
Abstract
It is now well established that IUGR is associated with an increased risk of a range of adult onset diseases, including cardiovascular disease, obesity, and type 2 diabetes. Infants from twin pregnancies are generally born smaller than singletons; therefore, it has been suggested that twins represent a naturally occurring model of IUGR. Although twin gestations contribute significantly to the population burden of preterm birth and small size at birth, whether twins have the same long-term health consequences as IUGR singletons remains unclear. The purpose of this review is to consider what is currently known about the clinical implications of twinning, the differences that exist between the growth and developmental profiles of singleton and twin fetuses, and to use this as a basis for exploring the question of whether fetuses conceived as twins are analogous to IUGR singletons of similar birthweight and gestation. This question is increasingly important in both the clinical and research settings, because the incidence of twinning is increasing and the long-term implications of reduced size at birth are mostly investigated in species which bear multiple offspring.
Similar content being viewed by others
Main
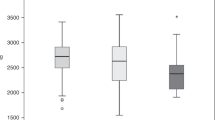
It is now well established that IUGR and being born small-for-GA (SGA) are associated with an increased risk of adult onset diseases; these include cardiovascular disease, obesity, and type 2 diabetes (1–3). In singletons, the risk of adult disease is inversely related to birthweight across the birthweight spectrum (2,3). Twins, as a population, are born lighter than singletons, with the normal distribution of birthweights for these infants shifted to the left of the normal singleton distribution (4,5) (Fig. 1). It has, therefore, been argued that twin pregnancies represent a natural model of IUGR (6). If this is the case, it would be expected that twins may be at increased risk for the long-term adverse health outcomes associated with reduced size at birth.

The birthweight distribution of twins (○) and singletons (•) in the United States in 1997 after excluding those with a birth weight <500 g or a GA <22 wk. Reprinted with permission from Joseph et al. Copyright © 2003 BioMed Central (http://www.biomedcentral.com/1471-2393/3/3).
Although the role of IUGR in increasing the risk of adult diseases has been extensively explored in singletons, the relationship between birthweight and the onset of adult diseases in those born as twins is unclear, with conflicting evidence in the literature (2). Most of the early twin studies did not include a singleton reference group, and more recent studies which have done so have shown increased adiposity and reduced insulin sensitivity in twins compared with singletons, and that these outcomes are related to size at birth (7,8). However, the number of studies that have addressed this is small, and the question remains as to whether the fact that twins tend to be smaller than singletons is due to the same type of environmental influences that cause IUGR in singletons (i.e. reduced placental transfer capacity), or whether there are inherent physiological differences between fetuses of singleton and twin pregnancies that are associated with distinct long-term outcomes in twins and singletons of comparable weight and GA at birth.
Normal and Abnormal Intrauterine Growth: Clarifying the Terminology
Preterm birth refers to birth before 37 completed weeks of gestation and this definition applies to all pregnancies, whether singleton or multiple. Term birth is between 37 and 41 completed weeks of gestation. Appropriate growth is expressed relative to GA to account for increasing size with advancing gestation. Thus, appropriate for GA babies have a birthweight between the 10th and 90th percentiles for the gestation at which they were born; small for GA (SGA) babies lie below the 10th percentile. Although the terms SGA, LBW, and IUGR are often used interchangeably, and many infants will fit more than one definition, the terms are not synonymous. LBW is used to describe any infant with a birthweight <2500 g, irrespective of GA; IUGR is a much more complex term describing infants who have failed to reach their intrauterine growth potential secondary to a pathological cause. IUGR is, therefore, a clinical diagnosis, which is made by examination of the baby after birth. In singleton pregnancies in developed countries, IUGR is usually the result of a deficit in placental transfer capacity due to placental dysfunction or maternal disease. These pathologies are not more common in twin pregnancies; thus, the increased risk of SGA and/or IUGR in twin pregnancies may be secondary to an alternative etiology.
Adverse Outcomes in Twin Pregnancies: A Clinical Perspective
Increasing incidence of twin pregnancies in developed countries.
The clinical importance of understanding more about the long-term health outcomes of twin fetuses is highlighted by data from developed countries demonstrating an increase in the incidence of twinning of between 28 and 59% over the past two decades (4,9–11). This increase has been linked largely to the increased utilization of artificial reproductive technologies (ART) and, to a lesser extent, the increase in mean maternal age over this period of time (9,10). In Australia, the average age of women having their first child in 2005 was 30.7 y, an increase of 3.4 y from 1985 (12), and similar increases have been reported in other developed countries (10). The increased incidence of twinning in older mothers is independent of the use of ART and seems to be the result of increased incidence of multiple ovulation in older women (13). Although there have been increases in both twin and higher order multifetal pregnancies, pregnancies with three or more fetuses make up only a very minor percentage of all births, and this review will focus predominately on twin pregnancies, which are more common and for which there have been more detailed studies on growth trajectories and postnatal outcomes.
