
Abstract
Background:
In adults, anthropometric measures of central adiposity, such as waist-height ratio (WHtR) and waist circumference (WC), are more strongly associated with cardio-metabolic risks than BMI.
Methods:
To provide similar quantitative tools for North American children, we created smoothed centile charts and LMS tables for WHtR and WC based on data from the US National Health and Nutrition Survey, cycle III (NHANES III, N = 11,930 aged 2–24 y 1988–1994).
Results:
Applying these reference charts to subsequent NHANES survey cycles, 1999–2012) demonstrated a significant mean increase in both Z-scores of approximately 0.30 SD. In measuring the strength of the association between anthropometric measures and cardio-metabolic risk factors, a unit change in Z-scores for WHtR, WC, and BMI significantly increased the odds of an adverse outcome in all cases (1.18–2.03, P < 0.0001). Z-scores for both measures of central adiposity were significantly more strongly associated with cardio-metabolic comorbidities than BMI-Z.
Conclusion:
Since Z-scores permit standardized comparisons across ages and genders, they are useful measures of central adiposity in both clinical or research settings. By providing LMS tables for children and adolescents based on North American reference data, we hope to provide quantitative tools for the study of obesity and its complications.
Similar content being viewed by others

Main
With increasing prevalence of obesity at younger ages, anthropometric measures other than BMI have been proposed as predictors for the development of cardio-metabolic risks, such as diabetes and hyperlipidemia. In particular, a waist-height ratio (WHtR) > 0.5 has been shown to be a stronger predictor than BMI at all ages, presumably because the former is a better direct measure of central adiposity (1,2,3). Nevertheless, this “one-size-fits all” approach to WHtR ignores the natural variation of this measure with age and gender in children and adolescents.
In younger subjects, waist circumference (WC) has also been shown to be at least as strong a predictor as BMI for metabolic complications (4,5). Although several groups have applied the LMS model to create smoothed centile charts for waist-circumference in North American children and adolescents (6,7,8), none published tables of LMS parameters needed to calculate Z-score or exact centiles in subsequent studies. In addition to dissimilarities between populations, there were also differences in measurement techniques: Although both Statistics Canada and NHANES recommend a validated protocol for measuring WC at the level of the iliac crest in the mid-axillary line (9), reference data from outside North America are often based on different choices for the physical landmarks used to measure WC (see Discussion for details).
Our primary objective was to apply the LMS method to create gender-specific reference growth charts for both WHtR and WC in children aged 5–19 y of age in the North American NHANES III cohort (1988–1994), a North American reference population that predates much of the recent increase in obesity prevalence. The LMS method is currently the most common method for creating growth references, used by both the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO). The method summarizes growth data in terms of three parametric curves, where the L curve captures the skewness of the distribution, the M curve represents its median, and the S curve describes the coefficient of variation. Once fitted, age and gender-specific LMS tables are used to calculate Z-scores and centiles. Secondary objectives included examining the evolution of both WC and WHtR Z-scores in subsequent biennial NHANES surveys A-G (1999–2012) and evaluating the utility of these Z-scores as predictors of metabolic comorbidities.
Results
Our reference growth charts for WC and waist-height ratio vs age are based on data from the NHANES III survey 1988–1994, part of an ongoing National Health and Nutrition Survey for both children and adults. Data were available for 6,140 females and 5,790 males aged 2–24 y from NHANES III (1988–1994). For testing these curves, an additional 10,018 females and 10,227 males aged 5–19 y were available from subsequent biennial NHANES cycles A-G (1999–2012).
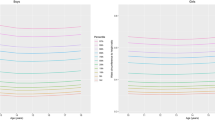
Figure 1 shows considerable variation in both WC and WHtR with age and gender. Moreover, in panels c,d (WHtR vs. age), the dotted horizontal line marks the 0.5 ratio associated with adverse outcomes in adult studies, which fails to track any particular pediatric centile. For both measures, the asymmetry in centile curves on either side of the median speaks to a rightward skew in their distributions, which the LMS model is designed to accommodate. For this reason, the reference charts were supplemented with the LMS parameters in Table 1 , which can be used to calculate exact centiles and Z-scores for each physical measure. A more granular tabulation with monthly intervals is provided in the electronic supplement for researchers and providers of electronic medical records (Supplementary Table S1 online).

