
Abstract
Background:
Fragile X syndrome (FXS) is the most common cause of inherited intellectual disabilities and autism. The reported prevalence of the full mutation (FM) gene FMR1 in the general population is 0.2–0.4 per 1000 males and 0.125–0.4 per 1000 females.
Population screening for FMR1 expanded alleles has been performed in newborns and in an adult population. However, it has never been carried out in an entire town.
Ricaurte is a Colombian district with 1186 habitants, with a high prevalence of FXS, which was first described by cytogenetic techniques in 1999.
Methods:
Using a PCR-based approach, screening for FXS was performed on blood spot samples obtained from 926 (502 males and 424 females) inhabitants from Ricaurte, accounting for 78% of total population.
Results:
A high prevalence of carriers of the expanded allele was observed in all FXS mutation categories. Using the Bayesian methods the carrier frequency of FM was 48.2 (95% Credibility Region CR: 36.3–61.5) per 1000 males and 20.5 (95% CR:13.5–28.6) per 1000 females; the frequency of premutation carrier was 14.1 (95% RC: 8.0–21.7) per 1000 males (95% RC: 8.0–21.7 per 1000 males) and 35.9 (95% RC: 26.5–46.2) per 1000 for females (95% RC: 26.5–46.2 per 1000 females), and gray zone carrier was 13.4 (95% RC: 7.4–20.7) per 1000 males (95% RC: 7.4–20.7 per 1000 males) and 42.2 (95% RC: 32.2–53.8) per 1000 for females (95% RC: 32.2–53.8 per 1000 females). Differences in carrier frequencies were observed for premutation and FM alleles between natives and non-natives.
Conclusions:
This study shows that in Ricaurte the carrier frequencies of FMR1 expanded alleles (premutations and FMs) are higher than those reported in the literature, suggesting that Ricaurte constitutes a genetic cluster of FXS.
Similar content being viewed by others

Introduction
Fragile X syndrome (FXS) is the most common leading etiology of inherited intellectual disabilities (IDs) and autism spectrum disorders (ASD). FXS is inherited as an X-linked pattern and caused by an abnormal expansion of the trinucleotide CGG repeat located in the promoter region of the FMR1 gene at Xq27.3.
Individuals with more than 200 repeats are affected by FXS and present with a classic phenotype characterized by IDs, ranging from mild to moderate, in addition to behavioral and physical features, such as attention-deficit hyperactivity disorder (ADHD), anxiety, aggression, large and protruding ears, hyperextensible finger joints, and macroorchidism [1]. Furthermore, approximately 60–70% of individuals with FXS present with ASD [2]. Females affected with FXS have a less severe ID than males. Approximately 30–50% of affected females show normal intellectual functioning [3].
Premutation carriers, harboring an allele with 55–200 repeats, are generally not affected with the classic FXS phenotype; however, they are at risk of developing the late-onset neurological disorder, the fragile X-associated tremor ataxia syndrome (FXTAS), which affects approximately 40% of older male carriers, and approximately 8–16% of older female carriers. In addition, female premutation carriers are at risk to develop the fragile X-associated primary ovarian insufficiency (FXPOI) that occurs in approximately 20% of female carriers compared to 1% in the general population [4,5,6]. Furthermore, some premutation carriers can develop ASD, seizures, learning disabilities, anxiety, depression, ADHD, and visual perceptual deficits [6,7,8].
The reported prevalence of the full mutation (FM) carrier (>200 CGG repeats in FMR1) in the general population is 0.2–0.4 per 1000 males and 0.125–0.4 per 1000 females [9,10,11,12]. However, reports of the prevalence of carriers of intermediate, premutation, and FM alleles differ among studies according to sample size, definition of CGG repeat size categories, DNA diagnostic test used, and population/ethnic groups studied. In addition, the type of screening such as newborns, screening of children in special education settings, and screening of pregnant volunteer adults with or without a history of ID in their family will influence the prevalence [9, 11]. Hunter and colleagues (2014) reported in a systematic literature review and meta-analysis of published prevalence studies in the general population based on DNA testing using PCR and/or Southern blotting techniques. They found that a prevalence of the FM allele carrier was 0.14 per 1000 males and 0.09 per 1000 females. The prevalence of carriers of PM alleles was 1.2 per 1000 males and 3.4 per 1000 females [13].
