
Abstract
Background
Pre-dialysis blood pressure variability (BPV) in adolescent and young-adult maintenance hemodialysis (MHD) patients remains unknown. This study aimed to show the degree of 44-h BPV and to explore its related risk factors in adolescent and young-adult MHD patients.
Methods
One hundred and fifty-three hemodialysis patients aged from 14 to 29 were selected from 11 medical facilities in Guizhou, China. Variability independent of the mean BP (VIM) obtained by 44-h ambulatory BP monitoring was used to calculate BPV. Baseline characteristics, physical measurement, and laboratory parameters were compared between different groups categorized by quartiles of VIM of systolic BP (VIMSBP).
Results
VIMSBP levels were found to be positively related to interdialytic weigh growth rate (IDWG), serum phosphorus, and serum intact parathyroid hormone (iPTH; Spearman correlation coefficients 0.474, 0.229, and 0.437, respectively; P<0.05 for all) and negatively related to hemoglobin (Hb) and albumin (−0.317, P<0.001, and −0.166, P=0.04, respectively) in all adolescent and young-adult MHD patients. In multiple linear regression analysis, IDWG, Hb, serum phosphorus, and serum iPTH had an independent association with VIMSBP.
Conclusion
Our analysis revealed an independent association of BPV with IDWG, Hb, serum phosphorus, and serum iPTH among adolescent and young-adult patients undergoing dialysis. This observation warrants further study.
Similar content being viewed by others

Main
Chronic kidney disease (CKD) is an important public health problem worldwide, affecting 8–16% of the adult population. In China, the overall prevalence of CKD was 10.8%, and even higher in southwest (18.3%) regions compared with other regions (1). Hypertension is now considered to be an independent risk factor for end-stage renal disease (ESRD), prevalent over 56–85% of ESRD patients undergoing dialysis (2, 3). Pre-dialysis blood pressure has been shown to be strongly associated with poor prognosis of ESRD (4). Elevated pre-dialysis blood pressure represents a powerful risk marker for subsequent cardiovascular events and all-cause mortality both in children and in elder maintenance hemodialysis (MHD) patients (5, 6). Unfortunately, effective management strategies of hypertension for dialysis patients are not available (7).
Blood pressure variability (BPV), defined as blood pressure fluctuations, appeared in all hemodialysis (HD) patients. In the past, only five major studies indicated that the pre-dialysis or visit-to-visit BPV, a new marker of cardiovascular risk, was independently associated with all-cause mortality in elder MHD patients (8, 9, 10, 11, 12, 13). However, no data are available relating BPV in adolescent and young-adult patients with HD to primary end point such as cardiovascular events and all-cause mortality.
In the present study of 153 Chinese youths, we evaluated 44-h ambulatory BP (ABP) from the end of last dialysis to the beginning of the next dialysis. To our knowledge, this is the only large group of adolescent and young-adult MHD patients in which 44-h ABP levels have been collected. Multiple linear regression analysis was used to characterize the degree of BPV and to explore its related risk factors in dialysis patients aged 14–29 during dialysis interval monitored by ABP.
Methods
Subjects
The adolescent and young-adult patients aged 14–29 years who underwent routine MHD at 11 dialysis facilities in GuiZhou, Southwest China, were enrolled in this multicenter, prospective study. Inclusion criteria are as follows: (i) patients undergoing HD three times weekly, (ii) 14≤age <30 years, and (iii) antihypertensive therapy only use calcium channel blockers (CCBs) and/or angiotensin system blockers (AECI or ARB). We excluded patients who did not sign the informed consent or invalid monitoring, who underwent kidney transplantation, combined HD, and peritoneal dialysis, and who were taking other antihypertension drugs such as metoprolol or terazosin. Ethical approval for this study (GZPPHEC-2015-028) was provided by the Ethical Committee of GuiZhou Provincial People’s Hospital, China, on 2 February 2015. The informed consent was obtained from every young adults or immediate family members of adolescent subjects before the enrollment.