Increased perinatal morbidity and mortality in twin pregnancies.
The increased incidence of twinning has important implications for neonatal care units, as it is well established that twins have an increased incidence of common neonatal problems (11). According to recent Australian figures, perinatal mortality rates are 21.5 per 1,000 births in twins, compared with 9.2 per 1,000 births in singletons (11). This higher perinatal mortality in twin pregnancies is largely due to the 6-fold higher incidence of preterm delivery (<33 wk' gestation) and increased incidence of LBW (<2500 g) and very LBW (<1500 g) in this infant population (9); however, even term deliveries of twins have higher rates of obstetric complications (14). In a large cohort study in Belgium, which included data from 12,021 singleton and 3,108 twin births that were naturally conceived reported that, in comparison to singleton births, twin birth had a significantly increased risk of preterm delivery [relative risk (RR), 6.88], LBW (RR, 8.58), and very LBW (RR, 7.29) when infants were matched for maternal age, parity, fetal sex, and year of birth (14). The increased incidence of preterm delivery and very LBW is of particular significance, because these infants often require intensive care in neonatal units and have a high risk of neonatal morbidity and poor long-term growth and developmental outcomes.
The Physiology of Fetal Growth in Twin Pregnancies
Differences in the growth trajectory between normal singleton and twin pregnancies.
In establishing whether twins are truly growth restricted with respect to their singleton counterparts, it is important to examine what is already known about their growth and developmental trajectory in utero and to compare this with that of normal and IUGR singleton fetuses.
How do the growth and developmental trajectory of twins compare with that of growth-restricted singletons?
IUGR in singleton pregnancies is most commonly detected in the second half of gestation. Numerous experimental paradigms have mimicked this by impairing placental function and thus nutrient delivery to the fetus in late gestation, resulting in a phenotype similar to that seen in human IUGR, with growth restriction, polycythemia, hypoglycemia, and hypoxemia (2). Examples include maternal heat stress, maternal undernutrition, uterine artery ligation, placental specific gene knock-out experiments, experimental restriction of placental growth, and placental embolization in a variety of species (15,16). In the majority of these experimental paradigms, the insult is applied in mid to late gestation, so that the growth trajectory of these fetuses diverges from normally grown singletons only in late gestation. This is also supported by data from the placental specific igf2 knockout in mice, in which placental growth potential is restriction before conception (17). In this model, placental transfer capacity is able to meet the nutritional requirements of the developing fetus until the third trimester of pregnancy, after which the growth trajectory slows compared with normally grown singletons (17). In the mouse igf2 P0 knockout, there is actually up-regulation of placental nutrient transfer which initially maintains fetal growth before the onset of growth failure (18).
The fetal growth trajectory of twins diverges from that of singletons much earlier in gestation than previously thought (around 8 wk in the human) (19–21), and a slower fetal growth persists in late gestation in both humans (20) and sheep (21,22). It was originally proposed that this reduced intrauterine growth was due to constraints imposed by uterine size and a restricted ability of the placenta to support the nutrient requirements for both fetuses in late gestation (23). However, it has since been demonstrated that the high compliance of the uterine wall means that physical constraint is unlikely to make any substantial contribution to fetal growth restraint (24). Similarly, limitations to placental supply do not seem to account for this early deviation in growth, because the growth trajectories of singletons and twins diverge much earlier than the time when nutrient delivery could be limiting factor.
These findings have led to the emerging paradigm that events in early gestation, perhaps as early as the time of conception, play a critical role in determining intrauterine growth trajectories and size at birth in twin gestations. Thus, the cause of the reduced growth in twins may have an origin distinct from that in growth-restricted singletons and this may have implications for the long-term effects. A caveat to this is the recent evidence demonstrating that, in singleton pregnancies, an observed fetal size in the first trimester that is less than expected is associated with an increased risk of SGA and preterm birth (25), and also the awareness that many placental vasculopathies, including preeclampsia, have their origin in early pregnancy.
Evidence for the importance of the early gestational environment for intrauterine growth in twin gestations: Studies of fetal reduction.
The earliest evidence that the growth trajectories of twin and singleton pregnancies was established in early gestation came from the unilateral fetectomy studies performed by Vatnick et al. (26). These studies showed that both placental weight and fetal body weight in late gestation in twins reduced to singletons at 50 d of gestation (term = ∼150 d gestation) were intermediate between those for naturally conceived singleton- and twin pregnant ewes (26). Furthermore, our own studies have demonstrated that after fetal reduction even earlier in an ovine pregnancy, measures of linear growth and gestation length after fetal reduction are reduced compared with those of singletons (Hancock and Bloomfield, unpublished data).