Population screening for FXS in newborns or in an adult population with ID has been carried out [9,10,11, 14–16].
Several newborn screening studies have been conducted on blood spot cards and used to identify the FM in males in different countries including United States, Canada, Spain, and Taiwan [9, 10, 17,18,19]. Coffee et al. [10] used a quantitative methylation-sensitive PCR-based approach (Q-MSP) to screen 36,124 de-identified newborn males in the United States and estimated that the prevalence of FXS in the general population was 0.19 per 1000 males (95% confidence interval: 0.09–0.4 per 1000 males) [10]. Although less expensive than Southern Blot, the Q-MSP, which could be performed on blood spot samples, does not allow the identification of gray zone and premutation alleles, which have clinical importance in terms of genetic counseling and risk of developing FXTAS and FXPOI [20, 21]; furthermore, it cannot identify females with the FM, who may not have ID, but require genetic counseling.
Tassone et al. [9, 11] in 2012 and in 2015 described a PCR technique, using a CGG-specific primer in addition to the FMR1-specific primers lying outside the CGG repeat element. By testing 14,207 newborns (7312 males and 6895 females) they found that the prevalence of gray zone allele carrier was 15.2 per 1000 females and 8.9 per 1000 males, while the prevalence of premutation allele carrier was 4.78 per 1000 females and 2.33 per 1000 males. Only one case with the FM was identified in 7312 newborn males [9].
Currently, in Colombia, there are no data about the prevalence of expanded allele carrier of the FMR1 gene. A Colombian district, Ricaurte (see Fig. 1), which is located in the north region of Valle del Cauca province (or department), has severe economic limitations and poor access to health services. With a population of 1186 habitants, Ricaurte has been historically recognized because many of its inhabitants have ID. At the end of the 1990s, using a cytogenetic approach, we performed a study of 44 subjects who were clinically evaluated and 28 of them were tested for FXS by means of karyotyping. This led to the diagnosis of 19 patients with FXS without any premutation carrier identified (26.3 per 1000 males and 10 per 1000 females) [22].

Location of Ricaurte. Ricaurte is a district located in the north of South America, southwest of Colombia in a province called Valle del Cauca. This district is approximately 240 km from Bogota, Colombian capital.
Thus, the objective of this study was to determine the carrier frequency of different allele categories of the FMR1 gene by carrying out a population screening of the entire population of the town of Ricaurte (Colombia). Our findings suggest that Ricaurte represents a genetic cluster of FXS.
Materials and methods
Subjects
This screening study included 1186 inhabitants of Ricaurte, a semi-rural district which belongs to the municipality of Bolívar, located in the north region of Valle del Cauca´s department (province) in Colombia. All of the elderly and underage people who gave permission with an inform consent signed by the legal representative and/or themselves were included in the study. This study was approved by local health authorities of Ricaurte (Bolívar) and with the authorization of the Institutional Review Board (IRB) of the School of Health of Universidad del Valle (Cali, Colombia), with the approval number 016–014.
Being a native of Ricaurte was defined through the survey by the answer of the following question “When you were born, did your father or mother live in Ricaurte?” If the answer was positive, the participant was defined as a native of Ricaurte. If the answer was no, the subject was considered as non-native of Ricaurte.
Previous to the beginning of the study, several steps were taken including engaging community members directly affected by fragile X-associated disorders and their families, community leaders, government officials, local priest, and health services officials using Community-Based Participatory Research (CBPR) principles such as trust, respect, clear communication on roles, and shared mission (see online supplementary material).