(a,b) Smoothed waist circumference centiles (girls and boys, 5–19 y). (c,d) Smoothed waist-height ratio centiles (girls and boys, 5–19 y). Smoothed centiles were fitted to reference data for each gender using the LMS model. The dotted line in panels c,d marks the empiric cut-off of WHtR = 0.5 for comparison with specific pediatric centiles.
Figure 2 graphically displays a shift in mean WC Z-scores as a function of age since NHANES III. For clarity, cycles A-C (1999–2004) and D-G (2005–2012) were pooled. There was a noticeable shift at all ages compared to the NHANES III reference (1988–1994). A comparable shift was observed in mean WHtR Z-score over time (not shown).

Mean waist circumference Z-scores over time. Waist circumference Z scores were calculated based on NHANES III reference curves and smoothed using penalized regression splines: NHANES III (solid line), NHANES A-C (dashed line), and NHANES D-G (dotted line). Gray shading denotes the corresponding 95% confidence intervals. Biennial NHANES cycles A-G (1999–2012) did not differ significantly from each other (not shown).
In Table 2 , the unadjusted mean Z-scores have moved by 0.33–0.35 SD since the reference period, which was not changed by adjustment for gender and race-ethnicity. Further heterogeneity was seen with adjustment, since the mean score for Black children was significantly lower than for White children, while the mean score for Mexican-American children was higher. Only one interaction term achieved statistical significance, with female subjects in later NHANES cycles showing a small increase (ΔZ = 0.1, P < 0.001) in WHtR-Z and a similar trend for WC-Z (ΔZ = 0.06, P = 0.07), indicating that the increase over time was greater in girls than boys. No significant differences were noted in mean scores between early (1999–2004) and later (2005–2012) survey eras (see Figure 2 ).
For subjects studied between 1999 and 2012, Table 3 summarizes the odds ratios (OR) for an adverse metabolic outcome (as defined in Methods) associated with a unit increase in Z-scores for WC, WHtR, or BMI. All ORs differ significantly from the null, with 95% CI’s that do not cross 1. In all cases, WC-Z and WHtR-Z are more strongly associated with metabolic risk factors than BMI-Z. From the formal pairwise comparisons, we see that the WHtR-Z outperforms BMI-Z for abnormal total cholesterol (TC), low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), and triglycerides (TG), P < 0.05; and WC-Z is superior to BMI as a predictor for abnormal HDL and TG. Compared to BMI, WC and WHtR are both stronger predictors of elevated glycated hemoglobin levels, but the pair-wise differences do not achieve statistical significance.
As suggested by these results, these three Z-scores are not necessarily concordant. In NHANES cycles A-G (N = 20,245), BMI-Z was generally higher than the corresponding waist-based measures. Between WC-Z and BMI-Z, the mean (±SD) within-subject difference was −0.44 ± 0.68 (Pearson correlation r1 = 0.89). In contrast, the mean difference between WHtR-Z and BMI-Z was - 0.60 ± 0.71 (r2 = 0.88). The two measures of central adiposity were more consistent, with a mean difference (WHtR-Z - WC-Z) of 0.15 ± 0.42 with a correlation r3 = 0.92.
Our LMS tables are based on North American reference data and a standardized measurement protocol. In Figure 3 , we see how the median WC in our NHANES III cohort compares to the corresponding centile in other studies, reflecting differences in both reference populations and measurement techniques.