These results are in accordance with the observational outcomes of selective fetal reduction surgeries and spontaneous fetal reduction (i.e. abortion of one or more fetuses in the absence of surgical intervention) in humans, which both suggest that when a twin pregnancy is reduced to a singleton pregnancy in early gestation, the GA at delivery and the birthweight in the reduced singletons are still significantly lower than in normally grown singletons (27–31). Clearly, surgical fetal reduction in humans is not a random process, and if fetal position permits, there is selection of the smallest fetus for fetocide, which would tend to favor increased size of the remaining fetus, and the procedure itself may affect growth of the remaining twin. Similarly, spontaneous fetal reduction is more likely to occur in pregnancies in which there is some underlying pathology or complication, which may affect the growth of the remaining fetus(es). Nevertheless, these clinical observations are similar to findings in animal studies, which did include appropriate sham controls, and the fact that fetal reduction in early gestation does not completely restore fetal growth in either experimental animals or humans provides evidence that the growth trajectory of singleton and twin fetuses is not entirely due to reductions in nutrient availability in late gestation but is also influenced by factors present in the intrauterine environment in the early weeks of gestation, and long before nutrient supply would be expected to be limiting to fetal growth (32).
How does the developmental trajectory of twins compare with growth-restricted singletons?
In singletons, IUGR has been associated with an altered development of several key regulatory systems, including the hypothalamic-pituitary-adrenal (HPA) and glucose-insulin axes, and these alterations play a central role in determining the increased risk of metabolic and cardiovascular diseases in these infants later in life (2). Twin conception also results in altered timing of development of these axes compared with singleton pregnancies, although not necessarily in the same way as IUGR in singletons.
IUGR singletons have been reported to have increased cortisol concentrations in comparison with their normally grown counterparts, in both humans and large animal models. Cortisol concentrations are increased in the growth-restricted fetal sheep when compared with normally grown controls (33,34), and cordocentesis studies have also reported higher plasma cortisol concentrations in IUGR human fetuses at weeks 18–38 of gestation (35). The nature of HPA axis adaptations in twins seems to be quite different from that seen in growth-restricted singletons. In twin fetal sheep, basal cortisol and ACTH concentrations are lower than in singles (36,37) and these differences persist in response to acute stress (38). Furthermore, an exogenous ACTH challenge elicits a blunted fetal cortisol response in twins compared with singletons (37), whereas the adrenal responsiveness to an ACTH challenge in IUGR singletons is increased in comparison to normally grown singletons (34).
Differences are also seen in the development of the glucose-insulin axis in twin fetal sheep compared with IUGR singletons. In twins, pancreatic development in late gestation is advanced compared with singletons, as evidenced by their enhanced response to a glucose challenge in utero (37), and there are no differences in glucose tolerance between postpubertal twin and singleton lambs (39). IUGR in singletons, however, is associated with reduced β-cell mass and deficiencies in glucose-stimulated insulin secretion both before and after birth (40). The IUGR lamb exhibits enhanced whole-body insulin sensitivity of glucose metabolism and catch-up growth in early postnatal life when compared with normally grown singletons (41), and the abundance of insulin receptors in skeletal muscle is increased both before and after birth (42). This early phase of enhanced insulin sensitivity precedes the development of impaired insulin disposition in both basal and challenged states in IUGR adult males (43).
Periconceptional origins of fetal growth restriction in singletons and twins: Is there evidence that this leads to altered growth and developmental outcomes?
The data presented above suggest that the late gestation physiology of normally grown twins is different from that of the IUGR singleton fetus. This is perhaps not surprising if one considers that growth restriction in twins seems to be set early in gestation, rather than being the consequence of environmental stressors that emerge much later in gestation and interfere with the existing growth trajectory. There is also evidence from animal studies that a growth and developmental trajectory, which is set during the periconceptional period, can alter subsequent growth and developmental outcomes. The fetal adrenal seems to be particularly sensitive to insults in the periconceptional period. MacLaughlin et al. (44) showed that periconceptional undernutrition in the pregnant ewe results in altered relationships between adrenal growth and steroidogenic enzyme expression at 55–56 d gestation. Therefore, it seems that nutritional/endocrine signals to the developing embryo can have persistent effects on the development of key physiological systems. The effect of environmental insults on the development of the HPA are likely to be of particular importance in the context of long-standing observations that the adrenal gland is highly active during early gestation, after which it undergoes a period of quiescence until the prepartum activation, which is thought to be important for determining the timing of parturition (45,46).
This ability of the environment experienced by the embryo around the time of conception to influence developmental trajectories raises the question of whether there are specific signals, or combinations of signals, that sense the environment of the early embryo and determine the developmental trajectory of the fetus. Such signals seem to operate following periconceptional undernutrition to result in altered growth and development detectable months after the end of the period of nutritional restriction (36). Similar signals may be present in twin, but not singleton, pregnancies around the time of conception, placing the twin fetus on a different growth and developmental trajectory. In support of this, twins and singletons have been shown to exhibit different responses to maternal undernutrition during the periconceptional period (47). The nature of these signals is yet to be established, and this remains an important avenue for future research.