Trained personnel visited each and every one of the houses in the town, doing the survey and taking socio-demographic data, identifying if participants were or non-native of Ricaurte, and if in their family there was any suspicion of FXS.
A signature of the informed consent was requested before taking the blood sample through a digit puncture. The blood sample was collected on blood spot cards and labeled with the unique individual code. Samples were shipped to the Molecular Biology Lab of the MIND Institute at the University of California at Davis Medical Center (UCDMC), where the molecular test for FXS screening was performed. Participants provided informed consent according to protocols approved by the IRB.
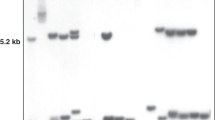
Blood spot screening: CGG sizing by PCR analysis
Samples were collected on 903 paper (Whatman Inc.). DNA was isolated from two punches using the QIAxtractor (Qiagen) as per the manufacturer's instructions. PCR analysis was performed using the AmplideXFMR1 reagent kit (Asuragen Inc. as previously reported [9, 23]. Allele sizing was obtained by running the PCR products on capillary electrophoresis and analysis was performed using the ABI Genescan analysis software. Genomic DNA was isolated from peripheral blood leukocytes for follow-up FXS molecular diagnosis for those subjects for whom an expanded allele was identified by PCR screening. DNA was isolated using standard procedure (Qiagen, Valencia, CA) and confirmatory DNA testing was performed using PCR and Southern blot analysis as detailed in Tassone et al. (2008) [24] and Filipovic-Sadic et al. [23]. Mutation categories were as described in Maddalena et al. [25].
Statistical analysis
Among the blood sampled subjects, the carrier frequency of each Fragile X allele (i.e. FM, premutation, and gray zone) was calculated using the ratio of the number of subjects with the mutation over the number of bleed subjects, according to each sex and origin (native, non-native, and total; see Table 1). The prevalence of carriers of each FMR1 allele obtained in Ricaurte was compared with the prevalence values reported in Hunter et al. (2014), meta-analysis adding up the overall prevalence of FM and premutation allele carrier throughout the studies belonging to that meta-analysis [13]; and against the values reported in Tassone et al. (2012) for the carrier frequency of gray zone alleles [9], obtaining the odds ratios (OR) of carrier frequencies which reflect the increased ratio of frequencies in Ricaurte (Colombia) in relation to the referenced articles. Additionally, 95% confidence intervals (95% C.I.) of ORs were calculated using the exact method with Stata 14.2® software. These results are presented in Table 2.
The population carrier frequency of the FMR1 alleles throughout the expanded range was obtained among the whole census population of Ricaurte, separating the results among sexes and origins. Given the small number of individuals in each of the allele categories, we decided to assume a Bayesian approach, to estimate the different carrier frequencies of the FMR1 alleles: FM, premutation, and gray zone. We obtained the Bayesian point estimates and their credibility regions (C.R.), which have a different interpretation compared with confidence intervals. In this case, limits of the credibility region are the values between what is possible to find the 95% of carrier frequencies in a given population [26]. For the estimation procedure, it was assumed that the natural pattern of the number of individuals, belonging to each mutation carrier category in the population, could be modeled using a multinomial distribution (likelihood); and the prior information about the parameters (vector of the carrier frequency) could be expressed using a Dirichlet distribution (the prior distribution). We used the empirical Bayes approach to obtain the parameters of the Dirichlet distribution, which were computed using the bootstrap intervals obtained from the data of the group of participants whose blood samples were collected [27], except for non-local people (men and women) because among them we did not observe cases of FM. As prior information for non-local men we used the prevalence obtained by Coffee et al (2009) [10] and for the non-local woman, the results reported by Song et al. (2003) [12] were considered as prior information.
