
Abstract
Basal cell nevus syndrome (BCNS) is an autosomal dominant disorder most commonly caused by a germline mutation in the PTCH1 gene. PTCH1 is known to have different isoforms with different functional properties and expression patterns among tissues. We detected a novel, pathogenic de novo mutation in PTCH1 isoform 1b (c.114delG) in a BCNS patient. Furthermore, we elucidated the specific expression pattern of PTCH1 isoforms in normal skin, BCC and peripheral blood by studying expression of different PTCH1 isoforms. Human skin showed expression of isoforms 1b and 1d, while peripheral blood additionally showed 1a and 1e expression. BCCs showed expression of all isoforms. Here we report a patient with a novel, isoform 1b specific mutation in PTCH1 and thereby distinguish PTCH1 isoform 1b as the major transcript in the development of BCNS.
Similar content being viewed by others


Introduction
Basal cell nevus syndrome (BCNS; MIM #109400) is an autosomal dominant disorder characterized by multiple basal cell carcinomas (BCCs) [1]. Molecular pathogenesis of BCNS is based on mutations in constituents of the hedgehog (Hh) pathway, leading to aberrant signaling. Inactivating mutations in tumor suppressor PTCH1 (Chr9q22.32) are most often the culprit in BCC. Although homozygous mutations are lethal in mouse embryos, heterozygous mutations in human result in congenital deformations and a higher risk of developing cutaneous BCCs due to loss of heterozygosity later in life [2, 3]. PTCH1 has different isoforms with specific spatial temporal expression properties. Isoforms differ in the 5′ coding regions and consequently the translated N-terminus of the protein [4]. Different isoforms are distinguished in which protein isoform L (PTCH1b) contains a unique 67 amino acid N-terminal sequence, which is missing in protein isoform L′ (PTCH1a’) and M (PTCH1a). The shorter protein isoform S, encoded by PTCH1 exon 1c, 1c′, 1d, and 1e lacks the entire N-terminus and therefore the first transmembrane region [4]. Schematic representation of the different isoforms of PTCH1 is shown in Fig. 1.

a Schematic representation of PTCH1 specific isoforms. Only different exons 1 and mutual exons 2 and 3 are depicted. Orientation is from 5′ to 3′ indicated with an arrowed-line. The start codon is given by a hooked arrow. b Translated PTCH1 protein from different isoforms. Isoform M is translated from transcript 1a (NCBI RefSeq: NM_001083602.2), isoform L′ from transcript 1a′ (NM_001083603.2), isoform L from transcript 1b (NM_000264.4) and isoform S from transcripts c (NM_001083604.2), c′ (NM_001083605.2), d (NM_001083606.2) and e (NM_001083607.2)
Differences in the N-terminus are responsible for the variable capabilities of inhibiting smoothened (SMO) [5]. Due to these differences in protein structure most isoforms can only partially inhibit SMO. Only isoform 1b (protein isoform L) is known to be capable of complete SMO inhibition [6]. The expression of different isoforms varies per tissue type and developmental stage, suggesting a specific role for each isoform in organogenesis [4,5,6]. Recently, contribution of aberrant Hh signaling due to PTCH1 mutations was found in ocular developmental anomalies [7]. This includes a heterozygous frameshift mutation specific for isoform 1a′ (c.4delG) resulting in ocular features overlapping with the BCNS phenotype. The specific expression patterns in human skin is largely unknown. Because of the importance of Hh signaling in human skin, the expression levels of isoform specific mutations could be of major influence on the development of basal cell carcinoma.
Case report
Here, we describe a 9-year-old Finish boy with macrocephaly (+4 SD), bifid and fused ribs (permission was not given to publish photographs). He showed no calcification of the falx cerebri and so far had developed no basal cell carcinomas, palmoplantar pits or odontogenic keratocysts, clinical features usually appearing in puberty [8]. Based on the clinical criteria by Kimonis et al. we considered the diagnosis of BCNS and performed PTCH1 mutation analysis [9, 10]. The parents and his older brother had no clinical features of BCNS.