One possibility is epigenetic modification of the embryonic/fetal genome (48). Periconceptional undernutrition has been shown in a number of studies to result in altered methylation of the igf2/h19 promoter region in the fetal adrenal (49), liver (50), and hypothalamus (51), suggesting the early embryonic environment impacts on later epigenetic state in a range of fetal tissues. The potential role of epigenetic modifications in twin pregnancies in explaining the different intrauterine growth and developmental profiles of twin and singleton fetuses has been highlighted by a recent study (Stevens, Challis, Bloomfield, and White, unpublished data) demonstrating altered methylation and histone acetylation in the arcuate nucleus of the hypothalamus in twin fetuses compared with singletons. This suggests that similar epigenetic changes may also be present in tissues that play an important role in fetal growth. Epigenetic modifications in the igf2/h19 promoter are associated with altered fetal growth (52); however, whether altered methylation or histone acetylation within this, or other, loci contributes to the altered gestational growth profile in twin fetuses remains unknown and represents an important question for future research.
What Is the Evidence for Adverse Outcome in Twin Pregnancies Compared With IUGR Singletons?
If it is the case that there are periconceptional origins of altered growth and development in twins compared with singletons, the questions that need to be addressed next are the following: (1) do these early developmental changes have long-term implications and (2) are the outcomes likely to be different to those in singletons, in which IUGR typically results from placental or nutritional deficiencies which arise later in gestation?
Is there a role of birthweight in defining long-term health outcomes in twin pregnancies?
In twins, there is conflicting evidence regarding the association between birthweight, postnatal growth, and an increased risk of metabolic diseases in adulthood, including obesity, type 2 diabetes, and cardiovascular disease (53), associations that are now well established in singletons (2). Most of the evidence in twins comes from classical twin studies, in which the relationships between health or physiological outcomes and birthweight are compared between monozygotic and dizygotic twin pairs, thereby theoretically controlling for genotype (54,55). More recent data, however, suggest that this approach may be too simplistic, as it is now evident that both twins of a twin pair, whether mono- or dizygotic, are subject to the influences that subtle differences in the intrauterine environment impose on the fetal developmental trajectory (53,56). Thus, traditional twin studies are likely to underestimate the effect of the intrauterine environment, as both types of twinning will be affected. More recent studies have taken this into account by making use of regression analyses that incorporate both a between-twin coefficient (accounting for the contribution of shared maternal factors, such as nutritional status and socioeconomic status) and a within-twin pair coefficient (accounting for individual fetal factors, such as individual nutrition, metabolic, or hormonal status) to provide more information on the role of the intrauterine environment (57–59). There have been limited studies that have compared the long-term health outcomes within a twin pair; therefore, it is not clear whether the twin of lower birthweight has poorer health outcomes than the heavier twin in the pair, and it may well be that both twins are in fact equally affected.
Similarly, two recent studies in large animal models have provided conflicting data on the effect of LBW due to twinning on blood pressure in postnatal life. Ross et al. (60) found that twins had significantly greater systolic, diastolic, and mean arterial pressures compared with singleton lambs at 21 d of age. There was some concern that this result may have been confounded by the fact that the animals were dehydrated during the blood pressure measurements, and a comparable study by De Matteo et al. (61), in which blood pressure was assessed in the hydrated state, found no differences between blood pressure in twins and singletons at 8 wk of age. Furthermore, within-twin pair analysis in this study showed that there was no significant difference in current weight or in mean arterial pressures between twins that had been heavier or lighter at birth (61). In contrast, HPA axis activity in young adult twin sheep is increased compared with singleton controls and is also inversely associated with the within-twin coefficient for birthweight, suggesting an association with fetal growth (39). Thus, further studies in species that bear singleton and multiple offspring will be required to adequately address the relationships between long-term physiological outcomes that may impact on disease risk and birthweight/fetal growth in twins, in particular, studies that directly compare postnatal outcomes in IUGR singletons and normally grown twins.
Implications of the Developmental Differences Between Singletons and Twins for Research Into the Developmental Origins of Adult Disease
Despite the controversy about the potential differences that may or may not exist between twins and singletons, the use of multiple pregnancies as a means of generating IUGR offspring in both small and large animals has been used relatively widely to study the developmental origins of adult health outcomes. In these studies, it is relatively common to see twins defined as “spontaneous” or “natural” forms of growth restriction, and some studies have grouped together multiple births and singletons which fall within the accepted definition of IUGR (62–65). These studies have argued that growth restriction per se (defined by birthweight), independent of its origin, is the principal determinant of fetal programming (62).
