
Abstract
Gastroesophageal reflux disease (GERD) is a frequent consideration in intensive care unit neonates. We tested the hypothesis that symptoms in GERD are dependent on the spatiotemporal and physicochemical characteristics of reflux events by evaluating the symptom sensitivity index (SSI) and symptom index (SI) in relation to the refluxate characteristics. Thirty symptomatic neonates (30.7 ± 0.8 wk gestation) were evaluated using manometry and pH-impedance methods. During 704.3 h of recordings, 2063 gastroesophageal reflux (GER) were observed; 54% of the GER were associated with symptoms. Defined by physical characteristics, there were 51.3% liquid, 29.1% gas, and 19.6% mixed GER. Defined by chemical characteristics, there were 48.5% acid and 51.5% nonacid GER. Defined by most proximal extent, 79.2% were supra-UES (upper esophageal sphincter) and 20.8% were infra-UES. Higher SSI was noted with pH-only events (p < 0.0001 versus pH-impedance events). Higher SI was noted with movement symptoms (versus sensory, p = 0.04). In a subset analysis, the frequencies of GER events, acid clearance time, and SSI were all greater in chronic lung disease versus none (p < 0.001). In conclusion, clinical significance of symptoms as measured by SSI and SI and characterization of spatial-temporal-physical-chemical nature of GER events as defined by pH-impedance methods clarifies the definition of GERD.
Similar content being viewed by others

Main
Gastroesophageal reflux disease (GERD) is a frequent consideration in infants at-risk of life-threatening events, chronic lung disease (CLD), and dysphagia. Concern of GERD in neonates is evident by the frequent use of acid suppressive medications (1) and prokinetics (2) that are commonly prescribed to alter gastric acidity or gastroprokinetic functions. Furthermore, practices in the NICU attribute aerodigestive symptoms to the injurious effects of acid reflux events (ARE). However, the composition of the refluxate varies depending on the composition of the gastric contents, i.e. acid, enzymes, food, gas, bile, swallowed material; albeit, all these have a common factor, i.e. volume. Suppression of gastric acid alone may have been beneficial or associated with side effects (1), and therapies targeted to modify gastroesophageal reflux (GER) and gut motility have noxious consequences (3).
Using pH-impedance techniques, classification of ARE in relation to symptom characteristics in CLD has been determined by us (4). Traditionally, esophageal pH <4 is considered ARE, and all others as nonacid reflux events (NARE) (5). However, significance of measurable characteristics of refluxate such as ARE, NARE, gas, mixed, liquid, high, or low reflux events in relation to symptoms in symptomatic NICU neonates remaining unclear. Therefore, this study was undertaken to 1) classify the physicochemical and spatiotemporal characteristics of GER events, 2) characterize the frequency and distribution of symptoms, 3) define the relationship of symptoms with the characteristics of GER using symptom sensitivity index (SSI) and symptom index (SI), and 4) perform subset analysis among a) those with CLD and those without, and b) differences in symptom distribution within the NARE group in response to pH change versus none.
METHODS
Subjects.
Thirty neonates [median (IQR)] of 30.6 (7.0) wk gestation, 1.4 (1.4) kg at birth were evaluated for suspected GERD at 43.6 (5.6) wk postmenstrual age (PMA) and weighed 3.6 (1.7) kg. None were receiving acid suppressive medications or prokinetics. At assessment, subjects were receiving full enteral nutrition via intragastric feedings or oral feedings and standard respiratory management at the Nationwide Children's Hospital NICU. CLD was defined as the need for supplemental oxygen requirement beyond 36 wk PMA. Informed written consent was obtained before the start of the study, and the protocol was approved by the Institutional Review Board at The Research Institute of Nationwide Children's Hospital.
Manometric methods.
We used the same manometric technique previously used by our group to characterize the esophageal motility waveforms and to define the distance from nares to the upper esophageal sphincter (UES) and the lower esophageal sphincter (LES) (4,6–8). Briefly, the catheter assembly (Dentsleeve International, Mui Scientific, Ontario, Canada) was passed nasally in the supine lying infant, and pull-through techniques were adopted to ensure appropriate positioning (9). The catheter was withdrawn at 0.5-cm intervals with a pause of at least 20 s in each station, until the high pressure zone of the LES or UES were identified by the presence of a constant increase in the pressure above baseline. Change in LES pressure with breathing and swallow induced changes in UES and LES relaxations were observed to ensure proper positioning.
pH-impedance methods.
