
Abstract
Background:
The aim of our study was to measure drug-related changes in hemodynamics and oxygen metabolism in response to different doses of an age-appropriate dobutamine formulation in hypoxic pigs. A secondary aim was to validate superior vena cava flow (SVCF) as a marker of cardiac index (CI) for subsequent clinical trials of this formulation in humans.
Methods:
Newborn pigs (n = 18) were exposed to 2-h hypoxia (10–15% oxygen) followed by reoxygenation (21–30% oxygen 4 h). After 1-h reoxygenation, pigs were randomized to: control group (no treatment), dobutamine infusion at a rate of 10–15 or 15–20 µg/kg/min. Dobutamine groups received two dobutamine doses during 30 min with a 60 min washout period between doses. Cardiovascular profile and oxygen metabolism were monitored. In four animals, an ultrasonic perivascular flow probe was placed around superior vena cava to measure SVCF.
Results:
Hypoxia significantly decreased CI, systemic vascular resistance and mean arterial blood pressure (MABP). Dobutamine doses significantly increased heart-rate, CI, and oxygen-delivery without changes in stroke-volume and MABP. Only 10–15 µg/kg/min increased oxygen consumption and peripheral tissue oxygenation measured by Near-infrared spectroscopy. A positive correlation was observed between SVCF and CI.
Conclusion:
The new pediatric dobutamine formulation improved hemodynamic status, with dose-specific differences in metabolic response. SVCF may be a useful surrogate for CI in subsequent clinical trials.
Similar content being viewed by others
Main
Neonatal asphyxia frequently leads to shock, myocardial dysfunction, pulmonary hypertension, poor regional perfusion, inadequate tissue oxygen delivery, impaired cerebral blood flow autoregulation, and, potentially, end-organ injury and death (1). Importantly, in neonates surviving asphyxia, there is a risk of subsequent neurological injury.
Inotropes are often used in asphyxiated infants who are exhibiting signs of cardiovascular compromise. Dobutamine, dopamine, and epinephrine are commonly used inotropes. However, these drugs are currently used off label with there being little in the way of safety or efficacy data for their use in neonates. Specifically, dobutamine, a semisynthetic sympathomimetic drug, has been used off-label in newborns and children for over 20 y to enhance cardiac output (2). The importance of using licensed age-appropriate drug formulations is now recognized by regulatory agencies, clinicians, and investigators (3).
In the light of the EU and United States new drug regulations on medicines for children, a need exists for an age-appropriate formulation for dobutamine. Much of our current understanding of the pathophysiology of perinatal disorders has evolved from animal studies. The piglet model can be used to study perinatal hypoxia: the newborn piglet has a development similar to the 36–38 wk human fetus (4). Moreover, they share with human similar anatomic and physiologic characteristics involving the cardiovascular (with a histological appearance of the myocardium nearly identical) and other systems. These characteristics confer major advantages over models in other species; moreover, its size allows the instrumentation and monitoring systemic and regional hemodynamic changes, tissue perfusion, and oxygen demand. Our animal experiments were part of a larger NEO-CIRC European project (FP7_HEALTH grant agreement 282533) which studies a new age appropriate (for use in newborns in the first 72 h of life) dobutamine formulation in order to increase availability of medicines authorized for children as well as to increase the information available on the use of medicinal products in the pediatric population.
A key factor to obtain safety and efficacy data from clinical trials of inotropes such as dobutamine is an objective measure of cardiac output (CO), and hence cardiac index (CI, calculated as CO divided by animal weight). CO is linked to systemic blood flow (and hence tissue perfusion), but the presence of ductal and atrial shunts in some neonates limits the usefulness of this approach and so newer ways of measuring systemic blood flow are needed (5). Echocardiographic measurements of superior vena cava blood flow (SVCF) may provide a more reliable indication of neonatal systemic perfusion and could be used primarily in premature neonates to assess CO independent of the transitional circulation shunts. SVCF is potentially a proxy measure for cerebral blood flow (6), and low SVCF has been associated with neurological injury in premature neonates.
The primary aim of the study was to measure the effects of different doses of a new pediatric formulation of dobutamine on hemodynamic and oxygen metabolism in hypoxic neonatal piglets. Our secondary aim was to validate SVCF as a marker of CI in neonatal asphyxiated piglets with normal and low CO. Furthermore, we evaluated changes in biochemical parameters and cardiac histological samples after dobutamine administration.