In litter-bearing species, such as the guinea pig, rat, and pig, natural variations in birthweight between litter mates have commonly been used to study differences between low-birthweight and high-birthweight individuals (66–68). In the pig studies, Poore and Fowden (67,68) demonstrated that LBW pigs exhibited accelerated (catch-up) growth in the immediate postnatal period, as well as impaired glucose tolerance, insulin sensitivity, and cardiovascular and endocrine function in adolescence and adulthood compared with their high-birthweight counterparts. In the sheep, a principally monotocous species, ewes have been selectively bred to bear 4–5 lambs with a range of birthweights, and the LBW lambs born to these ewes exhibit postnatal hyperphagia and accelerated growth, increased adipose tissue deposition, and reduced muscle mass when compared with their higher birthweight counterparts (64,69,70). These studies therefore seem to provide evidence that growth restriction induced as a consequence of the presence of multiple fetuses within the same uterus is associated with the same profile of postnatal outcomes as reported in growth-restricted singletons.
However, the question of whether fetuses of polytocous species are resistant to developmental adaptations in response to additional (or fewer) fetuses has not been addressed. It is, of course, impossible to have singleton controls in litter-bearing species; studies in which species have singleton and twin pregnancies, such as the human and the sheep, are necessary to separate out the effects of singleton versus multiple conceptions.
Summary and Conclusions
This review has drawn on data from clinical and experimental animal studies to focus on the question of whether twins are analogous to IUGR singletons in their intrauterine growth and long-term health outcomes. Although there is clear evidence that the trajectory of fetal growth and development of key regulatory systems including the HPA and glucose-insulin axis in utero is different in twins compared with IUGR singletons, whether small twins have the same long-term health outcomes as IUGR singletons of comparable weight and gestation remains unclear. Experimental animal studies of the smallest offspring of litter-bearing species have reported similar physiological outcomes in these spontaneously growth-restricted offspring compared with those reported for IUGR singletons. However, it seems likely that the smallest of these higher order multiples develop in a significantly compromised intrauterine environment that is different to that experienced by the healthy twin fetus.
In humans, the ability to assess whether twins have similar long-term outcomes as IUGR singletons has no doubt been confounded by the high rate of preterm births in this infant population since preterm delivery is associated with its own set of long-term health issues. There are currently few data on the long-term metabolic and cardiovascular consequences of preterm birth, and it is difficult to separate the effect of preterm birth from reduced size at birth.
It is, therefore, clear that more clinical studies that examine the outcomes of IUGR in twins born at term and studies in predominately singleton and twin-bearing animal species that directly compare the postnatal outcomes of twins and IUGR singletons are required to understand fully the long-term implications of twinning.
Abbreviations
- HPA:
-
hypothalamic-pituitary-adrenal
- SGA:
-
small for GA
References
Gardosi J 2004 Customized fetal growth standards: rationale and clinical application. Semin Perinatol 28: 33–40
McMillen IC, Robinson JS 2005 Developmental origins of the metabolic syndrome: prediction, plasticity, and programming. Physiol Rev 85: 571–633
Barker DJ 1992 Fetal growth and adult disease. Br J Obstet Gynaecol 99: 275–276
Alexander GR, Kogan M, Martin J, Papiernik E 1998 What are the fetal growth patterns of singletons, twins, and triplets in the United States?. Clin Obstet Gynecol 41: 114–125
Joseph K, Liu S, Demissie K, Wen SW, Platt RW, Ananth CV, Dzakpasu S, Sauve R, Allen AC, Kramer MS, The Fetal and Infant Health Study Group of the Canadian Perinatal Surveillance System 2003 A parsimonious explanation for intersecting perinatal mortality curves: understanding the effect of plurality and of parity. BMC Pregnancy Childbirth 3: 3
Blickstein I 2005 Growth aberration in multiple pregnancy. Obstet Gynecol Clin North Am 32: 39–54