Methods
Genomic DNA of the boy and his parents was isolated (Wizard Genomic DNA purification kit, Promega) and PTCH1 coding exons (based on RefSeq: NM_000264.4 (1b), NM_001083603.2 (1a′), NM_001083602.2 (1a) and exon numbering by Nagao et al. [4]) of the proband were Sanger sequenced (BigDye v1.1 sequencing kit, ABI3730 DNA analyzer, Applied Biosystems, primer sequences on request). Targeted sequence analysis for the PTCH1 mutation was performed for the parents and non-paternity was excluded using polymorphic markers (AmpFISTR Identifiler PCR Amplification kit, Life Technologies). The variant has been submitted to the PTCH1 locus specific database (LSDB) of the Leiden Open Variant Database (LOVD 3.0, http://www.lovd.nl), with individual ID 00086975. To correlate the isoform expression level to other tissues in human, isoform expression experiments were conducted by analysis of RNA, isolated from three nodular basal cell carcinomas of a patient with previously confirmed different inactivating PTCH1 mutations, three samples derived from healthy human skin and two samples from peripheral blood of healthy controls. RNA was isolated using Trizol (Life Technologies) and equal RNA concentrations reverse transcribed into cDNA (Quanta qScript cDNA Supermix, Quanta Biosciences). cDNA synthesis and expression was checked with exonic PTCH1 primers located in 3 and 5. Subsequently, the constitution of the expressed PTCH1 isoforms was analysed by separately PCR (Amplitaq 360, Clontech) amplifying each isoform using specific forward primers in exon 1 combined with a shared exon 2 reverse primer [4]. Primer sequences are listed in supplemental table S1 and isoform specific first exon sequences are shown in supplemental figure S1. Results were visualized using conventional gel-electrophoresis.
Results
Molecular analysis on DNA of the symptomatic male patient identified a novel heterozygous mutation in exon 1, c.114delG (Fig. 2), specific for isoform 1b of the PTCH1 gene (NCBI RefSeq: NM_000264.4). The mutation could not be detected in both parents and non-paternity was excluded. The de novo mutation putatively results in a frameshift and premature truncation of the protein (p.(Leu39Cysfs*41)). The mutation may also result in nonsense mediated mRNA decay. The mutated region is highly conserved among species and no other pathogenic mutations have been previously reported in this exon.

PTCH1 mutation in isoform 1b specific transcript. Top panel, part of exon 1b PTCH1 sequence trace of a control individual and lower panel sequence trace of the patient across the mutation c.114delG (arrow). Sequence are in reverse complement orientation with nucleotide codes shown underneath (S; G or C, K; G or T, Y; C or T). Variant has been submitted to the PTCH1 locus specific database (LSDB) of the Leiden Open Variant Database (LOVD 3.0), ID number 00086975
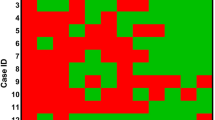
Considering the importance of the Hh pathway in skin, expression patterns of specific isoforms were determined. In case of tissue specific isoform expression, predictions could be made regarding the effect of isoform specific mutations. Our analysis on tissue samples of control patients (healthy skin, cutaneous BCCs and whole peripheral blood) for specific PTCH1 isoforms as part of overall expressed transcript (exon 3–5 amplification, not shown), showed only expression of isoform 1b and 1d in normal skin, while in cutaneous basal cell carcinoma all isoforms were expressed. In peripheral blood, PTCH1 isoform 1b, 1d, 1e, and 1a are expressed (Fig. 3).