Twenty-four hour pH-impedance studies were done using the pH-MII probe, model ZIN-S61C01E, (Sandhill Scientific Inc, Highlands Ranch, CO) that had six impedance channels (seven impedance rings) and one pH channel (4). After calibration, the probe was securely set at 87% of the distance from the nares to the upper border of the LES, such that the location of the pH sensor was in the distal esophagus (10). Based on the manometric definitions, the esophageal body length varied between 5.1 and 9.9 cm (median, 7.8 cm), and the pH-impedance probe was of adequate size to use in infant esophageal lengths up to 15 cm.
Documentation of symptoms.
Trained nurse assistants, who were blinded to the recordings, documented the symptoms/caring events upon occurrence. The nurses were well trained to recognize the symptoms objectively. Event markers were placed directly using the touch screen interface for 1) respiratory symptoms (cough, grunting, gagging, bradycardia, and desaturation), 2) sensory symptoms (irritability, arching, grimace, cry, or pain), and 3) physical movement (stretching of limbs). Irritability was characterized by neck extension and arching; and pain in neonates was recognized as grimace, eye convergence, frown, or folds on the forehead or cry.
Data analysis.
Manual analysis was performed to document GER by observing the change in impedance by >50% with retrograde bolus movement (11,12). GER was classified based on the physical property into gas, liquid, and mixed refluxate. Gas reflux was defined as a rapid increase (50% from preepisode mean impedance value) simultaneously in at least two consecutive impedance channels without any evidence of swallowing. Liquid reflux was defined as a 50% decrease from preepisode mean impedance value with retrograde bolus movement starting distally and propagated to at least two more proximal channels. Mixed reflux was defined as combination of liquid and gas reflux (13). GER was also classified based on the chemical property into a) ARE (fall of pH to <4 for >5 s or when the pH decrease of at least 1 pH unit for >5 s if pH was already <4 during liquid presence as determined by MII) and (b) NARE (no decrease in pH to <4 during liquid presence as determined by MII; subset analysis was also performed based on the presence or absence of a pH change of >1 unit for each NARE) (5). Gas reflux was classified into ARE and NARE depending on the association of fall in pH. Spatial characteristics of the GER events were identified by the proximal extent of the refluxate into supra-UES or infra-UES based on the manometric definitions. Temporal characteristics were determined by the duration of the dwell of the refluxate (clearance) within the esophageal column. Bolus clearance time (BCT) was measured from the onset at which impedance decreases below 50% of the baseline to the offset at which impedance returns to 50% of the baseline value. Acid clearance time (ACT) was defined as the time taken for the esophageal pH to normalize to pH ≥4.0 for ≥5.0 s. Artifacts and meal periods were excluded. Symptom-reflux relationships were applied in each of these eight GER characteristics (ARE, NARE, gas, liquid, mixed, high, low, and pH-only events). Any GER was labeled as symptomatic if a symptom presented during the GER and for 2 min after the reflux duration. The same symptom would only be counted once following the GER to overcome the overlap of the same symptom associated with consecutive GER time windows. The SI was calculated [(number of symptoms with reflux events/total number of symptoms in 24 h) × 100] (12,14). We also calculated the SSI [(number of reflux events associated with symptoms/total number of reflux events in 24 h) × 100] (4,12,14,15).
Statistical analysis.
The physical, chemical characteristics, and most proximal extent within the esophagus were tested for association with the symptoms. SSI and SI were calculated. Multinomial mixed models or linear mixed models were used to study the association between BCT and ACT and GER characteristics. In these models, a statement for repeated effect was included to account for the correlation within subjects. These models were fit using PROC GENMOD or PROC MIXED in SAS version 9.1 (SAS Institute Inc., Cary, NC). As data are not normally distributed, values are shown as median (IQR) or as % unless stated otherwise. Log transformation was performed to achieve normality for the statistical analyses (mixed models), and p value <0.05 was considered significant.