Measurement of Ambulatory Blood Pressure Monitoring and Assessment of BPV
ABP monitoring was performed once for each subject using validated devices (Spacelabs, WA) according to the instructions from the end of last dialysis to the beginning of the next dialysis, totally 44 h (ref. 14). The intervals between measurements were 30 min during the day (0800–1000 hours) and 60 min at night (1000–0800 hours). In 44 h, there should be in total 68 times blood pressure monitoring, which when more than 80% (54 times) was considered as an effective monitoring. The patients were asked to keep a detailed diary during the monitoring to identify the false-positive result of hypertension. According to the 44-h AMBP monitoring reports, the 44-h mean SBP and DBP were calculated.
In order to transform SD uncorrelated with the mean BP, variability-independent of the mean (VIM) was calculated as follows (15):


-
1
The parameter a can be estimated using nonlinear regression by fitting a curve of the form y=xa through a plot of individual SD SBP (y) against the individual mean SBP (x).
-
2
The parameter k is a constant that can be chosen such that the mean value of VIM is the same as the mean value of SD.
-
3
The parameter M is the average value of the mean SBP in all individuals, and then k=Ma.
For example, the parameter a (nonlinear regressing fitting power function was used to estimate) was 0.465 and the average value of the mean SBP in all individuals was 136.87 mm Hg, and then k=Ma=136.870.465=9.85; if the mean SBP±SD SBP of Patient 1 was 143±15 mm Hg, then VIM(Patient 1)=9.85 × 15/1430.465=14.70. Therefore, a=0.465, k=9.85 for 44-h mean SBP. Same calculation was performed for 44-h mean DBP (a=0.239, k=2.88) in our research.
Physical Measurement and Laboratory Parameters
To evaluate nourishment status in the subjects, we assessed their height (cm) and weight (kg) and calculated BMI as weight/height2 (kg/m2). Upper arm muscle circumference was measured with soft feet. The measuring point was the midpoint from shoulder to the olecranon connection when upper limbs naturally droop. To minimize intra-operator variability, the averages of three consecutive measurements were recorded. Dry weight was obtained from bioelectric impedance device directly (Biodynamics, Seattle, WA) using Bioelectrical impedance spectroscopy, and the interdialytic weigh growth rate (IDWG%) was calculated by the following formula: IDWG%=(body mass at the beginning of the dialysis−body mass at the end of last dialysis)/dry weight.
Blood samples were also obtained in the morning after an 8-h overnight fast. Laboratory parameters include the following: pre-dialysis serum creatinine, blood urea nitrogen, Cystatin C, hemoglobin (Hb), albumin (Alb), high-sensitivity C-reactive protein, serum calcium, phosphorus, magnesium, and intact parathyroid hormone (iPTH). Biochemical indicators were tested using automatic biochemical detector (Olympus, Tokyo, Japan) and Hb was determined using blood routine examination (Sysmex sf-3000, Kobe, Japan). iPTH assay was detected using chemiluminescence immunoassay. Hb (36 subjects) and renal function parameters (48 subjects) were measured more than two times in 3 months, and the time-average value of above parameters was calculated for analysis.
Standard HD Sessions
All patients were dialyzed using 1.6 m2 surface area high-flux polysulfone dialyzers with bicarbonate-based dialysate (Na+ 138 mmol/l, HCO3– 32 mmol/l, K+ 2.0 mmol/l, Ca2+ 1.50 mmol/l, and Mg2+ 0.5 mmol/l). The prescribed duration time was 4 h with a blood flow rate of 250 ml/min and a dialysate flow rate of 500 ml/min. The adequacy of dialysis was assessed by using Kt/V (K, dialyzer clearance of urea, t, dialysis time, V, volume of distribution of urea). According to Kidney Disease Outcomes Quality Initiative (KDOQI) 2015 update, the target Kt/V should be 1.2 per session (16).
Statistical Analysis
SPSS software (IBM, Chicago, IL) was used for statistical analyses. Means±SD and median with interquartile range were used for normally and non-normally descriptive statistics of continuous variables, respectively. Because the cutoff value of BPV was still unclear, subjects were categorized into quartiles according to the VIMSBP (VIM of 44-h mean SBP) value. Comparisons among the groups were carried out by Kruskal–Wallis test or one-way ANOVA. Simple correlation coefficient of VIMSBP and other variables were investigated by Spearman analysis. In univariate and multivariate linear regression analyses, VIMSBP was modeled as the independent variable and dialysis parameters, such as IDWG, Alb, phosphorus, iPTH, and Hb, were the dependent variables; in addition, adjustment factors included age, sex, dialysis duration, BMI, arm muscle circumference, dry weight, serum creatinine, blood urea nitrogen, Cystatin C, high-sensitivity C-reactive protein, serum calcium, serum magnesium, Kt/V, 44-h mean SBP, and drugs (ACEI/ARB, CCB). Throughout the study, P<0.05 was taken as the minimum level of statistical significance.