Gel-electrophoresis of PCR products from isoform specific cDNA, Lanes 1, 4, 7, 10, 13, and 16 represent healthy skin, lanes 2, 5, 8, 11, 14, and 17 represent BCC tumor and lanes 3, 6, 9, 12, 15, and 18 represent peripheral blood. Specific isoform 1a amplification in lanes 1–3, isoform 1a′ (together with 1a) lanes 4–6, isoform 1b lanes 7–9, isoform 1c (together with 1c’) lanes 10-12, isoform 1d lanes 13–15 and isoform 1e lanes 16–18. Marker lanes are indicated with M shown on the left and right. Experiments were done in triplicate with the same results. All no template controls were negative and non-isoform specific PTCH1 reverse transcribed PCR, positive (data not shown)
Discussion
BCNS can be diagnosed on clinical features [9, 10]. Although there is no clear genotype/phenotype correlation, clinical criteria often match with identification of genetic mutations [8]. However, molecular diagnosis is the gold standard and advised [10]. In the described case only minor BCNS criteria were seen (macrocephaly and bifid/fused ribs) and genetic PTCH1 analysis was used to confirm BCNS. Validating the de novo occurrence of the mutation by excluding presence in both parents further strengthens pathogenicity and refines additional genetic counseling. The identified exon 1b mutation c.114delG is novel and specific for only isoform 1b of PTCH1. Of the presently more than 410 reported unique mutations distributed throughout the PTCH1 gene (Leiden Open Variation Database 3.0), none have been located in exon 1. Suzuki et al. identified a de novo mutation in exon 2 and suggested that isoforms PTCH1-1c, PTCH1-1d, and PTCH1-1e (PTCHS protein) are probably dispensable [11]. They proposed that only the longer isoforms 1b, 1a and 1a′ are associated with BCNS. Furthermore, the association between ocular developmental anomalies and PTCH1 mutations, including one specific for isoform 1a′ increases the likelihood of an important role of the longer isoforms of PTCH1 in embryonal development. By identifying a PTCH1 isoform 1b mutation we strengthened the hypothesis that this particular isoform is the major transcript in the development of BCNS [10]. To the best of our knowledge this is the first report of a PTCH1 mutation in isoform 1b.
In our normal control skin samples, isoform 1b and 1d are expressed; indicating that both the full-length protein isoform L and the truncated isoform S are present. This partially conflicts with the results reported by Kogerman et.al, who could not detect isoform 1b in normal skin, but only protein S related isoforms [12]. In the basal cell carcinomas we analyzed, isoforms 1a, 1a′, 1b, 1c(c’), 1d and 1e are expressed. Although Kogerman et al. found 1b, 1d and 1e expression in BCC, the expression of gene isoforms capable of being translated into the other protein isoforms (M and L′ respectively) has not been shown before [12]. This is especially interesting because at least protein isoform M seems to be capable of inhibiting Gli transcription and inducing apoptosis [4].
In whole blood of a healthy individual, isoform 1a, 1b, 1d, and 1e are expressed. Of those, isoform 1a and 1e are not expressed in healthy skin. Differential expression between various tissues are consistent with previous findings [4,5,6]. Probably, the subtleties needed for silencing the Hh pathway in case of tissue polarization are essential for fetal development as can be seen in BCNS and ocular anomalies, but largely dispensable after birth.
The difference in expression patterns in BCCs show that other isoforms can still be expressed. As some PTCH1 isoform promoters are known to have GLI-binding sequences and therefore responsive to GLI in driving inhibition of SMO, it is tempting to speculate that isoforms might be capable of compensating the lack of a specific PTCH1 isoform in case of an isolated loss of function mutation [4,5,6, 13]. Expression of those different isoforms could be initiated as a result of the feed-back mechanism through the functional GLI binding sites in the promoter regions of PTCH1. Theoretically, this compensation mechanism could be at least partially responsible for slowing down the growth in BCC, especially in case of upregulation of any of the longer and probably most functional isoforms; 1a′, 1a and in particular 1b. In case of an exon 1b mutation, the effect of compensating isoform expression is likely to be incomplete, since isoform 1b is the only isoform capable of sustained suppression of SMO activation.
Consequences of isoform specific mutations are hard to predict, since the clinical features of BCNS are highly variable and the temporal and special expression patterns are largely unknown, as is the degree of inhibition reached by upregulation of different isoforms. Although loss of heterozygosity is needed for development of BCCs, PTCH1 haploinsufficiency during embryogenesis seems to be sufficient for the development of typical congenital BCNS features. So unfortunately, for our young patient with an isolated PTCH1 isoform 1b mutation, it is not possible to predict the development of other clinical features of BCNS later in life.