Median waist circumference (WC, cm) as a function of age (a = female, b = male). NHANES III (solid line) is compared to alternative reference populations from the UK (18 •), Australia (19 ◦), the Netherlands (20 +), and Germany (21 ◇; 22 ▴). Much of the observed variation is due to differences in the technique used to identify landmarks to measure WC (9), e.g. at the level of the umbilicus (19), at the narrowest point between the costal margin and the iliac crest (20,21,22), mid-way between the costal margin and the iliac crest (18), or at the level of the iliac crest in the mid-axillary line, the latter applied consistently across NHANES cycles (23).
Discussion
Given the variation in both WHtR and WC across ages and genders, the primary goal of this study was to produce LMS tables based on North American data so that clinicians and investigators can easily calculate Z-scores and exact centiles for both anthropometric measures of central adiposity. In addition to their role in epidemiologic studies of obesity and cardiovascular risk, growth charts are familiar tools that are easily applied by health-care workers in a clinic setting for both screening and longitudinal follow-up of individual patients.
For adults, a recent meta-analysis of over 300,000 subjects of both genders and varied ethnicities (10) concluded that WHtR and WC were better screening tools for cardio-metabolic risk factors than BMI, presumably because they better reflect central adiposity than BMI (weight/height2), which can be distorted by nonfat mass (e.g., muscle) and visceral adiposity. WHtR may be a particularly powerful instrument in specific ethnic groups, like South Asians, where BMI and WC have relatively poorer sensitivity and specificity (11).
Although BMI is the standard measure of overweight and obesity in children and adolescents (12,13,14,15), large cross-sectional population surveys, such as NHANES and the Bogalusa Heart Study, have demonstrated the superiority of WHtR over BMI for identifiying cardiovascular disease (CVD) risk factors in children (12,13,14,15). WC has also been proposed as an alternate measure, with performance at least comparable to BMI (5,6). Smaller prospective pediatric series (4) have also confirmed the prognostic value of WC at age 8 y as a predictor of future CVD risk-factor clustering.
Unlike adult studies, the thresholds of concern have been less clearly defined for children and adolescents. Following adult conventions, a simple cut-off of 0.5 or 0.6 for WHtR has been proposed (1,2,3,16,17), an approach that ignores the variation in WHtR with age and gender seen in Figure 1 . To our knowledge, neither growth charts nor LMS tables have previously been reported for pediatric WHtR despite the observed variation in expected values with age and gender.
More work has been done to define normal age- and gender-specific WC. In fact, several sets of pediatric WC growth charts (i.e., smoothed centile plots) have been produced with North American data (Katzmarzyk Fitness Canada Survey, Cook et al. NHANES data, Katzmarzyk Bogalusa, Fernandez NHANES III). Unfortunately, none of these reports included LMS tables for calculating Z-scores and centiles in subsequent studies. Nevertheless, LMS tables are available for WC in children in the UK (18), Australia (19), the Netherlands (20), and Germany (21,22). In addition to focusing on specific age ranges (e.g., 11–18 y), these charts also differ nontrivially in the measurement technique used to evaluate WC, e.g., at the level of the umbilicus (19), at the narrowest point between the costal margin and the iliac crest (20,21,22), mid-way between the costal margin and the iliac crest (18), or at the level of the iliac crest in the mid-axillary line, the last consistently applied across NHANES cycles (23). Given the extent of the variation in normal WCs across studies ( Figure 3 ), practitioners should take care to align their clinical measurement methods with those actually used to create their reference charts. This is particularly true given systematic differences in WC obtained by the various methods, with the NHANES protocol yielding consistently higher measurements in cross-over studies on the same subjects aged 3–79 y (9).