Methods
We obtained 18 newborn piglets (age 2–4 d, 1.7 ± 0.2 kg) of both sexes from a local farm on the morning of the experiment. This study was carried out in strict accordance with the recommendations in the Guide for the Care and Use of Laboratory Animals. The experimental protocol met European and Spanish regulations for protection of experimental animals (2010/63/UE and RD53/2013) and was approved by the Ethical Committee for Animal Welfare of the Cruces University Hospital, Spain (EU-03.BI#013_11).
Surgical Preparation
The animals were sedated with intramuscular ketamine (15 mg/kg) and diazepam (2 mg/kg). Analgesia and anesthesia were induced by intravenous (IV) fentanyl (5 μg/kg) and propofol (1.2 mg/kg) respectively and maintained by a continuous infusion of fentanyl (5–20 μg/kg/h) and propofol (2–3 mg/kg/h) administered through an ear vein. At the same time, the animals were paralyzed using a continuous IV infusion of vecuronium bromide (3 mg/kg/h). A continuous three-lead ECG was established in all animals.
After a tracheotomy, we inserted a 4.0 mm ID tracheal tube, connected to a neonatal ventilator (VIP Bird, Bird Products, Palm Springs, CA) with the following initial settings: fraction of inspired oxygen (FiO2) = 0.25, respiratory frequency (fR) = 20 breaths/minute, positive end-expiratory pressure = 3 cmH2O and positive inspiratory pressure = 10 cmH2O. Deviations from acceptable blood gases values (PaO2 90–110 mmHg, PaCO2 35–45 mmHg and pH 7.35–7.45) were corrected by adjusting the ventilator settings and/or by adding sodium bicarbonate as needed.
A thermodilution arterial catheter (5Fr, PiCCO Plus, Pulsion, München, Germany) was inserted into the femoral artery to monitor mean arterial blood pressure (MABP) and heart rate (HR), to measure CO and to obtain arterial blood samples for blood gas analysis (PaO2, PaCO2, pH, Base Excess (BE), SaO2), lactate, and hemoglobin (Hb) (GEM Premier 4000, Instrumentation Laboratory Company, Lexington, MA). In addition, a 5 Fr three-lumen catheter was inserted into the internal jugular vein to inject cold saline, to monitor central venous pressure (CVP), to maintain fluids (10% dextrose-saline at 5 ml/kg/h) and to obtain blood samples for blood gas analysis and for biochemical analysis. Finally, a 5 Fr three-lumen catheter was inserted into the femoral vein for IV infusion of dobutamine with an infusion pump (Alaris System with Guardarails, Cardinal Health, San Diego, CA). Blood temperature, measured by a thermistor at the thermodilution arterial catheter tip, was maintained at 38–39 °C using an overhead warmer along the experiment.
Correlation Studies of SVCF vs. CI
To measure SVCF, a left anterior thoracotomy was performed in the first intercostal space in four animals. The superior venous cava was isolated and a noninvasive perivascular Doppler flow probe (MA3PS, Transonics, Ithaca, FL) was placed around it to continuously measure SVCF. SVCF values were compared to the CI measured by thermodilution at different time points during experimental procedure (baseline, hypoxia, reoxygenation, and dobutamine administration). Briefly, 3 ml of cold saline (<8 °C) was injected into the central venous catheter. The injectate rapidly disperses volumetrically and thermally within the pulmonary and cardiac volumes. This volume of distribution is termed the intrathoracic volume. When the thermal signal reaches the thermistor-tipped in the femoral catheter, a temperature difference is detected and a dissipation curve is generated. Then, the monitor use specific algorithms to determine the cardiac output by integrating the area under the curve of the arterial pressure vs. time trace.
Experimental Design
Following surgery, the piglets were allowed to stabilize until baseline hemodynamic measures were stable (changes less than 10% over a 30-min period). Preliminary arterial blood gas analysis was performed at this time to ensure that pH, PaO2, and PaCO2 values were within acceptable limits. After stabilization, hypoxia was induced (FiO2: 0.1–0.15) by increasing the concentration of inhaled nitrogen gas for 120 min (7). At that moment, animals were randomly assigned to:
-
1. Control group (n = 6): following 60 min of reoxygenation (FiO2: 0.21–0.30) animals were maintained without dobutamine treatment after the end of the experimental period;
-
2. Low- to medium-dose group (L-M group) (n = 6): after 60 min of reoxygenation (FiO2: 0.21–0.30), each animal received two doses of the new pediatric dobutamine formulation (Proveca LTD, Daresbury, Cheshire, UK) during 30 min (10 and 15 µg/kg/min) with 60 min washout period between doses and after discontinuation of medication. All infusions were administered with an infusion pump, and
-
3. Medium- to high-dose group (M-H group) (n = 6): after 60 min of reoxygenation (FiO2: 0.21–0.30), each animal received two doses of the new pediatric dobutamine formulation during 30 min (15 and 20 µg/kg/min) with 60 min washout period between doses and after discontinuation of medication. The experimental design is shown in Figure 1 .
