
Abstract
We recently reported that hypoxic-ischemic (HI) insult to the brain of 7-d-old rats resulted in a slowly progressive learning and memory disability, which started at around 5 wk after HI, a time frame that is representative of human adolescence. The purpose of the present study was to examine whether physical or mental exercises can prevent this late-onset, slowly progressing disability. Wistar rats were subjected to left carotid ligation followed by 2 h of hypoxic stress (8% O2 and 92% N2 at 33°C). Sham-control rats were subjected to the same procedure without ligation and hypoxic stress. Six weeks after the HI, the animals were divided into four groups: pretraining control, no training control, pretraining HI, and no training HI groups. We used the plus maze, eight-arm radial maze, and choice reaction time task as the rehabilitative training. Sixteen weeks after the HI, the water maze task was performed over 5 d to evaluate spatial learning ability; thereafter, cerebral morphology of the animals was examined. There were no differences in swimming length and latency between the pretraining control and no training control groups. Swimming length and latency in the pretraining HI group were significantly shorter and swifter than those in the no training HI group. The infarct areas on the left cerebral hemisphere were equivalent between pretraining HI and no training HI groups at each sectional slice. Rehabilitative training tasks prevented the neonatal HI-induced late-onset slowly progressive learning and memory disability.
Similar content being viewed by others

Main
Neonatal HI encephalopathy causes learning and memory disability in childhood as well as cerebral palsy and epilepsy. The Rice et al. (1) model for neonatal HI encephalopathy in the rat has been widely used to study the long-lasting behavioral changes in learning and memory tasks after HI (2,3) because it is the only animal model that enables us to study long-term effects (4). We have previously performed extended observations up to 18 wk after HI stress and found characteristic impairments of three different steps of the memory process: attention, short-term working memory, and long-term reference memory (2).
Recently, in a long-term serial observation study, using the same neonatal rat HI model combined with magnetic resonance imaging, we discovered a characteristic phenomenon, termed late-onset slowly progressive brain damage (5). The ipsilateral hemispheric infarct volume slowly increased from 5 wk after HI stress. Compensatory hypertrophy of the contralateral cerebral hemisphere was observed only until 5 wk after HI; thereafter, the volume of the contralateral hemi-sphere also slowly diminished. These late-onset progressive morphologic changes were accompanied by progressive aggravation of learning and memory disabilities. Specifically, spatial learning disability in eight-arm radial maze tasks performed at 16 wk after HI was more pronounced than the disability at 7 wk after HI. These findings indicate that, in terms of learning and memory disability, perinatal HI-induced damage is not a stable disorder but a disorder that slowly progresses in later stages of life, such as around adolescence (5–7 wk of age in a rat's life span). From a therapeutic perspective, certain therapeutic modalities might be available, even in this later stage of life, to prevent further progression of the disability.
Physical or mental exercises, such as early handling in the neonatal period (6,7), environment enrichment (8,9), or rehabilitative manipulation (10), have all been demonstrated to improve learning and memory disability caused by HI or ischemic insult in rats. Until now, the efficacy of these interventions, with the intention of relieving a developmentally associated disorder, have been evaluated in laboratory animals in the early neonatal or adult periods, but have not been examined in adolescence. The purpose of this study was to examine whether physical and mental exercises, performed as a rehabilitation training program, could prevent the late-onset slowly progressive learning and memory disability that originated from neonatal HI insult.
MATERIALS AND METHODS
Animals.
This study was approved by the Experimental Animal Care and Use Committee at Miyazaki Medical College. Seventeen pregnant Wistar rats were purchased from a regional vendor (Japan Charles River, Atsugi, Japan). After they gave birth, we used 62 7-d-old rats. Newborn animals with body weights outside of the range determined by our nomogram were excluded.
Experimental protocol.
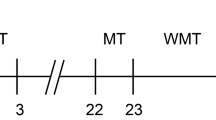
According to the presence or absence of HI stress, Wistar rats were grouped into sham control and HI groups. According to the presence or absence of rehabilitative training tasks, those groups were further subgrouped into pretraining and no training groups (Fig. 1). Therefore, we assigned four groups: pretraining control group (n = 15, male/female = 8/7), no training control group (n = 16, 6/10), pretraining HI group (n = 15, 9/6), and no training HI group (n = 16, 8/8).