References
John AM, Schwartz RA. Basal cell naevus syndrome: an update on genetics and treatment. Br J Dermatol. 2016;174:68–76.
Goodrich LV, Milenkovic L, Higgins KM, Scott MP. Altered neural cell fates and medulloblastoma in mouse patched mutants. Science. 1997;277:1109–13.
Hahn H, Wojnowski L, Zimmer AM, Hall J, Miller G, Zimmer A. Rhabdomyosarcomas and radiation hypersensitivity in a mouse model of Gorlin syndrome. Nat Med. 1998;4:619–22.
Nagao K, Toyoda M, Takeuchi-Inoue K, Fujii K, Yamada M, Miyashita T. Identification and characterization of multiple isoforms of a murine and human tumor suppressor, patched, having distinct first exons. Genomics. 2005;85:462–71.
Shimokawa T, Svard J, Heby-Henricson K, Teglund S, Toftgard R, Zaphiropoulos PG. Distinct roles of first exon variants of the tumor-suppressor Patched1 in Hedgehog signaling. Oncogene. 2007;26:4889–96.
Shimokawa T, Rahnama F, Zaphiropoulos PG. A novel first exon of the Patched1 gene is upregulated by Hedgehog signaling resulting in a protein with pathway inhibitory functions. FEBS Lett. 2004;578:157–62.
Chassaing N, Davis EE, McKnight KL, Niederriter AR, Causse A, David V, et al. Targeted resequencing identifies PTCH1 as a major contributor to ocular developmental anomalies and extends the SOX2 regulatory network. Genome Res. 2016;26:474–85.
Jones EA, Sajid MI, Shenton A, Evans DG. Basal cell carcinomas in gorlin syndrome: a review of 202 patients. J Skin Cancer. 2011;2011:217378.
Kimonis VE, Goldstein AM, Pastakia B, Yang ML, Kase R, DiGiovanna JJ, et al. Clinical manifestations in 105 persons with nevoid basal cell carcinoma syndrome. Am J Med Genet. 1997;69:299–308.
Bree AF, Shah MR, Group BC. Consensus statement from the first international colloquium on basal cell nevus syndrome (BCNS). Am J Med Genet A. 2011;155A:2091–7.
Suzuki M, Hatsuse H, Nagao K, Takayama Y, Kameyama K, Kabasawa Y, et al. Selective haploinsufficiency of longer isoforms of PTCH1 protein can cause nevoid basal cell carcinoma syndrome. J Hum Genet. 2012;57:422–6.
Kogerman P, Krause D, Rahnama F, Kogerman L, Unden AB, Zaphiropoulos PG, et al. Alternative first exons of PTCH1 are differentially regulated in vivo and may confer different functions to the PTCH1 protein. Oncogene. 2002;21:6007–16.
Agren M, Kogerman P, Kleman MI, Wessling M, Toftgard R. Expression of the PTCH1 tumor suppressor gene is regulated by alternative promoters and a single functional Gli-binding site. Gene. 2004;330:101–14.
Acknowledgements
We are grateful to Carolien N. van Oosterhoud, Renske Janssen and Anja R.M. Steyls for technical assistance.
Author contributions:
RG and MR conducted the research and have written the paper, MvG and KM have supervised the project, adjusted writing and are responsible for the overall content, HK identified and counseled the patient and family, AP provided the DNA diagnostics.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Gielen, RJ.C.A.M., Reinders, M.G.H.C., Koillinen, H.K. et al. PTCH1 isoform 1b is the major transcript in the development of basal cell nevus syndrome. J Hum Genet 63, 965–969 (2018). https://doi.org/10.1038/s10038-018-0485-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s10038-018-0485-0
This article is cited by
-
A novel splicing mutation of PTCH1 in a Chinese family with nevoid basal cell carcinoma syndrome
Medical Molecular Morphology (2019)