Figure 1 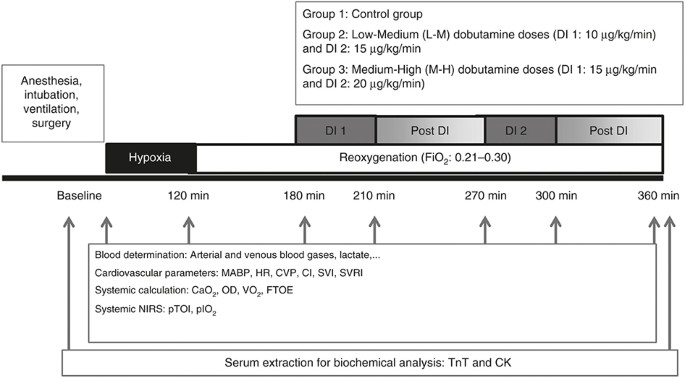
Experimental protocol. The arrows represents the points at which the data were recorded. CaO2, arterial oxygen content; CI, cardiac index; CVP, central venous pressure; CK, creatine kinase; DI, dobutamine infusion; FiO2, fraction of inspired oxygen; FTOE, systemic fractional oxygen extraction; HR, heart rate; MABP, mean arterial blood pressure; OD, oxygen delivery; pIO2, peripheral intravascular oxygenation; pTOI, peripheral tissue oxygenation index; SVI, stroke volume index; SVRI, systemic vascular resistance index; TnT, troponin T; VO2, oxygen consumption.

Dobutamine Formulation
The new pediatric formulation of dobutamine HCl solution (12.5 mg/ml in 5 ml glass vials, Proveca LTD, Daresbury) for injection is novel and investigational, containing half the quantity of antioxidant (sodium metabisulfite) compared to other marketed formulations due to concerns over the toxicity of this preservative in neonates. The manufacturing process is also novel, and uses nitrogen infusion and blanketing to limit the oxygen content the headspace of the vial, thereby limiting the rate of degradation of the dobutamine.
Measurements
At different time points ( Figure 1 ), blood samples were drawn from the femoral artery and the jugular vein to obtain blood samples to measure blood gases, base excess, lactate, and to perform biochemical analysis.
Animals were monitored for MABP, HR, CO, stroke volume index, CVP and temperature (IntelliVue MP50, Phillips, The Netherlands) specifically before and after any intervention ( Figure 1 ). The following variables were calculated:
-
1. Cardiac index (CI) (ml/kg/min) = CO ÷ weight
-
2. Systemic vascular resistance index (SVRI) (mmHg/ml.kg−1.min−1) = (MABP-CVP) ÷ CI
-
3. Systemic arterial (venous) oxygen content (Ca(v)O2) (O2 ml/dl) = (Sa(v)O2 × Hb × 1.39/100) + (Pa(v)O2 × 0.003)
-
4. Systemic oxygen delivery (OD) (O2 ml/kg/min) = CaO2 × CI
-
5. Systemic oxygen consumption (VO2) (O2 ml/kg/min) = (CaO2 – CvO2) × CI
-
6. Systemic fractional oxygen extraction (FTOE) = (SaO2 – SvO2) ÷ SaO2
Change in peripheral perfusion-oxygenation was assessed using a commercial continuous-wave method with a near-infrared spatially resolved spectroscopy (NIRS) instrument (NIRO 200 Hamamatsu Photonics, Hamamatsu, Japan). Laser diodes produce light in the near-infrared range that is transmitted thorough a fibreoptic bundle. The relative absorption coefficients obtained are used to calculate the tissue oxygenation index (TOI) in percent, that is, the ratio of oxyhemoglobin (O2Hb) to total hemoglobin (tHb), total hemoglobin being calculated as the sum of O2Hb and deoxyhemoglobin (HHb). pIO2 and pTOI were continuously monitored. Changes in pIO2, equivalent to the difference between O2Hb and HHb, were used as a surrogate of changes in peripheral blood flow whereas pTOI was used to estimate venous oxygen saturation (pSvO2) (8). Due to the small size and the thin covering layers of tissue of term, the sensor was placed in the renal region (renal fossa) in order to evaluate changes in peripheral perfusion and oxygenation.