The estimation procedure was carried out for different groups of inhabitants of Ricaurte, according to their origin: (a) whole population of males and females, (b) native males and native females, and (c) non-native males and non-native females. The statistical analysis was carried using the interface between the Open Bugs® software and the R software® [28]. The carrier frequency of each allele is presented in Table 3.
Results
Study population
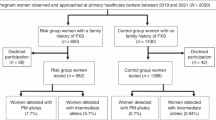
The total population of Ricaurte, registered in the census, was 1186 inhabitants (634 females and 552 males), with 75% of males and 71% of females being native of Ricaurte. There were 872 native and 314 non-native subjects in the census. Among natives, 21.8% (190 subjects) did not consent to participate in this study. Non-participation among non-natives was 22.3% (70 subjects).
Informed signed consent forms and blood spot samples were obtained from 926 (78.1%) subjects, 424 males, and 502 females. Among the collected samples, 329 and 353 were males and females’ natives of Ricaurte, respectively. The age of screened subjects ranged from 8 days to 96 years old.
Screening and confirmatory DNA tests
From the total number of 926 samples screened, 33 had the FM (11 females and 22 males), 25 carried a premutation allele (20 females and 5 males), and 27 carried a gray zone allele (22 females and 5 males). The screening results (number of individuals and frequencies) among total, natives, and non-natives, split by sex, are reported in Table 1.
Comparison with previous studies
Table 2 reports the comparison between the observed carrier frequency of each allele among the blood screened subjects of Ricaurte and the respective carrier frequency reported in Hunter et al. (2014) after adding up the overall carrier frequency of each allele (i.e. FM or premutation alleles) throughout the studies belonging to that meta-analysis [13]. The carrier frequency of each allele in the sample of Ricaurte was also compared to those reported in Tassone et al. 2012 [9], specifically for the carrier frequency of gray zone alleles. A statistically significant difference was observed for all allele categories, with exception of the gray zone among males. Furthermore, among men, the odds of carrier having an FM allele in Ricaurte was 323 times that in Hunter’s et al. study, and it was 192 times that in Hunter’s study among females. For the premutation alleles, OR were 8.8 and 7.1 among males and females, respectively.
Estimated population’s carrier frequency of expanded FMR1 allele
The carrier frequency of each expanded allele, estimated by the Bayesian methods, is presented for women and men according to their origin (natives, non-natives, and total) in Table 3. Among the whole population, the estimated carrier frequency of the FM was 48.2 per 1000 subjects among men and 20.5 per 1000 subjects among women. Full mutation and premutation carrier frequencies were higher among natives. These figures were 60.6 per 1000 subjects and 31.0 per 1000 subjects among native males and native females, respectively; being significantly higher in males compared with those non-natives. Moreover, the estimated prevalence of the premutation allele carrier was almost six times higher in native females in comparison with the non-native females, being a significant difference.
Discussion
The prevalence of FXS has varied in time and place due to changes in the methodologies, to differences in screened populations, and to variation among the definitions of the different CGG size ranges of alleles which have prevented the comparison among studies to estimate accurately the global prevalence of carrier of different FMR1 CCG repeat size alleles [13, 29].
Hunter et al. (2014) addressed these issues by carrying out a meta-analysis of the prevalence of FMR1 allele carrier using a random effects statistical model and including 54 articles, accounting for 5582 subjects. The study yielded a prevalence of the FM allele carrier as 0.14 per 1000 males (95% C.I.: 0.01–0.31 per 1000 males) and 0.09 per 1000 females (95% C.I.: 0.09–0.29 per 1000 females) [13]. The prevalence of carries of PM alleles was found in 1.17 per 1000 males (95% C.I.: 0.6–1.87 per 1000 males) and 3.44 per 1000 females (95% C.I.: 0.63–8.33 per 1000 females).