Even when WC growth charts have been available, appropriate levels of concern remain unclear. At least one cross-sectional report from the Bogalusa Heart Study included pediatric percentile cut-offs chosen on the basis of their association with adverse CVD risk factors (5), with percentiles of risk ranging from the 50th–57th for WC, depending on race and gender. Through comparison with BMI criteria, investigators in the UK (24) and Australia (4) defined overweight and obesity as WC values exceeding age- and gender-specific 91st or 98th percentile values. Cook et al. have suggested that cut-offs be defined by aligning adult levels of concern (102 cm in males and 88 cm in females – (6)) with pediatric centiles at age 19 y. For the NHANES III reference data presented here, these cut-offs would correspond to the 93rd and 75th percentiles, respectively. Were we to adopt a similar approach to WHtR, the adult threshold of 0.5 corresponds to the 65th percentile in girls and the 77th percentile in boys in Figure 1c , d . These definitions are similar to those adopted by the WHO to define overweight in children aged 2–19 y as the 85th percentile for BMI, which aligns at age 19 y with the adult definition at a BMI of 25 kg/m2 (13). Clearly, all such criteria are provisional, pending definitive prospective trials to examine the association between specific centiles and long-term cardiovascular outcomes.
Although Z-scores provide a meaningful comparison of WC across ages and genders and are particularly well-suited for intervention trials, few studies have adopted this approach (4,24). Z-scores are also useful for quantitative comparisons when percentile scores cluster near or above the 99th percentile, since such scores are otherwise difficult to distinguish. Moreover, Garnett (4) reported CVD risk-factor associations with Z-scores based on the 1985 Australian Health and Fitness Survey (ages 7–15 y), but the LMS tables used for these calculations were based on data collected using a different methodology (measurement at the umbilicus) than NHANES. Clearly, careful adherence to a standardized measurement protocol is a prerequisite to using these charts, and the NHANES measurement protocol, based on easily identifiable physical landmarks, represents a long-standing North American standard (23).
The primary aim of the current study was to tabulate LMS parameters for both WC and WHtR, which might be used to calculate Z-scores and exact centiles based on North American norms and to provide quantitative tools for evaluation of both measures of central adiposity in growing children. We deliberately selected data from NHANES III (1988–1994) to create these reference charts for the same reason that WHO 2007 (NCHS, 1963–1975) and CDC 2000 (NCHS, 1963–1994) growth reference charts for ages 5–19 y excluded more recent data to minimize the impact of the North American obesity epidemic (7,13,14,25). Like the WHO and CDC charts for school-aged children, these norms are also presented as a growth reference rather than a prescriptive growth standard, intended to be used as a yardstick for measuring change (13). In this light, Figure 2 and Table 2 clearly demonstrate a mean shift of 0.30–0.35 SD since NHANES III despite application of a consistent measurement technique by trained NHANES staff. Similar trends have been reported by others (16,17,24). We must therefore assume that this represents a real shift in the population distribution. The results in Table 2 also illustrate additional heterogeneity, particularly with regards to ethnicity, with lower scores in Black children and higher scores in Mexican-American children. Since South Asians may also differ in propensity to cardio-metabolic complications (11), it is perhaps unfortunate that the race-ethnicity data in the NHANES surveys do not permit further parsing of these distinctions, though Asian ethnic origin was added with the most recent NHANES cycle.
In our exploratory analysis of the association of anthropometric measures with cardio-metabolic risk factors in subsequent NHANES survey cycles, Table 3 confirms that a unit change in all three Z-scores significantly increased the odds for all adverse metabolic outcomes (P < 0.0001). Both WHtR and WC were consistently more strongly associated with abnormal metabolic profiles than BMI. It is intriguing that ORs for WHtR-Z were significantly higher (P < 0.05) than for BMI-Z for 4/4 adverse lipid measurements (TC, LDL, HDL, and TG), and the ORs for WC-Z were significantly higher for HDL and TG. Since the odds ratios in Table 3 were largely unaffected by additional adjustment for sex and race-ethnicity (not shown), we might further infer that these Z-scores capture the impact of central adiposity on CVD risk across genders and races. Due to sample size and age restrictions imposed by the NHANES subsampling protocol (e.g., no fasting specimens below age 12 y), these results should only be considered exploratory. Nevertheless, our findings are consistent with the results of adult studies (10,11).