Biochemical and Histological Analysis
Serum troponin T (TnT) and serum creatinine kinase activity (CK) were determined at baseline and at the end of the experiment using specific Troponin T Elisa Kit (KA3319, Abnova, Tapei City, Taiwan) and creatinine kinase assay kit (ab155901, Abcam, Cambridge, MA).
At the end of the experiment, animals were sacrificed through an overdose of anaesthesia (6% of sevoflurane, 1.5 mg/kg of vecuronium and 300 mg/kg of potassium chloride). Postmortem samples of left ventricle and left atrium were removed and fixed in 4% formaldehyde for histological analysis. Different areas of the heart were embedded in paraffin wax to prepare sections for light microscopy and stained for routine histological examination (hematoxylin-eosin). The histological examinations were carried out by a pathologist who was blinded to group assignments of these piglets.
Statistical Analysis
Data was analyzed using JMP statistical discovery software (version 8, SAS Institute, North Carolina). One-way ANOVA was performed to assess time point differences in gas exchange, cardiovascular parameters and systemic oxygenation and perfusion as a function of group. Comparisons of results at all-time points were performed by two-way repeated-measures ANOVA as a function of group and time. Comparison of measured values before and after dobutamine administration was assessed by Student’s paired t test. Simple linear correlation analysis was used to assess the relationship between SVCF measurements and CI measurements. A P < 0.05 was considered statistically significant. Values are expressed as mean ± SD.
Results
The subsequent results are displayed as mean and SD. The piglets were 2.0 ± 0.9 d old, weighing 1.7 ± 0.2 kg with no statistically significant differences noted in any of the baseline values between each group. Three piglets died during hypoxia and their data were excluded from the study.
Two hours of hypoxia resulted in severe metabolic acidosis (pH: 6.81–6.96; base excess (BE): −24.9–22.2 mmol/l) with a significant increase in lactate concentration (16.5–18.1 mmol/l) and normocapnia (41–44 mmHg) ( Table 1 ). With the first dose of dobutamine (10 μg/kg/min in low to medium (L-M) group and 15 μg/kg/min in medium to high (M-H) group) pH, BE, and lactate concentration demonstrated a significant improvement compared to control group ( Table 1 ). These findings were also replicated after second dobutamine dose in both dobutamine groups ( Table 1 ).
SVCF vs. CI Correlation
Thirty-two correlations were calculated between SVCF with CI in four animals. A good positive correlation (r2 = 0.645) was observed when SVCF was compared with CI (P < 0.0001) ( Figure 2 ). At baseline, the animals showed a SVCF of 75 ± 17 ml/kg/min that decreased to 45 ± 1 ml/kg/min during hypoxia.

Correlation between superior vena cava flow (SVCF) and cardiac index (CI). The regression line and correlation coefficient (r2 = 0.645) demonstrate a significant linear relationship (P < 0.0001).
Systemic Hemodynamic Responses
There were no baseline differences among groups in the cardiovascular parameters studied ( Figures 3 and 4 ). Two hours of hypoxia resulted in a significant decrease in both CI (mean CI: 228–242 vs. 327–425 ml/kg/min) and systemic vascular resistance index (SVRI) (mean SVRI: 0.10–0.14 vs. 0.19–0.24 mmHg/kg/min) and severe reduction in MABP (mean MABP: 32–34 vs. 75–89 mmHg) in comparison with baseline values (P < 0.05 in all cases), but no significant changes in stroke volume index or HR.

The effect of dobutamine infusion in systemic hemodynamic. (a) Mean arterial blood pressure (MABP) and (b) heart rate (HR) in control group (white circle), low to medium dobutamine (L-M) dose group (black triangle) and medium to high dobutamine (M-H) dose group (black square). Data are expressed as mean and SD. *P < 0.05 vs. Control group (one-way ANOVA), §P < 0.05 vs. pretreatment (Student’s paired t test) and †P < 0.05 vs. control group (two-way repeated-measures ANOVA as a function of group and time).

The effect of dobutamine infusion in systemic hemodynamic indexes. (a) Cardiac index, (b) systemic vascular resistance index and (c) stroke volume index in control group (white circle), low to medium dobutamine (L-M) dose group (black triangle) and medium to high dobutamine (M-H) dose group (black square). Data expressed as mean and SD. *P < 0.05 vs. control group (one-way ANOVA), §P < 0.05 vs. pretreatment (Student’s paired t-test) and †P < 0.05 vs. control group (two-way repeated-measures ANOVA as a function of group and time).
