Jong FJ, de Rijke YB, de Jong FH, Uitterlinden AG, et al. Organic anion transporter 1B1: an important factor in hepatic thyroid hormone and estrogen transport and metabolism. Endocrinology. 2008;149:4695–701.
Roef GL, Rietzschel ER, De Meyer T, Bekaert S, De Buyzere ML, Van daele C, et al. Associations between single nucleotide polymorphisms in thyroid hormone transporter genes (MCT8, MCT10 and OATP1C1) and circulating thyroid hormones. Clin Chim Acta. 2013;425:227–32.
Lago-Leston R, Iglesias MJ, San-Jose E, Areal C, Eiras A, Araujo-Vilar D, et al. Prevalence and functional analysis of the S107P polymorphism (rs6647476) of the monocarboxylate transporter 8 (SLC16A2) gene in the male population of north-west Spain (Galicia). Clin Endocrinol. 2009;70:636–43.
Jacobsson JA, Haitina T, Lindblom J, Fredriksson R. Identification of six putative human transporters with structural similarity to the drug transporter SLC22 family. Genomics. 2007;90:595–609.
Nigam SK, Bush KT, Martovetsky G, Ahn S-Y, Liu HC, Richard E, et al. The organic anion transporter (OAT) family: a systems biology perspective. Physiol Rev. 2015;95:83–123.
Sun W, Wu RR, van Poelje PD, Erion MD. Isolation of a family of organic anion transporters from human liver and kidney. Biochem Biophys Res Commun. 2001;283:417–22.
Volk C. OCTs, OATs, and OCTNs: structure and function of the polyspecific organic ion transporters of the SLC22 family. Wiley Interdiscip Rev: Membr Transp Signal. 2014;3:1–13.
Ruth KS, Campbell PJ, Chew S, Lim EM, Hadlow N, Stuckey BG, et al. Genome-wide association study with 1000 genomes imputation identifies signals for nine sex hormone-related phenotypes. Eur J Hum Genet. 2016;24:284–90.
Zhang X, Li D, Li M, Ye M, Ding L, Cai H, et al. MicroRNA‐146a targets PRKCE to modulate papillary thyroid tumor development. Int J Cancer. 2014;134:257–67.
Li X, Thyssen G, Beliakoff J, Sun Z. The novel PIAS-like protein hZimp10 enhances Smad transcriptional activity. J Biol Chem. 2006;281:23748–56.
Tuccilli C, Baldini E, Sorrenti S, Di Gioia C, Bosco D, Ascoli V, et al. Papillary thyroid cancer is characterized by altered expression of genes involved in the sumoylation process. J Biol Regul Homeost Agents. 2015;29:655–62.
Gerondopoulos A, Langemeyer L, Liang JR, Linford A, Barr FA. BLOC-3 mutated in Hermansky–Pudlak syndrome is a Rab32/38 guanine nucleotide exchange factor. Curr Biol. 2012;22:2135–9.
Seto S, Tsujimura K, Koide Y. Rab GTPases regulating phagosome maturation are differentially recruited to mycobacterial phagosomes. Traffic. 2011;12:407–20.
Takeda S, Fujiwara T, Shimizu F, Kawai A, Shinomiya K, Okuno S, et al. Isolation and mapping of karyopherin alpha 3 (KPNA3), a human gene that is highly homologous to genes encoding Xenopus importin, yeast SRP1 and human RCH1. Cytogenet Cell Genet. 1997;76:87–93.
Acknowledgements
The Croatian Science Foundation funded this work under the project “Identification of new genetic loci implicated in the regulation of thyroid and parathyroid function” (Grant 1498). The “10 001 Dalmatians” project was funded by the Medical Research Council UK, The Croatian Ministry of Science, Education and Sports (Grant 216-1080315-0302), and the Croatian Science Foundation (Grant 8875).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Gunjača, I., Matana, A., Boutin, T. et al. Genome-wide association meta-analysis for total thyroid hormone levels in Croatian population. J Hum Genet 64, 473–480 (2019). https://doi.org/10.1038/s10038-019-0586-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s10038-019-0586-4