Poulsen P, Grunnet LG, Pilgaard K, Storgaard H, Alibegovic A, Sonne MP, Carstensen B, Beck-Nielsen H, Vaag A 2009 Increased risk of type 2 diabetes in elderly twins. Diabetes 58: 1350–1355
Monrad RN, Grunnet LG, Rasmussen EL, Malis C, Vaag A, Poulsen P 2009 Age-dependent nongenetic influences of birth weight and adult body fat on insulin sensitivity in twins. J Clin Endocrinol Metab 94: 2394–2399
Blondel B, Kogan MD, Alexander GR, Dattani N, Kramer MS, Macfarlane A, Wen SW 2002 The impact of the increasing number of multiple births on the rates of preterm birth and low birthweight: an international study. Am J Public Health 92: 1323–1330
Martin JA, Hamilton BE, Ventura SJ, Menacker F, Park MM, Sutton PD 2002 Births: final data for 2001. Natl Vital Stat Rep 51: 1–102
Umstad MP, Gronow MJ 2003 Multiple pregnancy: a modern epidemic?. Med J Aust 178: 613–615
Laws P, Hilder L 2008 Australia's mothers and babies 2006. 2008 AIHW National Perinatal Statistics Unit, Sydney. Available at: http://www.npsu.unsw.edu.au/PRERUWeb.nsf/resources/AMB_2008/$file/ps22.pdf. Accessed March 8, 2011
Beemsterboer SN, Homburg R, Gorter NA, Schats R, Hompes PG, Lambalk CB 2006 The paradox of declining fertility but increasing twinning rates with advancing maternal age. Hum Reprod 21: 1531–1532
Ombelet W, Martens G, De Sutter P, Gerris J, Bosmans E, Ruyssinck G, Defoort P, Molenberghs G, Gyselaers W 2006 Perinatal outcome of 12,021 singleton and 3108 twin births after non-IVF-assisted reproduction: a cohort study. Hum Reprod 21: 1025–1032
Morrison JL 2008 Sheep models of intrauterine growth restriction: fetal adaptations and consequences. Clin Exp Pharmacol Physiol 35: 730–743
Robinson JS, Falconer J, Owens JA 1985 Intrauterine growth retardation: clinical and experimental. Acta Paediatr Scand Suppl 319: 135–142
Constância M, Hemberger M, Hughes J, Dean W, Ferguson-Smith A, Fundele R, Stewart F, Kelsey G, Fowden A, Sibley C, Reik W 2002 Placental-specific IGF-II is a major modulator of placental and fetal growth. Nature 417: 945–948
Constância M, Angiolini E, Sandovici I, Smith P, Smith R, Kelsey G, Dean W, Ferguson-Smith A, Sibley CP, Reik W, Fowden A 2005 Adaptation of nutrient supply to fetal demand in the mouse involves interaction between the IGF2 gene and placental transporter systems. Proc Natl Acad Sci USA 102: 19219–19224
Leveno KJ, Santos-Ramos R, Duenhoelter JH, Reisch JS, Whalley PJ 1979 Sonar cephalometry in twins: a table of biparietal diameters for normal twin fetuses and a comparison with singletons. Am J Obstet Gynecol 135: 727–730
Iffy L, Lavenhar MA, Jakobovits A, Kaminetzky HA 1983 The rate of early intrauterine growth in twin gestation. Am J Obstet Gynecol 146: 970–972
Rattray PV, Garrett WN, East NE, Hinman N 1974 Growth, development and composition of the ovine conceptus and mammary gland during pregnancy. J Anim Sci 38: 613–626
Koong LJ, Garrett WN, Rattray PV 1975 A description of the dynamics of fetal growth in sheep. J Anim Sci 41: 1065–1068
Bleker OP, Wolf H, Oosting J 1995 The placental cause of fetal growth retardation in twin gestations. Acta Genet Med Gemellol (Roma) 44: 103–106
Westwood M, Gibson JM, Sooranna SR, Ward S, Neilson JP, Bajoria R 2001 Genes or placenta as modulator of fetal growth: evidence from the insulin-like growth factor axis in twins with discordant growth. Mol Hum Reprod 7: 387–395
Bukowski R, Smith GC, Malone FD, Ball RH, Nyberg DA, Comstock CH, Hankins GD, Berkowitz RL, Gross SJ, Dugoff L, Craigo SD, Timor-Tritsch IE, Carr SR, Wolfe HM, D'Alton ME 2007 Fetal growth in early pregnancy and risk of delivering low birth weight infant: prospective cohort study. BMJ 334: 836–840
Vatnick I, Schoknecht PA, Darringrand R, Bell AW 1991 Growth and metabolism of the placenta after unilateral fetectomy in twin pregnant ewes. J Dev Physiol 15: 351–356
Brambati B, Tului L, Camurri L, Guercilena S 2004 First-trimester fetal reduction to a singleton infant or twins: outcome in relation to the final number and karyotyping before reduction by transabdominal chorionic villus sampling. Am J Obstet Gynecol 191: 2035–2040
Alexander JM, Hammond KR, Steinkampf MP 1995 Multifetal reduction of high-order multiple pregnancy: comparison of obstetrical outcome with nonreduced twin gestations. Fertil Steril 64: 1201–1203
Depp R, Macones GA, Rosenn MF, Turzo E, Wapner RJ, Weinblatt VJ 1996 Multifetal pregnancy reduction: evaluation of fetal growth in the remaining twins. Am J Obstet Gynecol 174: 1233–1238