All dobutamine doses significantly increased CI with an increase in HR and a significant decrease of SVRI compared to pretreatment points but with no change in stroke volume index ( Figures 3 and 4 ). However, only the M-H group showed higher CI and lower SVRI than controls with a significant increase in HR, at two given dobutamine doses (15 and 20 μg/kg/min) while L-M group showed a significant increase of CI with an increase in HR only after 15 μg/kg/min dobutamine administration compared to controls.
Mean arterial blood pressure values fell below baseline values after hypoxia, during reoxygenation and after different dobutamine dose administration. MABP was maintained stable along the time without significant alteration between groups. Meanwhile, CVP of 6–8 mmHg was maintained without changes among groups or in relation to any of the doses.
Systemic Oxygen Metabolism and Transport
At baseline, there were no differences among groups in any of the systemic oxygen metabolism and transport parameters. Two hours of hypoxia produced a significant decrease in arterial oxygen content (CaO2), oxygen delivery (OD), and oxygen consumption (VO2) ( Table 1 and Figure 5 ) with a significant increment of systemic FTOE (P < 0.05 vs. baseline).

The effect of dobutamine infusion in systemic oxygen metabolism. (a) Oxygen delivery (OD), (b) oxygen consumption (VO2) and (c) oxygen extraction (FTOE) in control group (white circle), low to medium dobutamine (L-M) dose group (black triangle) and medium to high dobutamine (M-H) dose group (black square). Data expressed as mean and SD. *P < 0.05 vs. control group (one-way ANOVA), §P < 0.05 vs. pretreatment (Student’s paired t-test) and †P < 0.05 vs. control group (two-way repeated-measures ANOVA as a function of group and time).
The administration of all dobutamine doses produced a significant increase in OD in comparison to controls. However, only the 10–15 μg/kg/min dobutamine doses resulted in VO2 increment without changes in CaO2 and FTOE.
Peripheral tissue oxygenation index (pTOI) and peripheral intravascular oxygenation (pIO2) measured by NIRS showed a significant decrease at the end of hypoxia (pTOI: 58 ± 5 vs. 26 ± 9; pIO2: −2 ± 2 vs. −53 ± 6). After 60 min of reoxygenation, these parameters recovered partially in all animals (pTOI: 49 ± 5; pIO2: −19 ± 5). Only the L-M group showed a significant improvement of regional circulation and oxygen saturation after first (pTOI: 54 ± 4 vs. 49 ± 5; pIO2: −10 ± 4 vs. −19 ± 5) and second (pTOI: 56 ± 3 vs. 52 ± 4; pIO2: −6 ± 3 vs. −13 ± 2) dobutamine dose administration compared to baseline.
Biochemical and Histological Analysis
Baseline serum cardiac troponin T levels were 202 ± 124 pg/ml. After 6 h of experimental period, the controls showed a nonsignificant increase of troponin T levels to 317 ± 159 pg/ml. In contrast, the piglets given dobutamine groups showed similar cardiac troponin T levels compared to baseline (L-M group: 171 ± 38 pg/ml and M-H group: 186 ± 97 pg/ml). At the end of the experimental period, serum creatine kinase (CK) activity was significantly increased in controls (121 ± 63 U/l) in comparison with 15–20 μg/kg/min (43 ± 6 U/l) (P < 0.05) and 10–15 μg/kg/min (58 ± 18 U/l) (P = 0.06).
Necropsies at the end of the experiment revealed acute hemorrhagic foci and mild diffuse congestion in myocardium in four of the six controls. However, ventricular pathological changes were observed in only one animal in the 10–15 μg/kg/min dobutamine group and in two animals in 15–20 μg/kg/min dobutamine group.
Discussion
In these newborn piglets, induction of hypoxia led to cardiovascular abnormalities such as hypotension, metabolic acidosis, decrease in CI and SVCF as well as an increase in biochemical markers such as serum troponin T and CK. We found that the new dobutamine formulation causes a significant increase in CI, HR and OD without changes in MABP or SV. Only the administration of 10–15 μg/kg/min showed a significant increase in VO2 and pTOI and pIO2.