Results
Characteristics and Laboratory Parameters
In total, 398 patients, aged 14–29, who underwent hemodialysis were enrolled from 11 dialysis facilities (n=1,057) of Guizhou in Southwest China. Figure 1 showed that 245 subjects were excluded because they did not sign the informed consent (146 subjects), because of invalid monitoring (27 subjects), because of using other antihypertensive drugs (38 subjects), and because they underwent irregular or combined HD and peritoneal dialysis (28 subjects) and kidney transplantation (6 subjects). Among the 153 subjects attending this study, 84 cases (54.9%) were male and 69 were female (45.1%), aged 21.78±3.44 years, and the duration of dialysis that they underwent was 42.33±9.0 months. Primary diseases were as follows: chronic glomerulonephritis (71 cases, 46.41%), hypertension nephropathy (49 cases, 32.03%), congenital obstructive nephropathy (12 cases, 7.84%), polycystic kidney (8 cases, 5.23%), diabetic kidney disease (8 cases, 5.23%), and renal dysplasia (5 cases, 3.27%).

Patients enrolled in the study. HD, hemodialysis; PD, peritoneal dialysis.
Demographic, clinical, and biological characteristics of patients categorized by VIMSBP quartiles (<9.70, 9.70–11.02, 11.02–12.46, and >12.46) are shown in Table 1. Patients in the fourth quartile had higher IDWG (from the first quartile to the fourth quartile: 4.30±1.48, 5.20±1.70, 6.00±2.22, and 7.25±2.78%, P<0.001), serum phosphorus (1.50±0.48, 1.66±0.53, 1.70±0.50, and 1.86±0.69 mmol/l, P=0.04), and serum iPTH (196.40 (128.93, 385.28), 275.93 (195.10, 491.40), 426.45 (263.40, 705.70), and 510.10 (385.50, 645.65) pg/ml, P<0.001) levels, but lower Hb (119.08±23.99, 113.06±21.23, 104.49±23.37, and 98.57±22.17 g/l, P=0.001) and Alb (35.21±7.65, 35.82±5.13, 31.63±6.01, and 33.84±5.78 g/l, P=0.02) values. The remaining parameters had no statistical significance between groups (P>0.05).
The degree of 44-h mean BP and corresponding VIM, SD was presented in Table 2. The mean SBP and DBP in the 44-h period were similar between the four groups (P=0.18 and P=0.11, respectively). Variability independent of the mean SBP and VIMDBP in the 44-h period, as well as SD of SBP and SD of DBP values in the study population, was significantly higher in the fourth quartile compared with that in the first quartile (P<0.001).
Simple Correlation Coefficient of VIMSBP and Other Variables in Adolescent and Young-Adult MHD Patients
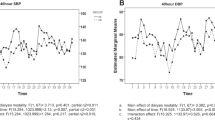
Next, the association of VIMSBP with laboratory parameters and SD of SBP was evaluated in Table 3 and Figure 2; simple correlation analysis indicated that the VIMSBP level was positively related with IDWG (Spearman correlation coefficients r=0.474, P<0.001, Figure 2a), serum phosphorus (r=0.229, P=0.004, Figure 2b), and serum iPTH (r=0.437, P<0.001, Figure 2c), and was negatively related with Hb (r=−0.317, P<0.001, Figure 2d) and Alb (r=−0.166, P=0.04) in all adolescent and young-adult MHD patients. When these associations in non-hypertensive patients (n=104) were assessed, the relationship of VIMSBP with those factors remains the same together with age and duration of dialysis; data were displayed in the Table 3. VIMSBP in hypertensive patients was associated with IDWG (r=0.555, P<0.001), serum iPTH (r=0.362, P=0.01), Hb (r=−0.290, P=0.04), and age (r=−0.300, P=0.04). In addition, there was no relationship between SBP and VIMSBP in any patient (r=0.013, P=0.88).