Morandi et al. (26) have recently commented on the poor receiver operator characteristics associated with all anthropometric measures in pediatric metabolic syndrome, citing areas under the receiver operator characteristics curve (AUC) of 0.55–0.70. Here, too, the best AUC (for HDL < 40 mg/dl) was 0.694 (95% CI 0.682–0.706, not shown), which is significantly better than chance agreement (AUC = 0.5), but of questionable value as a screening test. Nevertheless, prospective evaluation of predictive ability will be needed to further assess their clinical utility (4,6,18,24,27), particularly since childhood adiposity tracks into adulthood (28), and WC and BMI at age 8 y predict subsequent clustering of CVD risk factors (4).
In adopting the National Cholesterol Education Panel cut-points to define metabolic comorbidities, we recognize that alternate definitions are also possible (see ref. (29)). For example, the AAP Committee on Nutrition (30) recommended a low HDL cut-point of 35 mg/dl, which decreases the number of adverse outcomes from N = 2,861 to 1,108 and increases the strength of the association with WHtR-Z (OR = 2.17, CI = 2.04–2.32) and WC-Z (OR = 2.23, CI = 2.08–2.39).
Strengths and Limitations
The strengths of this study are the robust sample size, the standardized NHANES anthropometric measurement protocol, the quality of the (NHANES III) reference data, and the application of a well-accepted statistical methodology in the LMS model for skewed distributions. Weaknesses reflect the lack of longitudinal or prospective data, as well as the relative paucity of biochemistry results for younger children. Consequently, the tests of association between anthropometric measures of central adiposity and adverse metabolic outcomes ( Table 3 ) should only be considered exploratory. As with conventional growth charts, lack of concurrent data on pubertal stage may also blur important clinical distinctions (12,13).
Conclusions
In adults, anthropometric measures of central adiposity, such as WHtR and WC, are more strongly associated than BMI with adverse cardio-metabolic outcomes. Given systematic variations in these measures across ages and genders, LMS tables for calculating Z-scores and centiles based on North American reference data are needed to make quantitative comparisons, but are not readily available in published form. By choosing NHANES III as a reference population, our tables minimize the impact of the North American obesity epidemic, seen here as a shift of 0.30–0.35 SD in both Z-scores between NHANES III and subsequent survey cycles. Moreover, these norms are based on well-established measurement methods applied consistently over time. In cross-sectional analyses, we see that WHtR-Z and WC-Z are more strongly associated than BMI-Z with abnormal lipid profiles in children and adolescents in the NHANES database. We therefore hope that other investigators will be able to apply these quantitative tools in longitudinal studies of obesity and its complications in children and adolescents.
Methods
Anthropometric Data
Reference data were available for age, height, WC, and race-ethnicity for 6,140 females and 5,790 males aged 2–24 y from the US National Health and Nutrition Survey, cycle III (NHANES III, 1988–1994). NHANES III was deliberately designed to be “fairly-close to self- weighting nationally” (31), i.e., nationally representative for the non-institutionalized US population. Beginning with NHANES III and continuing through subsequent biennial cycles (NHANES A-G, 1999–2012), anthropometric measurements were collected using a standardized measurement protocol (23): In brief, calibrated stadiometer heights were measured to the nearest 0.1 cm by trained staff. A snug tape measure was used to measure WC to the closest 0.1 cm after palpating and marking the iliac crests in the mid-axillary lines while subjects placed their hands on their opposite shoulders. Since data were not consistently collected across NHANES cycles, race-ethnicity categories were pooled as European-American (White), African-American (Black), Mexican American (Mex), and Other (7). Ethics approval was obtained from the Health Research Ethics Board of the University of Manitoba’s Faculty of Medicine for the use of anonymous data from an existing database for epidemiologic investigations.