RESULTS
Participant characteristics.
Demographic comparisons between CLD and non-CLD are stated (Table 1). At evaluation, 11 (36.7%) infants were oral-fed and the rest via nasogastric tube; and 7 (39%) in the CLD group and 4 (33%) in the non-CLD group received continuous tube feeding (p = NS). At discharge, 15 (50%) were oral-fed exclusively, 7 (23%) were oral and gastrostomy-fed, and 8 (27%) were gastrostomy-fed exclusively.
Classification of GER events: physical, chemical, and spatial characteristics.
Overall, 2063 GER events were recognized by combined MII-pH recordings, of which 1969 (95.4%) were pH-impedance events and 94 (4.6%) were pH-only events. False pH-refluxes caused by pH-fluctuations or electrode drift were ruled out. Physical characteristics of GER revealed that 1010 (51.3%) were liquid, 574 (29.1%) were gas, and 385 (19.6%) were mixed. Chemical characteristics revealed that 954 (48.5%) were ARE and 1015 (51.5%) were NARE. Spatial characteristics were based on the manometric definitions in each patient, and 1559 (79.2%) supra-UES GER and 410 (20.8%) infra-UES GER were identified by the most proximal extent of the refluxate.
Bolus clearance time in relation to physicochemical and spatial characteristics.
Each patient spent median 27.4 (12.5) s per event in bolus clearance of liquid or mixed GER events. Characteristics of BCT per GER event per individual subject data are summarized (Fig. 1A). Prolonged BCT was noted with mixed GER compared with liquid GER by 1.5-fold, (p = 0.0002), and supra-UES GER compared with infra-UES GER by 1.2-fold, (p < 0.0001). Similar BCT was noted between ARE and NARE. Subgroup analysis on median BCT per event per subject was similar between patients with CLD [26.1 (10.5) s] and without CLD [32.9 (9.3) s, p = 0.2].

Duration of average BCT and average ACT per patient per GER event. In (A), average BCT is different based on physical (liquid vs. mixed, *p = 0.0002) and spatial characteristics (high vs. low, ‡p = 0.0001) but similar based on chemical characteristics (acid vs. nonacid, p = NS). In (B), average ACT is longer for pH-only events compared with acid pH-impedance events (**p < 0.0001). The boundary of the box indicates the 25th and 75th percentiles; the solid line within the box marks the median value; and the error bars indicate the 5th and 95th percentiles.
ACT in relation to acid pH-impedance events and pH-only events.
The median ACT per acid pH-impedance events per subject was 234.8 (208.8) s and with pH-only events was 335.9 (624.6) s (p < 0.0001, Fig. 1B). Similarities was noted between patients with and without CLD for acid pH-impedance events [294.2 (221.5) versus 215.5 (191.2); p = 0.1] and pH-only events [364.0 (1076.1) versus 304.9 (512.8); p = 0.2].
Physicochemical property of refluxate proximal extent: supra-UES or infra-UES.
There were 1559 supra-UES and 410 infra-UES events. Liquid GER events were greater in infra-UES (versus supra-UES, p < 0.0001; Fig. 2A). Chemical composition of GER among the infra-UES was different (versus supra-UES, p < 0.0001; Fig. 2B) in that more ARE were seen when the maximal height was infra-UES and more NARE were seen when the maximal height was supra-UES.

Physicochemical composition of GER defined as supra-UES or infra-UES. In (A), significant difference is noted with the distribution of GER based on physical properties, infra- vs. supra-UES (*p < 0.0001). Mixed GER is represented in white, liquid in gray, and gas in black. In (B), significant difference is noted with the distribution of GER based on chemical properties, between infra- vs. supra-UES (*p < 0.0001). NARE and ARE are represented in white and black, respectively.
Prevalence of symptoms based on physicochemical characteristics.
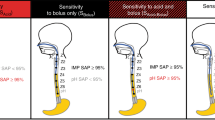
The distribution of the individual SI and SSI values is shown in Figure 3. In 6 patients (20%), the SI was >50%. An SSI of >10% was observed in 29 patients (96.7%). The highest SSI encountered was 95%. Discordance between the SI and SSI was observed in a substantial proportion of the patients (Fig. 3).