Differences in prevalence across studies can also be explained by ethnicity as observed in many studies [9, 19, 30], which have shown important differences in prevalence of gray zone alleles and premutation carriers in the same country, but in different ethnic groups. In the current study, we report on a special Colombian district with a high carrier frequency of premutation and FM alleles in both males and females, although this prevalence probably does not represent the prevalence of the whole country. However, given the observed high carrier frequency of expanded alleles, we suggest carrying out newborn screening for FXS in Colombia and especially in the Valle del Cauca, the province where Ricaurte is located.
Using Bayesian methods, the carrier frequency found in Ricaurte, of the FM was 47.6 per 1000 males (95% C.R.: 36.3–61.50) and 20.5 per 1000 females (95% C.R.: 13.5–28.6). The premutation carrier frequency was 14.1 (95% C.R.: 7.4–20.7) per 1000 males and 35.7 (95% C.R.: 26.5–46.20) per 1000 females. These are the highest carrier frequencies reported until now in the literature [13, 14, 16, 31,32,33,34].
In the present research, the screening tool was applied to all inhabitants of Ricaurte who consented (not biased against or in favor of ID); hence, the results could be compared with the prevalence estimated by Hunter et al. in the group where the total population was studied. Table 2 indicates that carrier frequencies of FXS alleles are significantly higher in Ricaurte (Colombia) in comparison with the frequencies of studies of Hunter et al. and Tassone et al. Thus, the carrier frequency of the FM allele was 343.3 times higher among Ricaurte’s males and 226.7 higher among Ricaurte’s females. Similarly, the Ricaurte´s prevalence of premutation carrier was 11.1 times higher among males and 9.4 times higher among women than the respective prevalence estimated by Hunter et al. [13].
The observed frequency of individuals with an FM is higher than that of premutation carriers likely because premutation carriers tend to leave Ricaurte looking for better life opportunities whereas many of those with an FM are affected by ID and are not able to leave. In contrast, the prevalence of individuals with a gray zone allele was similar to the prevalence reported in the literature. This finding could be explained by the fact that no case was found to have expanded from a gray zone allele to a premutation allele.
The elevated prevalence of Fragile X mutation found in Ricaurte could be explained by the combination of several factors. The limited access of the inhabitants to health services, specifically genetic counseling and molecular testing, the hereditability and phenotypic characteristics inherent to FXS as asymptomatic carriers of women with the FM, or some popular beliefs of the population as wizard may have contributed to a low interest for medical assistance by families of the affected individuals. Also, there is a local belief that environmental factors could be the cause of ID. Finally, there is a lack of knowledge about FXS among local health workers.
Ricaurte and the founder effect
Ricaurte is a small town founded in the late XVIII century by 11 families, of which the family names are known, ten of them originated from other Colombian regions and one from Spain [31]. In one of the descriptions made by Álvarez Gardeazabal in 1986 emerged that individuals with ID were members of the families that had produced affected people “for centuries and centuries” [35]. The fact that all of the FM and premutation alleles were linked to three independent pedigrees (data not published). Given the socio-demographic characteristics of the town, it is well sustained to assume that a founder effect was responsible for the elevated frequency of the expanded alleles among subjects who are natives of Ricaurte, 66.7 per 1000 males and 31.3 per 1000 females for the FM; and 15.1 per 1000 males and 52.6 per 1000 females for the premutation. However, we will evaluate this hypothesis with haplotype analysis in future studies.
Following the test results, the inhabitants of Ricaurte who were found to be carriers of a gray zone or a premutation allele, and also females with FM of the FMR1 gene, received genetic and reproductive counseling, discussing the probability of having children with an expanded FMR1 premutation or children with the FM and therefore affected by FXS. In addition, premutation carriers underwent medical evaluation with a clinical history and physical examination aimed at finding signs and symptoms of FMR1-associated disorders, including FXPOI and FXTAS. Of the 20 females with the premutation, 17 were older than 40 years and 35% had findings suggestive of FXPOI; 8 of the females with premutation were older than 50 years and 50% had symptoms and clinical signs of FXTAS; one woman presented with FXPOI and FXTAS; three sister carriers of the premutation had more severe phenotypes, one had seizures that were difficult to control, another showed severe cerebellar atrophy related with intake of phenobarbital and the last had severe lifelong mutism [36]. Of the five males with premutation, two were older than 50 years and both had clinical signs of FXTAS, one had marked distal tremor and the other presented with behavioral changes suggestive of severe frontal deficits.