SVCF can be used to assess systemic blood flow in newborn infants, of which approximately 80% goes to the brain (9). In the crucial early postnatal period, SVCF may allow for a more accurate assessment of the status of systemic blood flow and response to different treatments as it is unaffected by cardiac shunting from the patent foramen ovale or ductus arteriosus (10). Although echocardiographic SVCF measurements are used in neonates, in newborn piglets it is quite difficult due to the piglet chest anatomy. To overcome this problem, we measured SVCF using a transit time ultrasound flow probe which is considered the standard reference method for cardiac output measurements in an animal model (11). In our model, a positive correlation was observed when SVCF was compared with CI before, after hypoxia period and during dobutamine administration. While it must be acknowledged that the method used to measure SVCF is very different to that used in human neonates, this study indicates that it is a biomarker, when measured accurately, reflects systemic blood flow. This is backed up by recent research showing that a new modified echocardiographic technique of measuring SVCF in human neonates correlates better with phased contract MRI measurements of SVCF.
In neonatal asphyxia, it is important to monitor CO and blood pressure because multisystem involvement includes hypotension and low CO. CO measurement using a technique of transpulmonary indicator dilution or ventricular outputs by echocardiography has been increasingly used (12). Dobutamine is a drug that primarily stimulates β-1 receptors, leading to increase inotropic and chronotropic effects and to a lesser extent, stimulates β-2 adrenergic receptors, leading to vasodilatation (decrease of SVRI). This combination of effects contributes to increase CO with decreased SVR (13,14). Previous animal research using neonatal animal models have observed that during the short-term dobutamine administration (10 min) the increase in CO is related to the chronotropic effects (increasing HR) (15), whereas the long-term (2 h) infusion demonstrated inotropic effects (increasing SV) (16). In our study, we found that the increase in CO after short-time dobutamine infusion was mainly due to the increased in HR rather than SV. Interestingly due to hypoxia, the piglets had high HR values prior to dobutamine administration, so although the increase in CO was found to be directly related to HR, this effect was attenuated at HR values of approximately 250 bpm, attenuating the dose–response effect. Neonates reliance on increasing cardiac output through increasing their heart rate, due to a reduced ventricular diastolic compliance and an under-development of the neonatal myocyte which makes the heart being less able to respond to volume loading (17).
The effect of dobutamine on MABP during neonatal period was variable. Consistent with other reports, our findings showed that dobutamine infusion had no significant effect on MABP (16,18). A weak correlation between MABP and CO in preterm infants has been demonstrated (19) this is why MABP is not considered a good marker for CO. Therefore, the use of MABP as a measure of the inotropic action of dobutamine is unreliable, and direct flow measurement is needed. In fact, at short-term infusions, dobutamine did not correct the low MABP seen in hypoxic piglets, although it did increase CO and SVCF. These data are similar to that obtained by Devictor et al. in 1988 in six full-term human neonates with severe perinatal asphyxia. They demonstrated a significantly increased in CO, HR and aortic blood flow velocity after 10 µg/kg/min of dobutamine administration (20). The MABP increased but not significantly and SV remained unchanged (20). Therefore for effective increases in MABP and CO while caring for newborn infants recovering from perinatal asphyxia, another agent with vasopressive action such as dopamine or noradrenaline may be added to dobutamine infusion.
In our study, severe hypoxia resulted in a significant decrease of CaO2, and VO2 with an increase of FTOE due to the decrease in OD. Moreover, the reoxygenation period resulted in a recovery of VO2 values with a partial recovery of FTOE and OD. Dobutamine therapy has been suggested to increase tissue metabolic rate in healthy newborn lambs (21) whereas in hypoxic piglets, OD increase was not accompanied by changes in VO2 or FTOE (18). In our study, the administration of 10–15 μg/kg/min of dobutamine in hypoxic newborn piglets produced a significant increase in VO2 probably due to the effect of dobutamine on OD (due to better CI) without changes in CaO2 and FTOE, while higher dobutamine doses did not show significant increase of VO2. This effect has also been previously observed in adult patients where dobutamine effects on oxygen metabolism were observed at lower doses but not at higher doses (22). To assess if these changes would have beneficial effects, the infusion and experiment duration should be maintained over a prolonged period of time.
There is a great interest in the use of NIRS technology in the neonatal intensive care unit (NICU) as a continuous, noninvasive bedside monitoring technique to monitor adequacy of tissue oxygen metabolism and perfusion (23). Measurements of the renal pTOI and pIO2 give insight into peripheral perfusion in general and into renal end-organ function (24,25). Regional saturation changes exceeding >20% from baseline would be reason for concern and may indicate compromised perfusion. In our experiment, renal pTOI and pIO2 measured by NIRS showed a significant decrease (> 40%) during hypoxia, suggesting a compromise in peripheral perfusion. During reoxygenation, these values were partially restored and only in L-M group the administration of dobutamine doses result in an improvement of regional circulation and oxygen saturation. This effect in regional tissue oxygenation during low to medium dobutamine infusion was also observed in healthy neonatal piglets (26), not found differences at higher doses.