Distribution of SI and SSI. The dotted lines indicate the thresholds for the SSI (positive if >10%; horizontal line) and the SI (positive if >50%; vertical line). Note the discordance between the SI and the SSI in many patients.
Overall, 2146 symptoms were noted in 1031 pH-impedance events and 938 (47.7%) GER events were unassociated with symptoms. The SSI for composite symptoms per pH-impedance event (occurrence of any combination of symptoms per GER event) was 52.4% (1031/1969). Of the 94 pH-only events, 82 (87.3%) were associated with 249 symptoms. The SSI for composite symptoms per pH-only event was 87.3% (82/94). However, only 56.5% acid pH-impedance events were associated with symptoms (p < 0.0001 versus pH-only events).
We analyzed the relationship between the physicochemical characteristics of the pH-impedance events and symptoms (composite symptoms, respiratory symptoms, sensory symptoms, or physical symptoms; Table 2). The occurrence of symptoms with GER was similar among physical and chemical characteristics (all p = NS). However, the distribution of respiratory symptoms, sensory symptoms, and physical symptoms was different in relation to physical and chemical characteristics (Fig. 4). Gas GER events were associated with more sensory symptoms than liquid and mixed refluxate. Compared with nonacid GER, acid GER were associated with more physical symptoms and less sensory symptoms.

Symptom distribution based on physicochemical characteristics. In (A), symptom distribution based on physical properties: gas vs. liquid (*p < 0.0001); gas vs. mixed (§p = 0.0008); liquid vs. mixed (¶p = 0.05). In B), symptom distribution based on chemical properties: acid vs. nonacid (**p = 0.001). Respiratory, sensory, and movement symptoms are represented in white, gray, and black, respectively.
Of 7118 symptoms, only 2395 were associated with pH-impedance events or pH-only events. SI was calculated as 2395/7118 = 33.7%. The distribution of reflux associated movement-symptoms was greater (p = 0.04 versus sensory, p = 0.1 versus respiratory; Table 3). Similarly, whenever a symptom was present, the odds of having a liquid reflux event was 2-fold higher than the odds of having a gas reflux or a mixed reflux event.
Subgroup analysis did not show any difference among the group of patients with and without CLD in symptom distribution with pH-impedance events. Conversely, the occurrence of symptom-associated pH-only reflux events was higher with CLD patients compared with non-CLD patients, 94.3% versus 78.0%, (p = 0.03). Specifically, the odds of CLD patients having a pH-only events resulting in sensory symptoms was 3.6 times higher than the odds of non-CLD patients having a sensory symptom-associated pH-only events (p = 0.0001). Relationship between symptoms and physicochemical characteristics of pH-impedance events was similar between CLD and non-CLD.
Of the 1015 NARE, only 225 (22.2%) were associated with a change in pH by >1. The frequency of symptom-associated GER were similar regardless of the change in pH (>1 pH unit, 43.1% versus none, 50%, p = NS). However, only 19.7% of the symptomatic nonacid GER were associated with change in pH by >1.
Prevalence of symptoms based on spatiotemporal characteristics.
Of 1559 supra-UES GER, 821 were associated with a total of 1686 symptoms (SSI = 821/1559 = 52.7%); and of 410 infra-UES GER, 210 were associated with 460 symptoms (SSI = 210/410 = 51.3%). Whenever a symptom occurred, the odds of supra-UES GER (SI = 1686/7118 = 23.7%) was 3.6 times higher than the odds of infra-UES GER (SI = 460/7118 = 6.5%).
We next examined the relationship between symptom frequency and the duration of bolus and acid clearance. Symptomatic ARE, including both acid pH-impedance events and pH-only events, were associated with longer ACT (p = 0.001, Fig. 5A); similarly, the association between symptomatic pH-impedance events and longer BCT was also noted (p = 0.01, Fig. 5B).

Relationship of symptoms/reflux with esophageal ACT and BCT are shown in A (p < 0.0001 for association) and B (p = 0.01 for association), respectively.