Correlation analysis between variability independent of systolic BP (VIMSBP) and interdialytic weigh growth rate (IDWG; a), serum phosphorus (b), serum intact parathyroid hormone (c), and hemoglobin (d).
Multivariate Linear Regression Analysis for VIMSBP
To further investigate the independent correlation of VIMSBP in all adolescent and young-adult individuals, multiple linear regression models were constructed using a model adjusted for age, sex, dialysis duration, BMI, arm muscle circumference, dry weight, laboratory parameters, Kt/V, 44-h mean SBP, and drugs (ACEI/ARB, CCB). It revealed that IDWG, Hb, phosphorus, and serum iPTH (standardized β=0.290, −0.498, 0.454, and 0.144, respectively, P<0.05) values maintained independent-factor association with VIMSBP in adolescent and young-adult MHD patients (Table 4).
Discussion
Hypertension has been considered as the major risk factor of cardiovascular disease as well as the main cause of mortality in pediatric patients with CKD (17). Considerable lines of evidence have supported the notion that increased BPV might be an independent pathogenic factor of all-cause mortality and cardiovascular event (9, 18). Findings of our study indicated that VIMSBP is significantly correlated with IDWG, phosphorus, serum iPTH, and Hb in adolescent and young-adult MHD patients. Such results suggested that BPV calculated by VIM may be directly or indirectly influenced via fluid overload, excessive activation of rein–angiotensin–aldosterone system and CKD mineral and bone disorder. These findings may shed new lights on the understanding of the importance of BPV in adolescent and young-adult dialysis patients together with (9, 18).
Inadequate volume control and salt restriction are common in dialysis patients during adolescence because of the second peak of growth and development. It may result in higher interdialytic weight gain during non-dialysis days (19). As we know, this interdialytic weight gain may be divided into weight gain from linear and somatic growth and excess fluid induced by kidney failure, with the latter contribute more. More importantly, interdialytic weight gain is the quantitative index of fluid overload that reflects the increase of BPV. As the variation of interdialytic weight gain increases, the patient’s pre-dialysis BP will increase and the blood volume after dialysis will reduce, which in turn might excessively activate rein–angiotensin–aldosterone system because of the decreased renal perfusion. In addition, numerous studies have proposed that high-salt intake will reduce baroreceptor sensitivity; meanwhile, it will also affect BPV (2, 20). Lower Hb and Alb levels in the higher VIMSBP group demonstrate that poor nutritional status during adolescence may be responsible for the increased heart rate and BP fluctuations (21). Specifically, our study is partially in agreement with findings by recent study in adult MHD patients, which show that higher IDWG and lower Hb levels are the major factors affecting high BPV patients (22).
CKD mineral and bone disorder is common in pediatric CKD patients, which has a major role in the etiology and progression of cardiovascular disease. Our study found that serum phosphorus and iPTH were positively correlated with VIMSBP. Moreover, growing lines of evidence from the recent studies have illustrated that elevated phosphate can promote vascular calcification, endothelia dysfunction, and arterial stiffness (23, 24, 25, 26). As is suggested by data analysis from the National Health and Nutrition Examination Survey (NHANES) cohort, serum iPTH levels were significantly positively correlated with both SBP and DBP (27). BP reduction in the hypertensive patients after parathyroidectomy has further expounded an etiological role of PTH in high BP, which is achieved through interaction between PTH and rein–angiotensin–aldosterone system (28, 29, 30). However, no studies on the relationship of BPV with serum phosphorus and PTH are available at present. Thus, the current study may be the first to explore the association between bone mineral metabolic disorder and BPV in CKD.
Moreover, evidence has indicated that a higher proportion of hypertension cases are diagnosed with the help of 44-h ABPM compared with 24-h ABPM, which has supported the mechanism by which volume shifts contribute to higher VIMSBP (14, 31). Latest research from Haskin et al. also analyzed 13 pediatric MHD patients aged 10−18 years using 44-h ABPM. The results suggested markedly higher BP loads on the second non-dialysis day than those on the first day, demonstrating that fluid that accumulates during the interdialytic period is related to higher BP values (32). Only the mean BP levels and loads are compared in previous literatures via 44-h ABPM. In comparison, our study is the first to apply VIMSBP, an accurate indicator, reflecting BP fluctuations instead of BP, in analyzing the larger sample size of adolescent and young-adult HD patients between dialysis day and non-dialysis days.