LMS Model
Centiles were fitted to gender-specific reference data for WC and WHtR using the LMS model with LMS Chartmaker Pro 2.5.4 to fit smoothed L (skew), M (median), and S (coefficient of variation) curves (32,33,34): For a given physical measure y, the corresponding Z-score is then given by z = ((y/M)L−1)/(LS), with recommended modifications for Z-scores outside the range −3 to +3 (35). This formula is inverted to yield centile y as a function of Z-score in y = M (1+LSz)(1/L), L ≠ 0. The LMS model assumes that after a Box-Cox power transformation, the data at each age are normally distributed; hence, the normal cumulative distribution function may be used to convert Z-scores into corresponding percentile curves (e.g., with a Gaussian distribution, z = −3, −2, −1, 0, 1, 2, and 3 corresponds roughly to percentiles 0.1, 3, 15, 50, 85, 97, and 99.9)
Statistical Methods
In R (36), tabulated LMS parameters were used to calculate WC and WHtR Z-scores and centiles for 27,255 subjects aged 5–19 y in NHANES III (N = 7,010) and biennial cycles A-G (N = 20,245, 1999–2012). Published WHO LMS parameters were used calculate corresponding BMI Z-scores, based on their core NHANES dataset for school aged children (1963–1975) (13).
To graphically compare mean Z-scores by age and NHANES cycle, individual Z scores were plotted vs. age and smoothed using quadratically penalized (thin plate) regression splines, with smoothing degrees of freedom selected by generalized cross-validation.
Linear regression was used to assess the mean change in Z-scores by NHANES cycle with and without adjustment for covariates gender (M, F) and race-ethnicity (White, Black, Mexican-American, and Other). Reference categories were NHANES cycle = NHANES III, race-ethnicity = White, and gender = M.
Metabolic Outcomes
To assess the utility of WC and WHtR Z-scores as predictors of metabolic and cardiovascular complications in an out-of-sample validation dataset, laboratory data were pooled and merged with anthropometric measures for all subjects aged 5–19 y in NHANES cycles A-G (1999–2012), with details available in the individual survey manuals (37). Data were available for total cholesterol (TC, N = 17,591, ages 6–19 y), high-density lipoprotein cholesterol (HDL, N = 17,585, aged 6–19 y), low-density lipoprotein cholesterol (LDL, N = 6,195, aged 12–19 y fasting), triglycerides (TG, N = 6,818, aged 12–19 y fasting), and glycated hemoglobin (GH, N = 9,063, aged 6–19 y). For each of these measures, abnormal cut-points were defined by the National Cholesterol Education Panel (38) criteria as TC ≥ 200 mg/dl (N = 1,944 cases), LDL ≥ 130 mg/dl (N = 541 cases), HDL < 40 mg/dl (N = 2,861 cases), TG ≥ 100 mg/dl for 0–9 y or ≥ 130 mg/dl for 10–19 y (N = 1,249 cases). Following current NHANES guidelines, a glycated hemoglobin ≥ 6.5% was classified as diabetes in all surveys (N = 90 cases). For each outcome, logistic regression was used to calculate the odds ratios corresponding to a unit change in Z-scores for WC, WHtR, or BMI.
Statement of Financial Support
No financial support was received for this study.
Disclosures
No conflicts or disclosures.
References
Kahn HS, Imperatore G, Cheng YJ. A population-based comparison of BMI percentiles and waist-to-height ratio for identifying cardiovascular risk in youth. J Pediatr 2005;146:482–8.
Khoury M, Manlhiot C, McCrindle BW. Role of the waist/height ratio in the cardiometabolic risk assessment of children classified by body mass index. J Am Coll Cardiol 2013;62:742–51.
Mokha JS, Srinivasan SR, Dasmahapatra P, et al. Utility of waist-to-height ratio in assessing the status of central obesity and related cardiometabolic risk profile among normal weight and overweight/obese children: the Bogalusa Heart Study. BMC Pediatr 2010;10:73.