Groutz A, Yovel I, Amit A, Yaron Y, Azem F, Lessing JB 1996 Pregnancy outcome after multifetal pregnancy reduction to twins compared with spontaneously conceived twins. Hum Reprod 11: 1334–1336
Pinborg A, Lidegaard O, la Cour Freiesleben N, Andersen AN 2005 Consequences of vanishing twins in ivf/icsi pregnancies. Hum Reprod 20: 2821–2829
Harding JE, Johnston BM 1995 Nutrition and fetal growth. Reprod Fertil Dev 7: 539–547
Simonetta G, Rourke AK, Owens JA, Robinson JS, McMillen IC 1997 Impact of placental restriction on the development of the sympathoadrenal system. Pediatr Res 42: 805–811
Phillips ID, Simonetta G, Owens JA, Robinson JS, Clarke IJ, McMillen IC 1996 Placental restriction alters the functional development of the pituitary-adrenal axis in the sheep fetus during late gestation. Pediatr Res 40: 861–866
Economides DL, Nicolaides KH, Linton EA, Perry LA, Chard T 1988 Plasma cortisol and adrenocorticotropin in appropriate and small for gestational age fetuses. Fetal Ther 3: 158–164
Edwards LJ, McMillen IC 2002 Impact of maternal undernutrition during the periconceptional period, fetal number, and fetal sex on the development of the hypothalamo-pituitary adrenal axis in sheep during late gestation. Biol Reprod 66: 1562–1569
Rumball CW, Harding JE, Oliver MH, Bloomfield FH 2008 Effects of twin pregnancy and periconceptional undernutrition on maternal metabolism, fetal growth and glucose-insulin axis function in ovine pregnancy. J Physiol 586: 1399–1411
Gardner DS, Jamall E, Fletcher AJ, Fowden AL, Giussani DA 2004 Adrenocortical responsiveness is blunted in twin relative to singleton ovine fetuses. J Physiol 557: 1021–1032
Bloomfield FH, Oliver MH, Harding JE 2007 Effects of twinning, birth size, and postnatal growth on glucose tolerance and hypothalamic-pituitary-adrenal function in postpubertal sheep. Am J Physiol Endocrinol Metab 292: E231–E237
Green AS, Rozance PJ, Limesand SW 2010 Consequences of a compromised intrauterine environment on islet function. J Endocrinol 205: 211–224
De Blasio MJ, Gatford KL, Robinson JS, Owens JA 2007 Placental restriction of fetal growth reduces size at birth and alters postnatal growth, feeding activity, and adiposity in the young lamb. Am J Physiol Regul Integr Comp Physiol 292: R875–R886
Muhlhausler BS, Duffield JA, Ozanne SE, Pilgrim C, Turner N, Morrison JL, McMillen IC 2009 The transition from fetal growth restriction to accelerated postnatal growth: a potential role for insulin signalling in skeletal muscle. J Physiol 587: 4199–4211
Gatford KL, Mohammad SN, Harland ML, De Blasio MJ, Fowden AL, Robinson JS, Owens JA 2008 Impaired {beta}-cell function and inadequate compensatory increases in {beta}-cell mass after intrauterine growth restriction in sheep. Endocrinology 149: 5118–5127
MacLaughlin SM, Walker SK, Kleemann DO, Sibbons JP, Tosh DN, Gentili S, Coulter CL, McMillen IC 2007 Impact of periconceptional undernutrition on adrenal growth and adrenal insulin-like growth factor and steroidogenic enzyme expression in the sheep fetus during early pregnancy. Endocrinology 148: 1911–1920
Wintour EM, Brown EH, Denton DA, Hardy KJ, McDougall JG, Oddie CJ, Whipp GT 1975 The ontogeny and regulation of corticosteroid secretion by the ovine foetal adrenal. Acta Endocrinol (Copenh) 79: 301–316
McMillen IC, Phillips ID, Ross JT, Robinson JS, Owens JA 1995 Chronic stress- the key to partutition?. Reprod Fertil Dev 7: 499–507
MacLaughlin SM, Walker SK, Roberts CT, Kleemann DO, McMillen IC 2005 Periconceptional nutrition and the relationship between maternal body weight changes in the periconceptional period and feto-placental growth in the sheep. J Physiol 565: 111–124
Joss-Moore LA, Lane RH 2009 The developmental origins of adult disease. Curr Opin Pediatr 21: 230–234
Zhang S, Rattanatray L, MacLaughlin SM, Cropley JE, Suter CM, Molloy L, Kleemann D, Walker SK, Muhlhausler BS, Morrison JL, McMillen IC 2010 Periconceptional undernutrition in normal and overweight ewes leads to increased adrenal growth and epigenetic changes in adrenal IGF2/H19 gene in offspring. FASEB J 24: 2772–2782
Gong L, Pan YX, Chen H 2010 Gestational low protein diet in the rat mediates IGF2 gene expression in male offspring via altered hepatic DNA methylation. Epigenetics 5: 619–626