Limitations
This experimental piglet model used in our study attempts to mimic the clinical phenomenon of neonatal hypoxia that results in low CO, hypotension, and a profound metabolic acidosis. However, as with all animal models of human disease there may be inter-species differences that limit the transferability of any results. For example, our piglet model of hypoxia does not seem to induce the hypercapnia seen with human neonates experiencing asphyxia which may influence the cardiovascular recovery. It is important to also recognize that the invasive method of measuring SVCF is very different to what is used in the clinical domain. However, this is due to the constraints of the thoracic cavity.
Conclusion
In summary, the new pediatric dobutamine formulation improved hemodynamic status in hypoxic neonatal piglets, with dose-specific differences in metabolic response. SVCF seems to be a promising measure of CO and we will be investigating its value in subsequent longer-term clinical trials of this new formulation. The pattern of change seen in response to the new dobutamine was encouraging and justifies longer-term studies in human neonates.
The new age appropriated dobutamine formulation due to the reduction of sodium metabisulfite levels and presentation, is expected to improve safety in relation to possible adverse events and potential medication errors. So, further studies are needed to evaluate long-term multisystem organ functions and neurodevelopmental outcome.
Special Dedication
This manuscript is dedicated to the life of Adolf Valls-i-Soler who passed away in December 2013 after the experimental part of this work was completed.
Statement of Financial Support
This research has been funded through the European Commission Seventh Framework Programme FP7 HEALTH-F5-2011 under grant agreement n° 282533.
Disclosure
The authors declare that no competing interests exist.
References
Shah P, Riphagen S, Beyene J, et al. Multiorgan dysfunction in infants with post-asphyxial hypoxic-ischaemic encephalopathy. Arch Dis Child Fetal Neonatal Ed 2004;89:F152–F155.
Rozé JC, Tohier C, Maingueneau C, Lefèvre M, Mouzard A. Response to dobutamine and dopamine in the hypotensive very preterm infant. Arch Dis Child 1993;69(1 Spec No):59–63.
Noel GJ, Van Den Anker JN, Lombardi D, Ward R. Improving drug formulations for neonates: making a big difference in our smallest patients. J Pediatr 2012;161:947–9.
Chapados I, Cheung PY. Not all models are created equal: animal models to study hypoxic-ischemic encephalopathy of the newborn. Neonatology 2008;94:300–303.
Evans N, Kluckow M. Early determinants of right and left ventricular output in ventilated preterm infants. Arch Dis Child Fetal Neonatal Ed 1996;74:F88–94.
Evans N, Kluckow M, Simmons M, et al. Which to measure, systemic or organ blood flow? Middle cerebral artery and superior vena cava flow in very preterm infants. Arch Dis Child Fetal Neonatal Ed 2002;87:F181–184.
Cheung PY, Gill RS, Bigam DL. A swine model of neonatal asphyxia. J Vis Exp 2011;56:3166.
Bravo MC, Bravo Mdel C, López P, et al. Acute effects of levosimendan on cerebral and systemic perfusion and oxygenation in newborns: an observational study. Neonatology 2011;99:217–23.
Drayton MR, Skidmore R. Vasoactivity of the major intracranial arteries in newborn infants. Arch Dis Child 1987;62:236–40.
Kluckow M, Evans N. Superior vena cava flow in newborn infants: a novel marker of systemic blood flow. Arch Dis Child Fetal Neonatal Ed 2000;82:F182–187.
Dean DA, Jia CX, Cabreriza SE, et al. Validation study of a new transit time ultrasonic flow probe for continuous great vessel measurements. ASAIO J 1996;42:M671–6.
de Waal K, Kluckow M. Functional echocardiography; from physiology to treatment. Early Hum Dev 2010;86:149–54.
Noori S, Seri I. Neonatal blood pressure support: the use of inotropes, lusitropes, and other vasopressor agents. Clin Perinatol 2012;39:221–38.
Mahoney L, Shah G, Crook D, Rojas-Anaya H, Rabe H. A literature review of the pharmacokinetics and pharmacodynamics of dobutamine in neonates. Pediatr Cardiol 2016;37:14–23.
Fiser DH, Fewell JE, Hill DE, Brown AL. Cardiovascular and renal effects of dopamine and dobutamine in healthy, conscious piglets. Crit Care Med 1988;16:340–5.