Garnett SP, Baur LA, Srinivasan S, Lee JW, Cowell CT. Body mass index and waist circumference in midchildhood and adverse cardiovascular disease risk clustering in adolescence. Am J Clin Nutr 2007;86:549–55.
Katzmarzyk PT, Srinivasan SR, Chen W, Malina RM, Bouchard C, Berenson GS. Body mass index, waist circumference, and clustering of cardiovascular disease risk factors in a biracial sample of children and adolescents. Pediatrics 2004;114:e198–205.
Cook S, Auinger P, Huang TT. Growth curves for cardio-metabolic risk factors in children and adolescents. J Pediatr 2009;155:S6.e15–26.
Fernández JR, Redden DT, Pietrobelli A, Allison DB. Waist circumference percentiles in nationally representative samples of African-American, European-American, and Mexican-American children and adolescents. J Pediatr 2004;145:439–44.
Katzmarzyk PT. Waist circumference percentiles for Canadian youth 11-18y of age. Eur J Clin Nutr 2004;58:1011–5.
Patry-Parisien J, Shields M, Bryan S. Comparison of waist circumference using the World Health Organization and National Institutes of Health protocols. Health Rep 2012;23:53–60.
Ashwell M, Gunn P, Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev 2012;13:275–86.
Jayawardana R, Ranasinghe P, Sheriff MH, Matthews DR, Katulanda P. Waist to height ratio: a better anthropometric marker of diabetes and cardio-metabolic risks in South Asian adults. Diabetes Res Clin Pract 2013;99:292–9.
The Global Resource for Nutrition Practice. Growth Monitoring of Infants and Children Using the 2006 World Health Organization [WHO] Child Growth Standards and 2007 WHO Growth References, 2012. http://www.dietitians.ca/Downloadable-Content/Public/Growth_Charts_backgrounder_eng.aspx.
de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ 2007;85:660–7.
Rodd C, Metzger DL, Sharma A ; Canadian Pediatric Endocrine Group (CPEG) Working Committee for National Growth Charts. Extending World Health Organization weight-for-age reference curves to older children. BMC Pediatr 2014;14:32.
Rolland-Cachera MF. Childhood obesity: current definitions and recommendations for their use. Int J Pediatr Obes 2011;6:325–31.
Li C, Ford ES, Mokdad AH, Cook S. Recent trends in waist circumference and waist-height ratio among US children and adolescents. Pediatrics 2006;118:e1390–8.
Xi B, Mi J, Zhao M, et al.; Public Health Youth Collaborative and Innovative Study Group of Shandong University. Trends in abdominal obesity among U.S. children and adolescents. Pediatrics 2014;134:e334–9.
McCarthy HD, Jarrett KV, Crawley HF. The development of waist circumference percentiles in British children aged 5.0-16.9 y. Eur J Clin Nutr 2001;55:902–7.
Eisenmann JC. Waist circumference percentiles for 7- to 15-year-old Australian children. Acta Paediatr 2005;94:1182–5.
Fredriks AM, van Buuren S, Fekkes M, Verloove-Vanhorick SP, Wit JM. Are age references for waist circumference, hip circumference and waist-hip ratio in Dutch children useful in clinical practice? Eur J Pediatr 2005;164:216–22.
Kromeyer−Hauschild K, Gläßer N, Zellner K. Perzentile für den Taillenumfang von Jenaer Kindern im Alter von 6 bis 18 Jahren. Aktuel Ernaehr Med 2008;33:116–22.
Kromeyer-Hauschild K, Dortschy R, Stolzenberg H, Neuhauser H, Rosario AS. Nationally representative waist circumference percentiles in German adolescents aged 11.0-18.0 years. Int J Pediatr Obes 2011;6:e129–37.
National Health And Nutrition Examination Survey (NHANES). Anthropometry Procedures Manual, 2011. http://www.cdc.gov/nchs/data/nhanes/nhanes_11_12/Anthropometry_Procedures_Manual.pdf2011.