The association between ACT and symptom frequency among patients with and without CLD was examined. Each ARE, including both acid pH-impedance events and pH-only events, was categorized based on symptoms. Prolonged ACT were associated with symptomatic AREs in CLD (all p < 0.05; Table 4); such association was absent in non-CLD (all p = NS; Table 4). Prolonged ACT was noted in CLD versus non-CLD for symptomatic AREs, (all p < 0.05; Table 4).
DISCUSSION
The definition of GERD in neonates/infants remains controversial and debates continue about the use and abuse of antireflux medical and surgical interventions (1,16). Given the complexity of refluxate composition and inability to distinguish symptoms due to physiological from pathological GER in the NICU infant, there is little recourse than to define GERD in an individualized setting. Establishing objective evidence of GER events and the relationship of symptoms with the physical or chemical composition of the refluxate is essential to characterize GERD.
Several important findings were observed with GER events in this study: 1) NARE are of equal frequency as ARE (17–19), and majority of events spread proximally above the UES; 2) average BCT was prolonged with mixed versus liquid, with supra-UES versus infra-UES; 3) ACT per acid pH-impedance event was lesser than pH-only events; 4) infra-UES GER was correlated with higher percentage of ARE compared with supra-UES GER, and supra-UES GER were associated with greater proportion of NARE; 5) 54% of GER events documented by pH-impedance were associated with symptoms, and more than 87% of the pH-only events were associated with symptoms; 6) the occurrence of symptoms was similar among different physicochemical characteristics, although the distribution of respiratory symptoms, sensory symptoms, and physical symptoms was different in relation to physicochemical characteristics; 7) subgroup analysis did not show any difference among the group of patients with and without CLD in symptom distribution, although the occurrence of symptom-associated pH-only reflux events was higher with CLD patients and that the sensory symptoms were greater in this group than non-CLD patients; 8) symptomatic ARE were associated with longer ACT; 9) prolonged acidity was associated with symptomatic ARE in CLD patients unlike non-CLD patients.
In this study, we categorized chemical GER events into ARE and NARE, as used before (8). We did not consider NARE to be synonymous with weakly alkaline reflux events, as we did not technically measure the degree of alkalinity (pH > 7).
It is clear from this study that symptoms can occur with varying physicochemical properties of refluxate or of its varying ascent. Some infants are more sensitive in reacting with symptoms (as in CLD) than others (without CLD). It is also clear why the management of GERD based on symptoms only is controversial, as there are “reflux-type symptoms” in the absence of GER. Management of GERD based on the frequency of GER is also controversial as a substantial proportion of GER were not associated with symptoms. Therefore, clinical trials based on symptom profiles only in neonates cannot offer definitive conclusions about GERD management. Similarly, clinical trials that have been based on the frequency of acid GER cannot offer definite conclusions about GERD management. The value of NARE and other background disease characteristics may have been ignored in such trials. Antireflux prophylactic medical therapies have been associated with necrotizing enterocolitis when given within the first weeks of life in premature infants, digestive problems, alteration of aerodigestive flora (20), abnormalities of calcium absorption, and osteopenia (3). Furthermore, aspirates of gastric juice in those treated with acid suppressants can be deleterious to the bronchial airway, and inflammatory reaction induced by bacteria and endotoxins have been reported in those CLD patients who were managed on proton pump inhibitors for GERD (21). Antireflux surgical therapies have been reported to be associated with early satiety, dyspepsia, and inability to vomit, fundoplication break-up, and GI dysmotility (3).