Nonetheless, our study is inevitably associated with certain limitations. First, considering the effect of antihypertensive drugs on the BPV level, it is explicitly stipulated that subjects receiving CCBs and (or) ACEI/ARB only for the treatment were enrolled in this study. Notably, there was no statistically significant difference in using antihypertensive drugs between different quartiles of VIMSBP groups (Table 1). Second, it is a cross-sectional study, which can hardly draw a conclusion regarding VIMSBP and abnormal mineral and bone metabolism parameters through causal relationships. In addition, the mechanisms underlying such an association remain unclear. Third, there are several measurements of BP fluctuations deriving from ABPM data, such as coefficient of variation, and weight SD, but VIM is the only indicator of BPV analyzed in this study. BPV is calculated by VIM to eliminate the influence of the mean BP on the SD of BP. As can be figured out from Table 2, SBP is not correlated with VIMSBP (r=0.013, P=0.88) (15). Finally, the variability of diurnal and nocturnal BP should be further explored, so as to provide a more detailed picture of BPV in adolescent and young-adult patients undergoing dialysis.
In conclusion, this is the first study to reveal the independent correlation of BPV with IDWG, hemoglobin, serum phosphorus, and serum iPTH among adolescent and young-adult patients undergoing dialysis. It highlights that early recognition and intervention against factors involved in hypertension is crucial to improve the outcomes of patients at risk. Furthermore, placebo-controlled randomized trials of medication targeting BPV are needed to evaluate whether these interventions can improve the renal outcomes and reduce mortality in adolescent and young-adult MHD patients.
References
Zhang L, Wang F, Wang L et al. Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet 2012;379:815–22.
Agarwal R . Regulation of circadian blood pressure: from mice to astronauts. Curr Opin Nephrol Hypertens 2010;19:51–8.
Lin J, Ding XQ, Lin P et al. A multi-center survey of hypertension and its treatment in patients with maintenance hemodialysis in Shanghai (Chinese). Zhonghua Nei Ke Za Zhi 2010;49:563–7.
Inrig JK . Peri-dialytic hypertension and hypotension: another U-shaped BP-outcome association. Kidney Int 2013;84:641–4.
Van Buren PN, Kim C, Toto RD, Inrig JK . The prevalence of persistent intradialytic hypertension in a hemodialysis population with extended follow-up. Int J Artif Organs 2012;35:1031–8.
Inrig JK, Van Buren P, Kim C, Vongpatanasin W, Povsic TJ, Toto RD . Intradialytic hypertension and its association with endothelial cell dysfunction. Clin J Am Soc Nephrol 2011;6:2016–24.
Campese VM, Lakdawala R . The challenges of blood pressure control in dialysis patients. Recent Adv Cardiovasc Drug Discov 2015;10:34–59.
Selvarajah V, Pasea L, Ojha S, Wilkinson IB, Tomlinson LA . Pre-dialysis systolic blood pressure-variability is independently associated with all-cause mortality in incident haemodialysis patients. PLoS One 2014;9:e86514.
Di Iorio B, Di Micco L, Torraca S et al. Variability of blood pressure in dialysis patients: a new marker of cardiovascular risk. J Nephrol 2013;26:173–82.
Shafi T, Sozio SM, Bandeen-Roche KJ et al. Predialysis systolic BP variability and outcomes in hemodialysis patients. J Am Soc Nephrol 2014;25:799–809.
Chang TI, Flythe JE, Brunelli SM et al. Visit-to-visit systolic blood pressure variability and outcomes in hemodialysis. J Hum Hypertens 2014;28:18–24.
Flythe JE, Inrig JK, Shafi T et al. Association of intradialytic blood pressure variability with increased all-cause and cardiovascular mortality in patients treated with long-term hemodialysis. AJKD 2013;61:966–74.
Kuipers J, Usvyat LA, Oosterhuis JK et al. Variability of predialytic, intradialytic, and postdialytic blood pressures in the course of a week: a study of Dutch and US maintenance hemodialysis patients. AJKD 2013;62:779–88.
Elaine U, Bruce A, Joseph F et al. Ambulatory blood pressure monitoring in children and adolescents: recommendations for standard assessment. Hypertension 2008;52:433–51.