Individuals affected with the premutation and FXS underwent a general medical assessment and were given specific recommendations for treatment of the pathologies encountered, such as seizures, aggression, sleep disorders, anxiety, substance use such as alcohol and drugs, among other general conditions. In eight patients with an FM, we found that alcohol and substance use dependence was associated with exacerbation of their behavioral problems, such as increased impulsivity and aggression, as well as of medical problems such as an increased frequency of seizures [32]. One case was diagnosed with Down syndrome and FXS and she was treated with sertraline for her severe anxiety and she had a good response to less anxiety and better language [33].
Castilla et al. [34] defined a genetic geographic cluster as a higher prevalence of genotypes compared to what is expected, in a population who lives in a limited geographic area for a long time. This definition differs from the definition of clusters of other types of diseases, as it does not use the prevalence of affected individuals, but of the genotypes. This is sustained by the fact that in genetic diseases there are asymptomatic individuals who are heterozygous carriers in the recessive pathologies, premutation carriers in triplet repetition diseases, and carriers without penetrance in dominant disorders, among others [34, 37].
The semi-rural district of Ricaurte meets the characteristics of a genetic cluster of FXS. First, the prevalence of both the premutation and the FM allele carrier is higher than the reported global prevalence [38,39,40]. Second, Ricaurte is a recognized Colombian district with a limited geographic area. Third, according to the observation made by the writer Álvarez Gardeazabal, the study by Universidad del Valle (Colombia) researchers in the late 1990s and the current study, FXS has been in Ricaurte for at least 60 years, but an expanded allele probably arrived with inhabitants of Ricaurte when it was founded.
Finally, the socio-demographic conditions, the genomics characteristics, and heritability of FXS suggest that Ricaurte is the FXS genetic cluster with the highest reported prevalence to date in the medical literature.
References
Hagerman RJ, Hagerman PJ. Fragile X syndrome: diagnosis. In: Hagerman RJ, Hagerman PJ, editors. Treatment and research. 3rd ed. Baltimore: The John Hopkins University Press; 2002.
Harris SW, Hessl D, Goodlin-Jones B, Ferranti J, Bacalman S, Barbato I. et al. Autism profiles of males with fragile X syndrome. MacLean WE Jr, Abbeduto L. (eds) Am J Ment Retard. 2008. p. 427–38.
Loesch DZ, Huggins RM, Bui QM, Epstein JL, Taylor AK, Hagerman RJ. Effect of the deficits of fragile X mental retardation protein on cognitive status of fragile x males and females assessed by robust pedigree analysis. J Dev Behav Pediatr. 2002;23:416–23.
Hagerman R, Hagerman P. Advances in clinical and molecular understanding of the FMR1 premutation and fragile X-associated tremor/ataxia syndrome. Lancet Neurol. 2013;12:786–98.
Saldarriaga W, Forero JV, Gonzalez LY, Hagerman R. Síndrome de temblor y ataxia asociado a frágil X (FXTAS): revisión de la literatura. Acta Neurol Colomb. 2015;31:325–34.
Wheeler AC, Bailey DB, Berry-Kravis E, Greenberg J, Losh M, Mailick M, et al. Associated features in females with an FMR1 premutation. J Neurodev Disord. 2014;6:18.
Roberts JE, Tonnsen BL, McCary LM, Ford AL, Golden RN, Bailey DB. Trajectory and predictors of depression and anxiety disorders in mothers with the FMR1 premutation. Biol Psychiatry. 2016;79:850–7.