Stevens A, Begum G, Cook A, Connor K, Rumball C, Oliver M, Challis J, Bloomfield F, White A 2010 Epigenetic changes in the hypothalamic proopiomelanocortin and glucocorticoid receptor genes in the ovine fetus after periconceptional undernutrition. Endocrinology 151: 3652–3664
Zeisel SH 2009 Epigenetic mechanisms for nutrition determinants of later health outcomes. Am J Clin Nutr 89: 1488S–1493S
Phillips DI, Davies MJ, Robinson JS 2001 Fetal growth and the fetal origins hypothesis in twins–problems and perspectives. Twin Res 4: 327–331
Baird J, Osmond C, MacGregor A, Snieder H, Hales CN, Phillips DI 2001 Testing the fetal origins hypothesis in twins: the birmingham twin study. Diabetologia 44: 33–39
Vågerö D, Leon D 1994 Ischaemic heart disease and low birth weight: a test of the fetal-origins hypothesis from the swedish twin registry. Lancet 343: 260–263
Morley R, Dwyer T 2005 Studies of twins: what can they tell us about the fetal origins of adult disease?. Paediatr Perinat Epidemiol 19: 2–7
Vaag A, Poulsen P 2007 Twins in metabolic and diabetes research: what do they tell us?. Curr Opin Clin Nutr Metab Care 10: 591–596
Poulsen P, Esteller M, Vaag A, Fraga MF 2007 The epigenetic basis of twin discordance in age-related diseases. Pediatr Res 61: 38R–42R
Carlin JB, Gurrin LC, Sterne JA, Morley R, Dwyer T 2005 Regression models for twin studies: a critical review. Int J Epidemiol 34: 1089–1099
Ross MG, Desai M, Guerra C, Wang S 2005 Programmed syndrome of hypernatremic hypertension in ovine twin lambs. Am J Obstet Gynecol 192: 1196–1204
De Matteo R, Stacy V, Probyn M, Desai M, Ross M, Harding R 2008 The perinatal development of arterial pressure in sheep: effects of low birth weight due to twinning. Reprod Sci 15: 66–74
Louey S, Cock ML, Harding R 2005 Long term consequences of low birthweight on postnatal growth, adiposity and brain weight at maturity in sheep. J Reprod Dev 51: 59–68
Muhlhausler BS, Ritorto V, Schultz C, Chatterton BE, Duffield JA, McMillen IC 2008 Birth weight and gender determine expression of adipogenic, lipogenic and adipokine genes in perirenal adipose tissue in the young adult sheep. Domest Anim Endocrinol 35: 46–57
Greenwood PL, Hunt AS, Hermanson JW, Bell AW 1998 Effects of birth weight and postnatal nutrition on neonatal sheep: I. Body growth and composition, and some aspects of energetic efficiency. J Anim Sci 76: 2354–2367
Greenwood PL, Hunt AS, Slepetis RM, Finnerty KD, Alston C, Beermann DH, Bell AW 2002 Effects of birth weight and postnatal nutrition on neonatal sheep: III. Regulation of energy metabolism. J Anim Sci 80: 2850–2861
Schröder HJ 2003 Models of fetal growth restriction. Eur J Obstet Gynecol Reprod Biol 110: S29–S39
Poore KR, Fowden AL 2004 The effects of birth weight and postnatal growth patterns on fat depth and plasma leptin concentrations in juvenile and adult pigs. J Physiol 558: 295–304
Poore KR, Fowden AL 2004 Insulin sensitivity in juvenile and adult large white pigs of low and high birthweight. Diabetologia 47: 340–348
Greenwood PL, Hunt AS, Hermnanson JW, Bell AW 2000 Effects of birth weight and postnatal nutrition on neonatal sheep: II. Skeletal muscle growth and development. J Anim Sci 78: 50–61
Greenwood PL, Hunt AS, Bell AW 2004 Effects of birth weight and postnatal nutrition on neonatal sheep: IV. Organ growth. J Anim Sci 82: 422–428
Acknowledgements
The authors wish to acknowledge John Carragher for editorial assistance.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by fellowships from the National Health and Medical Research Council of Australia (NHMRC) [B.M. and R.H.].
Rights and permissions
About this article
Cite this article
Muhlhausler, B., Hancock, S., Bloomfield, F. et al. Are Twins Growth Restricted?. Pediatr Res 70, 117–122 (2011). https://doi.org/10.1203/PDR.0b013e31821f6cfd
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/PDR.0b013e31821f6cfd
This article is cited by
-
High Maternal Serum Estradiol in First Trimester of Multiple Pregnancy Contributes to Small for Gestational Age via DNMT1-Mediated CDKN1C Upregulation
Reproductive Sciences (2022)
-
Twin discordance: a study of volumetric fetal brain MRI and neurodevelopmental outcome
European Radiology (2021)
-
Associations Between Fetal Growth and Self-Perceived Health Throughout Adulthood: A Co-twin Control Study
Behavior Genetics (2016)
-
Epigenetic modifications may play a role in the developmental consequences of early life events
Journal of Neurodevelopmental Disorders (2011)