Rothwell PM, Howard SC, Dolan E et al. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet 2010;375:895–905.
National Kidney Foundation. KDOQI clinical practice guideline for hemodialysis adequacy: 2015 update. Am J Kidney Dis 2015;66:884–930.
Mak RH, Bakris G . Pediatrics: masked hypertension: a risk factor in children with CKD. Nat Rev Nephrol 2010;6:132–4.
Parati G, Ochoa JE, Lombardi C, Bilo G . Blood pressure variability: assessment, predictive value, and potential as a therapeutic target. Curr Hypertens Rep 2015;17:537.
Deter HC, Buchholz K, Schorr U, Mathiak K, Sharma AM . Salt-sensitivity and other predictors of stress-related cardiovascular reactivity in healthy young males. Clin Exp Hypertens 2001;23:213–25.
Simmonds SS, Lay J, Stocker SD . Dietary salt intake exaggerates sympathetic reflexes and increases blood pressure variability in normotensive rats. Hypertension 2014;64:583–9.
Cherkas A, Abrahamovych O, Golota S et al. The correlations of glycated hemoglobin and carbohydrate metabolism parameters with heart rate variability in apparently healthy sedentary young male subjects. Redox Biol 2015;5:301–7.
Gu LJ, Zhang YR, Yuan WJ et al. Related factors and prognostic significance of intradialytic blood pressure variability in patients on maintenance hemodialysis(Chinese). Zhonghua Nei Ke Za Zhi 2013;52:453–8.
Garcia de Tena J, Hernandez-Gutierrez C, Abejon-Lopez L . Blood pressure and serum parathyroid hormone level. JAMA Intern Med 2015;175:1069.
Seifert ME, de las Fuentes L, Rothstein M et al. Effects of phosphate binder therapy on vascular stiffness in early-stage chronic kidney disease. Am J Nephrol 2013;38:158–67.
Brown JM, Williams JS, Luther JM et al. Human interventions to characterize novel relationships between the renin-angiotensin-aldosterone system and parathyroid hormone. Hypertension 2014;63:273–80.
Vaidya A, Brown JM, Williams JS . The renin-angiotensin-aldosterone system and calcium-regulatory hormones. J Hum Hypertens 2015;29:515–21.
He JL, Scragg RK . Vitamin D, parathyroid hormone, and blood pressure in the National Health and Nutrition Examination Surveys. Am J Hypertens 2011;24:911–7.
Iwata S, Hyodo E, Yanagi S et al. Parathyroid hormone and systolic blood pressure accelerate the progression of aortic valve stenosis in chronic hemodialysis patients. Int J Cardiol 2013;163:256–9.
Ulu SM, Ulasli A, Yaman F, Yaman G, Ozkececi G, Yuksel S . The relationship between vitamin D and PTH levels and cardiovascular risk in the elderly hypertensives. Clin Exp Hypertens 2014;36:52–7.
Tomaschitz A, Ritz E, Pieske B et al. Aldosterone and parathyroid hormone interactions as mediators of metabolic and cardiovascular disease. Metabolism 2014;63:20–31.
Agarwal R, Flynn J, Pogue V, Rahman M, Reisin E, Weir MR . Assessment and management of hypertension in patients on dialysis. J Am Soc Nephrol 2014;25:1630–46.
Haskin O, Wong CJ, McCabe L, Begin B, Sutherland SM, Chaudhuri A . 44-h ambulatory blood pressure monitoring: revealing the true burden of hypertension in pediatric hemodialysis patients. Pediatr Nephrol 2015;30:653–60.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Statement of Financial Support
The technological innovation team of diagnosis and treatment of CKD ((2013) 4031) and (LG (2012) 060) from the Guizhou Provincial Science and Technology Committee; ZKHT ((20161001)38) from Guiyang City Science and Technology Planning Project.
Rights and permissions
About this article

Cite this article
Da, J., Zhang, Z., Shen, Y. et al. Blood pressure variability is independent of systolic pressure in adolescent and young adult patients undergoing hemodialysis. Pediatr Res 83, 615–621 (2018). https://doi.org/10.1038/pr.2017.293
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2017.293
This article is cited by
-
Effects of indoor temperature and its fluctuation on blood pressure and its variability
International Journal of Biometeorology (2023)