Interestingly, in our study, the prolonged acid clearance and its association with increased symptom frequency support the hypothesis that chemosensitive stimulation and prolonged dwell of the acid GER in the esophagus activates visceral, somatic, and sensory aerodigestive pathways resulting in the generation of symptoms (irritability and arching, grimace, cry, cough, gagging, stridor, physical movement, and so on). Indeed, all these symptoms involve nerve-muscle interaction at various levels, and these phenomena may support sensitization of esophageal afferents. Prolongation of ACT may be due to alteration of clearance mechanisms, esophageal dysmotility, or decreased acid neutralization or larger volume of refluxate. Furthermore, sensitization may be greater in CLD infants as the SSI was greater in these infants compared with those with non-CLD infants. It is still unclear as to the best choice of symptom indices (SI, SSI, and SAP) regardless of the age spectrum. In neonate, this association may be even more challenging owing to multiplicity of symptoms and nonverbal nature of subject. Future studies must address the complexity of neonatal symptoms and best predictors in relation to GERD. The discordance between the SI and SSI is noted, and this may be due to the chance of the SI being higher in the presence of many GER episodes and the SSI tends to be higher in the presence of many symptoms. From our study, useful conclusions can be drawn based on discordant indices, in that, the combination of a high SSI and a low SI indicates that the patient's esophagus is sensitive to reflux but causes other than reflux are likely to contribute to the symptoms (22,23). Although there were multiple symptoms belonging to different classifications, i.e. respiratory, sensory, or physical, a given symptom was counted only once to overcome the overlap. However, each symptom may have different sensory-motor basis for its occurrence. This study lends support to the activation of esophageal-airway reflexes in the genesis of symptoms. For example, in pH-only reflux events, where there was no ascending spread of the refluxate, the ACT was longer and SSI was of increased frequency. The reasons why pH-only events occur are not entirely clear and have been reported by others (12). Such events may happen because of swallow-related GER events, transient LES relaxation, or incomplete LES relaxation reflex. During such scenarios, activation of esophageal vagal afferents and airway and supra-UES efferents can result in aerodigestive defensive reflexes and symptoms, thus forming the basis for esophagoglottal closure and pharyngoglottal closure reflexes (24,25). These protective reflexes prevent the refluxate from reaching the airway.
This study also lends support to the association of symptoms not only with acid events but also with nonacid, gas, liquid, or mixed events. Esophageal clearance of a bolus depends on multiple factors involved with esophageal motility, i.e. sensory motor characteristics of the peristaltic reflexes (deglutition reflex response and secondary peristalsis), upper esophageal sphincter contractile reflex, and lower esophageal sphincter relaxation reflex (9,26). We have shown recently that the recruitment of esophageal and airway defensive reflexes increases with volume dependent provocation, chemosensitive stimulation, or graded volumes of esophageal distention. Thus, treatment strategies based on modification of gastric acidity alone can be ineffective as acid is not the lone provoking agent.
GER may therefore be an important comorbidity factor especially in NICU neonates (4,27). Although GER (physiologic form) may be more frequent in neonates, distinction from GERD (pathologic form) can be difficult. As such, there are no definite standards to aid in the diagnosis of GERD, or of symptom recognition, or with the management of GER among NICU neonates. Lack of clarity with diagnosis and therapeutic targets for neonatal GERD can lead to empiric therapies with resultant consequences (3). Recent Pediatric GERD guidelines from NASPGHAN/ESPGHAN offer little evidence on the evaluation and management of suspected GERD in neonates, and the expert committee recognized lack of quality evidence that supports a) the diagnosis of GERD, b) medical therapies, or c) life style changing surgical therapies (3).
In conclusion: 1) The current study is the first study to have attempted classification of the GER and symptom indices based on physicochemical and spatiotemporal attributes of the refluxate in neonates. 2) Given the complexity of the composition of refluxate in the definition of GERD, the relationship of symptoms versus the physicochemical composition of the refluxate is essential, so that therapeutic targets can be appropriate. 3) Infants with intractable CLD merit evaluation for alternate pathophysiology. 4) Locus of esophageal provocation may influence aerodigestive symptoms. 5) The occurrence of respiratory symptoms regardless of spatiotemporal distribution of refluxate suggests the activation of esophago airway and pharyngeal airway reflex interactions. 6) Clinical significance as measured by SSI and SI and characterization of spatial-temporal-physical-chemical nature of GER events as defined by pH-impedance methods clarifies the definition of GERD, i.e. GER with increased frequency of respiratory, sensory, or movement symptoms.