Grigsby J, Cornish K, Hocking D, Kraan C, Olichney JM, Rivera SM, et al. The cognitive neuropsychological phenotype of carriers of the FMR1 premutation. J Neurodev Disord. 2014;6:28.
Tassone F, Iong KP, Tong T-H, Lo J, Gane LW, Berry-Kravis E, et al. FMR1 CGG allele size and prevalence ascertained through newborn screening in the United States. Genome Med. 2012;4:100.
Coffee B, Keith K, Albizua I, Malone T, Mowrey J, Sherman SL, et al. Incidence of fragile X syndrome by newborn screening for methylated FMR1 DNA. Am J Hum Genet. 2009;85:503–14.
Tassone F. Advanced technologies for the molecular diagnosis of fragile X syndrome. Expert Rev Mol Diagn. 2015;15:1465–73.
Song F, Barton P, Sleightholme V, Yao G, Fry-Smith A. Screening for fragile X syndrome: a literature review and modeling study HTA Health Technology Assessment NHS R&D HTA Programme Executive Summary Screening for fragile X syndrome. Health Technol Assess (Rockv). 2003;7:1–106.
Hunter J, Rivero-Arias O, Angelov A, Kim E, Fotheringham I, Leal J. Epidemiology of fragile X syndrome: a systematic review and meta-analysis. Am J Med Genet A. 2014;164A:1648–58.
Meguid N, Abdel-Raouf E, Dardir A, El AM. Prevalence of fragile X syndrome among school-age Egyptian males. World J Pediatr. 2007;3:271–5.
Puusepp H, Kahre T, Sibul H, Soo V, Lind I, Raukas E, et al. Prevalence of the fragile X syndrome among Estonian mentally retarded and the entire children’s population. J Child Neurol. 2008;23:1400–5.
Turner G, Webb T, Wake S, Robinson H. Prevalence of fragile X syndrome. Am J Med Genet. 1996;64:196–7.
Tzeng C-C, Tsai L-P, Hwu W-L, Lin S-J, Chao M-C, Jong Y-J, et al. Prevalence of the FMR1 mutation in Taiwan assessed by large-scale screening of newborn boys and analysis of DXS548-FRAXAC1 haplotype. Am J Med Genet A. 2005;133A:37–43.
Chow JC, Chen D-J, Lin C-N, Chiu C-Y, Huang C-B, Chiu P-C, et al. Feasibility of blood spot PCR in large-scale screening of fragile X syndrome in southern Taiwan. J Formos Med Assoc. 2003;102:12–6.
Rifé M, Badenas C, Mallolas J, Jiménez L, Cervera R, Maya A, et al. Incidence of Fragile X in 5,000 consecutive newborn males. Genet Test. 2003;7:339–43.
Saldarriaga W, Tassone F, González-Teshima LY, Forero-Forero JV, Ayala-Zapata S, Hagerman R. Fragile X syndrome. Colomb Med (Cali, Colomb). 2014;45:190–8.
Hagerman RJ, Hagerman P. Fragile X-associated tremor/ataxia syndrome—features, mechanisms, and management. Nat Rev Neurol. 2016;12:403–12.
Payan C, Saldarriaga W, Isaza C, Alzate A. Estudio focoendémico de retardo mental en Ricaurte Valle. In: XI premio Aventis—Academia Nacional de Medicina a la investigaciónmédica. 2000. p. 12–20.
Filipovic-Sadic S, Sah S, Chen L, Krosting J, Sekinger E, Zhang W, et al. A novel FMR1 PCR method for the routine detection of low abundance expanded alleles and full mutations in fragile X syndrome. Clin Chem. 2010;56:399–408.
Tassone F, Pan R, Amiri K, Taylor AK, Hagerman PJ. A rapid polymerase chain reaction-based screening method for identification of all expanded alleles of the fragile X (FMR1) gene in newborn and high-risk populations. J Mol Diagn. 2008;10:43–9.