Cheung PY, Barrington KJ, Bigam D. The hemodynamic effects of dobutamine infusion in the chronically instrumented newborn piglet. Crit Care Med 1999;27:558–64.
Romero T, Covell J, Friedman WF. A comparison of pressure-volume relations of the fetal, newborn, and adult heart. Am J Physiol 1972;222:1285–90.
Al-Salam Z, Johnson S, Abozaid S, Bigam D, Cheung PY. The hemodynamic effects of dobutamine during reoxygenation after hypoxia: a dose-response study in newborn pigs. Shock 2007;28:317–25.
Kluckow M, Evans N. Relationship between blood pressure and cardiac output in preterm infants requiring mechanical ventilation. J Pediatr 1996;129:506–12.
Devictor D, Verlhac S, Pariente D, Huault G. [Hemodynamic effects of dobutamine in asphyxiated newborn infants]. Arch Fr Pediatr 1988;45:467–70.
Penny DJ, Sano T, Smolich JJ. Increased systemic oxygen consumption offsets improved oxygen delivery during dobutamine infusion in newborn lambs. Intensive Care Med 2001;27:1518–25.
Krachman SL, Lodato RF, Morice R, Gutierrez G, Dantzker DR. Effects of dobutamine on oxygen transport and consumption in the adult respiratory distress syndrome. Intensive Care Med 1994;20:130–7.
Murkin JM, Arango M. Near-infrared spectroscopy as an index of brain and tissue oxygenation. Br J Anaesth 2009;103 Suppl 1:i3–13.
Nagdyman N, Ewert P, Peters B, Miera O, Fleck T, Berger F. Comparison of different near-infrared spectroscopic cerebral oxygenation indices with central venous and jugular venous oxygenation saturation in children. Paediatr Anaesth 2008;18:160–6.
Sakamoto T, Jonas RA, Stock UA, et al. Utility and limitations of near-infrared spectroscopy during cardiopulmonary bypass in a piglet model. Pediatr Res 2001;49:770–6.
Nachar RA, Booth EA, Friedlich P, et al. Dose-dependent hemodynamic and metabolic effects of vasoactive medications in normotensive, anesthetized neonatal piglets. Pediatr Res 2011;70:473–9.
Acknowledgements
The skilled technical assistance of Estibaliz Ruiz del Yerro is gratefully acknowledged. This study has been performed as part of the Neo-CIRCulation Project. The members of the consortium are outlined below: Chief Investigator: Adelina Pellicer, Madrid, Spain. Principal Project Co-ordinator: Heike Rabe, Brighton, UK. Local Investigators: Philip Amess, Neil Aiton, Ramon Fernandez, Liam Mahoney, Heike Rabe, Hector Rojas-Anaya, Brighton, UK; Vincent Jullien, Thomas Le Saux, Gerald Pons, Paris, France; Frank Biertz, Wolfgang Büter, Armin Koch, Hannover, Germany; Victoria Mielgo, Adolf Valls-i-Soler, Bizkaia, Spain; Wolfgang Göpel, Christoph Härtel, Lübeck, Germany; Mark Turner, Michael Weindling, Liverpool, UK; Claudia Roll, Datteln, Germany; Maria del Carmen Bravo, Fernando Cabanas, Madrid, Spain; Simon Bryson, Cheshire, UK; Alexandrina Tatu, Adrian Toma, Bucharest, Romania; Gabriela Zaharie, Cluj-Napoca, Romania; Géza Bokodi, Miklós Szabó, Budapest, Hungary; Tibor Ertl, Simone Funke, Pécs, Hungary; Ebru Ergenekon, Kivilcim Gücüyener, Şebnem Soysal, Ankara,Turkey; Olaf Dammann, Jennifer Lee, Boston, US; Neo-Circulation Expert Advisory Board: Tonse N. K. Raju, Bethesda, USA; Nicholas Evans, Sydney, Australia; Stephanie Läer, Düsseldorf, Germany; Silke Mader, Karlsfeld, Germany; Monika Seibert-Grafe, Mainz, Germany. Neo-Circulation Data Monitoring Comittee: Gorm Greisen, Copenhagen, Denmark; Lena Hellström-Westas, Uppsala, Sweden; Josef Högel, Ulm, Germany.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article

Cite this article
Mielgo, V., Valls-i-Soler, A., Lopez-de-Heredia, J. et al. Hemodynamic and metabolic effects of a new pediatric dobutamine formulation in hypoxic newborn pigs. Pediatr Res 81, 511–518 (2017). https://doi.org/10.1038/pr.2016.257
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2016.257