Abbreviations
- ACT:
-
acid clearance time
- ARE:
-
acid reflux event
- BCT:
-
bolus clearance time
- CLD:
-
chronic lung disease
- GER:
-
gastroesophageal reflux
- GERD:
-
gastroesophageal reflux disease
- LES:
-
lower esophageal sphincter
- NARE:
-
nonacid reflux event
- SI:
-
symptom index
- SSI:
-
symptom sensitivity index
- UES:
-
upper esophageal sphincter
References
Malcolm WF, Gantz M, Martin RJ, Goldstein RF, Goldberg RN, Cotten CM 2008 Use of medications for gastroesophageal reflux at discharge among extremely low birth weight infants. Pediatrics 121: 22–27
Barney CK, Baer VL, Scoffield SH, Lambert DK, Cook M, Christensen RD 2009 Lansoprazole, ranitidine, and metoclopramide: comparison of practice patterns at 4 level III NICUs within one healthcare system. Adv Neonatal Care 9: 129–131
Vandenplas Y, Rudolph CD, Di Lorenzo C, Hassall E, Liptak G, Mazur L, Sondheimer J, Staiano A, Thomson M, Veereman-Wauters G, Wenzl TG 2009 North American Society for Pediatric Gastroenterology Hepatology and Nutrition, European Society for Pediatric Gastroenterology Hepatology and Nutrition Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). J Pediatr Gastroenterol Nutr 49: 498–547
Jadcherla SR, Gupta A, Fernandez S, Nelin LD, Castile R, Gest AL, Welty S 2008 Spatiotemporal characteristics of acid refluxate and relationship to symptoms in premature and term infants with chronic lung disease. Am J Gastroenterol 103: 720–728
Vela MF, Camacho-Lobato L, Srinivasan R, Tutuian R, Katz PO, Castell DO 2001 Simultaneous intraesophageal impedance and pH measurement of acid and nonacid gastroesophageal reflux: effect of omeprazole. Gastroenterology 120: 1599–1606
American Gastroenterological Association 1996 American Gastroenterological Association medical position statement: guidelines on the use of esophageal pH recording. Gastroenterology 110: 1981
Jadcherla SR, Duong HQ, Hofmann C, Hoffmann R, Shaker R 2005 Characteristics of upper oesophageal sphincter and oesophageal body during maturation in healthy human neonates compared with adults. Neurogastroenterol Motil 17: 663–670
Gupta A, Jadcherla SR 2006 The relationship between somatic growth and in vivo esophageal segmental and sphincteric growth in human neonates. J Pediatr Gastroenterol Nutr 43: 35–41
Jadcherla SR, Hoffmann RG, Shaker R 2006 Effect of maturation of the magnitude of mechanosensitive and chemosensitive reflexes in the premature human esophagus. J Pediatr 149: 77–82
Jadcherla SR, Rudolph CD 2005 Gastroesophageal reflux in the preterm neonate. NeoReviews 6: e87–e98
Wenzl TG, Silny J, Schenke S, Peschgens T, Heimann G, Skopnik H 1999 Gastroesophageal reflux and respiratory phenomena in infants: status of the intraluminal impedance technique. J Pediatr Gastroenterol Nutr 28: 423–428
Rosen R, Nurko S 2004 The importance of multichannel intraluminal impedance in the evaluation of children with persistent respiratory symptoms. Am J Gastroenterol 99: 2452–2458
Zerbib F, des Varannes SB, Roman S, Pouderoux P, Artigue F, Chaput U, Mion F, Caillol F, Verin E, Bommelaer G, Ducrotte P, Galmiche JP, Sifrim D 2005 Normal values and day-to-day variability of 24-h ambulatory oesophageal impedance-pH monitoring in a Belgian-French cohort of healthy subjects. Aliment Pharmacol Ther 22: 1011–1021
Wiener GJ, Richter JE, Copper JB, Wu WC, Castell DO 1988 The symptom index: a clinically important parameter of ambulatory 24-hour esophageal pH monitoring. Am J Gastroenterol 83: 358–361
Lam HG, Breumelhof R, Roelofs JM, Van Berge Henegouwen GP, Smout AJ 1994 What is the optimal time window in symptom analysis of 24-hour esophageal pressure and pH data?. Dig Dis Sci 39: 402–409