McCarthy HD, Ellis SM, Cole TJ. Central overweight and obesity in British youth aged 11-16 years: cross sectional surveys of waist circumference. BMJ 2003;326:624.
Kuczmarski RJ, Ogden CL, Guo SS, et al. 2000 CDC Growth Charts for the United States: Methods and Development. Washington: National Center for Health Statistics Vital Health Stat, 2002.
Morandi A, Miraglia del Guidice E, Martino F, Martino E, Bozzola M, Maffeis C. The contribution of anthropometry, adiposity, and adiposopathy to cardiometabolic disturbances in obese youth. J Pediatr 2014;165:1178–83.
McCrindle BW. The contribution of anthropometry, adiposity, and adiposopathy to cardiometabolic disturbances in obese youth. J Pediatr 2014;165:1083–4.
Guo SS, Roche AF, Chumlea WC, Gardner JD, Siervogel RM. The predictive value of childhood body mass index values for overweight at age 35 y. Am J Clin Nutr 1994;59:810–9.
Silveira LS, Monteiro PA, Mello Antunes BM. Metabolic syndrome: criteria for diagnosing in children and adolescents. Endocrinol Metab Synd 2013;2:1–6.
Daniels SR, Greer FR ; Committee on Nutrition. Lipid screening and cardiovascular health in childhood. Pediatrics 2008;122:198–208.
National Health And Nutrition Examination Survey (NHANES). Sample Design and Analysis Guidelines, 1997. http://archive.nlm.nih.gov/proj/dxpnet/nhanes/docs/doc/nhanes3/lab/LAB_sample_design_and_analysis_guidelines.txt.
Cole T, Pan H. LMSChartmaker Pro v. 2.54: A program for calculating age-related reference centiles using the LMS method. 2.54 ed. Medical Research Council UK, 2011.
Cole TJ, Green PJ. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med 1992;11:1305–19.
Rigby RA, Stasinopoulos DM. Smooth centile curves for skew and kurtotic data modelled using the Box-Cox power exponential distribution. Stat Med 2004;23:3053–76.
WHO Multicentre Growth Reference Study Group. WHO child growth standards: length/height-for-age, weight-for-age, weight-for-length, weight-for- height and body mass index-for-age: Methods and development. Geneva: World Health Organization Press, 2006.
R Core Team, R Foundation for Statistical Computing. R: A language and environment for statistical computing; 2015. http://www.R-project.org/.
National Health And Nutrition Examination Survey (NHANES). Laboratory Procedure Manuals, 2012. http://www.cdc.gov/nchs/nhanes/nhanes2011-2012/manuals11_12.htm2012.
Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report. Pediatrics;128:S213–S56.
Author information
Authors and Affiliations
Corresponding author
Supplementary information
Supplementary Table S1
(XLS 159 kb)
Rights and permissions
About this article

Cite this article
Sharma, A., Metzger, D., Daymont, C. et al. LMS tables for waist-circumference and waist-height ratio Z-scores in children aged 5–19 y in NHANES III: association with cardio-metabolic risks. Pediatr Res 78, 723–729 (2015). https://doi.org/10.1038/pr.2015.160
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2015.160
This article is cited by
-
Physical activity and its impact on cardiovascular health in pediatric kidney transplant recipients
Pediatric Nephrology (2024)
-
Prenatal and childhood exposure to per-/polyfluoroalkyl substances (PFASs) and its associations with childhood overweight and/or obesity: a systematic review with meta-analyses
Environmental Health (2023)
-
The significance of central blood pressure for cardiovascular target organ damage in children and adolescents after kidney transplantation
Pediatric Nephrology (2023)
-
Sex Differences in Diet and Physical Activity Behaviors Among Racial/Ethnic Minority Adolescents with High Metabolic Risk
Journal of Racial and Ethnic Health Disparities (2023)
-
Clustering of lifestyle behaviors and adiposity in early adolescents in Spain: findings from the SI! Program for Secondary Schools
BMC Public Health (2023)