Maddalena A, Richards CS, Mcginniss MJ, Brothman A, Desnick RJ, Grier RE, et al. Technical standards and guidelines for fragile X: the first of a series of disease-specific supplements to the standards and guidelines for clinical genetics laboratories of the American College of Medical Genetics.
Forster J, O’Hagan A. Kendalls advanced theory of statistics. 2nd ed., vol. 2B (Pb 2015) London: Willey India Exclusive; 2015.
Gelman A, Carlin JB, Stern HS, Dunson DB, Vehtari A, Rubin DB. Bayesian data analysis. 3rd ed. Chapman and Hall/CRC; 2013.
Sturtz S, Ligges U, Gelman A. R2WinBUGS: A package for running WinBUGS from R. J Stat Softw. 2005;12:1–16.
Hagerman PJ. The fragile X prevalence paradox. J Med Genet. 2008;45:498–9.
Fernandez-Carvajal I, Walichiewicz P, Xiaosen X, Pan R, Hagerman PJ, Tassone F. Screening for expanded alleles of the FMR1 gene in blood spots from newborn males in a Spanish population. J Mol Diagn. 2009;11:324–9.
Lopez-Bedoya LM, Ayala-Rodriguez GI. Levantamiento historico corregimiento de Ricaurte municipio de Bolivar. Universidad Tecnologica de Pereira; 1997.
Salcedo-Arellano MJ, Lozano R, Tassone F, Hagerman RJ, Saldarriaga W. Alcohol use dependence in fragile X syndrome. Intractable Rare Dis Res. 2016;5:207–13.
Saldarriaga W, Ruiz FA, Tassone F, Hagerman R. Down syndrome and fragile X syndrome in a Colombian woman: case report. J Appl Res Intellect Disabil. 2016;30:970–4.
Castilla EE, Schuler-Faccini L. From rumors to genetic isolates. Genet Mol Biol. 2014;37(Suppl):186–93.
Alvarez-Gardeazabal G. “El Divino”. Bogota: Plaza & Janes; 1986.
Saldarriaga W, Lein P, González Teshima LY, Isaza C, Rosa L, Polyak A, et al. Phenobarbital use and neurological problems in FMR1 premutation carriers. Neurotoxicology. 2016;53: 141–7.
Poletta FA, Orioli IM, Castilla EE. Genealogical data in population medical genetics: field guidelines. Genet Mol Biol. 2014;37(Suppl):171–85.
Crawford DC, Meadows KL, Newman JL, Taft LF, Scott E, Leslie M, et al. Prevalence of the fragile X syndrome in African-Americans. Am J Med Genet. 2002;110:226–33.
Pesso R, Berkenstadt M, Cuckle H, Gak E, Peleg L, Frydman M, et al. Screening for fragile X syndrome in women of reproductive age. Prenat Diagn. 2000;20:611–4.
O’Byrne JJ, Sweeney M, Donnelly DE, Lambert DM, Beattie ED, Gervin CM, et al. Incidence of Fragile X syndrome in Ireland. Am J Med Genet A. 2017;173:678–83.
Acknowledgements
This work was supported by UC Davis Seed Grant and by the Universidad del Valle (Colombia) grant 1771. Special thanks to Asuragen, Inc. for providing supplies for this screening study.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
RJH has received funding from Alcobra, Neuren, Novartis, Roche, and Marinus regarding treatment studies in fragile X syndrome. RJH has also consulted with Zynerba and Ovid regarding treatment studies in fragile X syndrome. FT has received funding from Asuragen, Inc.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Saldarriaga, W., Forero-Forero, J.V., González-Teshima, L.Y. et al. Genetic cluster of fragile X syndrome in a Colombian district. J Hum Genet 63, 509–516 (2018). https://doi.org/10.1038/s10038-017-0407-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s10038-017-0407-6
This article is cited by
-
Phenotypic variability to medication management: an update on fragile X syndrome
Human Genomics (2023)