Mousa H, Caniano DA, Alhajj M, Gibson L, Di Lorenzo C, Binkowitz L 2006 Effect of Nissen fundoplication on gastric motor and sensory functions. J Pediatr Gastroenterol Nutr 43: 185–189
Mousa H, Woodley FW, Metheney M, Hayes J 2005 Testing the association between gastroesophageal reflux and apnea in infants. J Pediatr Gastroenterol Nutr 41: 169–177
Condino AA, Sondheimer J, Pan Z, Gralla J, Perry D, O'Connor JA 2006 Evaluation of infantile acid and nonacid gastroesophageal reflux using combined pH monitoring and impedance measurement. J Pediatr Gastroenterol Nutr 42: 16–21
van Wijk MP, Benninga MA, Omari TI 2009 Role of the multichannel intraluminal impedance technique in infants and children. J Pediatr Gastroenterol Nutr 48: 2–12
Srinivasan R, Asselin J, Gildengorin G, Wiener-Kronish J, Flori HR 2009 A prospective study of ventilator-associated pneumonia in children. Pediatrics 123: 1108–1115
Mertens V, Blondeau K, Vanaudenaerde B, Vos R, Farre R, Pauwels A, Verleden G, Van Raemdonck D, Dupont L, Sifrim D 2010 Gastric juice from patients “on” acid suppressive therapy can still provoke a significant inflammatory reaction by human bronchial epithelial cells. J Clin Gastroenterol 44: e230–e235
Bredenoord AJ, Weusten BL, Smout AJ 2005 Symptom association analysis in ambulatory gastro-oesophageal reflux monitoring. Gut 54: 1810–1817
Sengupta JN 2001 Electrophysiological recording from neurons controlling sensory and motor functions of the esophagus. Am J Med 111: 169S–173S
Jadcherla SR, Gupta A, Coley BD, Fernandez S, Shaker R 2007 Esophago-glottal closure reflex in human infants: a novel reflex elicited with concurrent manometry and ultrasonography. Am J Gastroenterol 102: 2286–2293
Jadcherla SR, Gupta A, Wang M, Coley BD, Fernandez S, Shaker R 2009 Definition and implications of novel pharyngo-glottal reflex in human infants using concurrent manometry ultrasonography. Am J Gastroenterol 104: 2572–2582
Pena EM, Parks VN, Peng J, Fernandez SA, Di Lorenzo C, Shaker R, Jadcherla SR 2010 Lower esophageal sphincter relaxation reflex kinetics: effects of peristaltic reflexes and maturation in human premature neonates. Am J Physiol Gastrointest Liver Physiol 299: G1386–G1395
Jadcherla SR, Wang M, Vijayapal AS, Leuthner SR 2010 Impact of prematurity and co-morbidities on feeding milestones in neonates: a retrospective study. J Perinatol 30: 201–208
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported, in part, by Grant RO1 DK 068158 from the National Institutes of Health [S.R.J.].
Rights and permissions
About this article
Cite this article
Jadcherla, S., Peng, J., Chan, C. et al. Significance of Gastroesophageal Refluxate in Relation to Physical, Chemical, and Spatiotemporal Characteristics in Symptomatic Intensive Care Unit Neonates. Pediatr Res 70, 192–198 (2011). https://doi.org/10.1203/PDR.0b013e31821f704d
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/PDR.0b013e31821f704d
This article is cited by
-
Characteristics of esophageal refluxate and symptoms in infants compared between pre-treatment and on treatment with proton pump inhibitors
Journal of Perinatology (2024)
-
Differentiating esophageal sensitivity phenotypes using pH–impedance in intensive care unit infants referred for gastroesophageal reflux symptoms
Pediatric Research (2021)
-
Role of feeding strategy bundle with acid-suppressive therapy in infants with esophageal acid reflux exposure: a randomized controlled trial
Pediatric Research (2021)
-
Diagnostic utility of impedance-pH monitoring in infants of diabetic mothers with oral feeding difficulties
Journal of Perinatology (2021)
-
Prolonging gavage feeds for reduction of gastroesophageal reflux in infants
Journal of Perinatology (2020)