Experimental schedule. Time points represent weeks after HI insult. Animal number: pretraining control group (n = 15, male/female = 8/7), no training control group (n = 16, 6/10), pretraining HI group (n = 15, 9/6), and no training HI group (n = 16, 8/8).
Hypoxic-ischemic insult at postnatal d 7.
HI groups were subjected to a modified Rice-Vannucci procedure to produce HI injury (1,2) Briefly, pups were anesthetized with ether and the left carotid artery was sectioned between double ligatures that were effected using 4-0 surgical silk. The pups were allowed to recover for 1–2 h and then exposed to 2 h of hypoxia in a plastic container that was perfused with a mixture of humidified 8% oxygen balanced with nitrogen. The temperature inside the container was kept at 33°C, which is the usual temperature to which rat pups are exposed when huddling with their mother (11). In the sham control group, each pup was treated the same as in the HI group, except for carotid artery ligation and hypoxia.
Rehabilitative training tasks.
Six weeks after the HI, the rehabilitative training tasks were started in the pretraining control and pretraining HI groups. These tasks consisted of the plus maze, eight-arm radial maze, and choice reaction time (CRT) task in that order. The detailed procedure is described elsewhere (2). All rats were housed in groups of four or five per cage from the fourth week after the HI and were placed under restricted food intake (10 g/d, CE-2, Crea Japan, Tokyo, Japan) for the eight-arm radial maze and CRT tasks. This fasting was done from wk 6 to wk 15 after the HI. The no training control and no training HI groups also received this food restriction. All rats had free access to water throughout the experimental period.
Water maze.
The swimming pool (Neuroscience Inc.) was a circular water tank, 150 cm in diameter and 45 cm deep, which was modified as described by Morris (12). It was filled to a depth of 34 cm with water at 23 ± 2°C. A platform, 12 cm in diameter and 32 cm high, was present inside the tank so that its top surface was 2 cm below the surface of the water. The pool was located in a large test room and surrounded by many cues external to the maze (e.g. the experimenter, ceiling lights, rack), which were visible from within the pool and could be used by the rat for spatial orientation. The positions of the cues were not changed throughout the period of testing. A CCD camera was connected to a personal computer for behavioral analysis (AXIS-30, Neuroscience Inc.).
Each rat underwent three trials daily for five consecutive days. A trial consisted of placing a rat by hand into the water facing the wall of the pool, at one of three starting positions, excluding the quadrant that contained the platform, which divided the pool into quadrants (north-N, south-S, east-E, or west-W). The platform was located in a constant position in the middle of one quadrant. During each block of three trials, each rat started at each of the three starting positions, but the sequence of the positions was selected randomly. In each trial, the latency (swimming time) to escape onto the hidden platform was recorded, with a cutoff time of 120 s. If a rat found the platform, it was permitted to remain there for 30 s. If a rat failed to find the platform within 120 s, it was placed on the platform and forced to remain there for 30 s. At the end of a trial, the rat was returned to its home cage. The intertrial interval was approximately 1 min. Performance in each trial was assessed according to three parameters: swimming time, swimming distance, and swimming speed.
Quantitative histologic analysis.
After all the experiments were complete, the animals were anesthetized with pentobarbital (50 mg/kg, i.p.) and perfused transcardially with saline followed by 4% paraformaldehyde. Brains were removed and sectioned coronally into 2-mm slices using a rat brain slicer. We then measured the area (mm2) of the contralateral and ipsilateral hemispheres in each brain section (4, 6, 8, 10, and 12 mm from the anterior pole of the cerebrum) using NIH Image software (version 1.62).
Statistics.
Results are expressed as means ± SEM. Repeated-measures two-way analysis of variance (ANOVA) was also used to evaluate the results of the water maze, followed by Tukey's test for post hoc analysis. Tukey's test after one-way ANOVA was used for comparison between average of result and for quantitative histologic analysis. A p < 0.05 was considered to be statistically significant.
RESULTS
No rats died during the procedures and the examinations. The data on the training tasks were similar to those of our previous reports (2).
Water maze.
With regard to swimming time, repeated-measures two-way ANOVA revealed a group difference (F3,58 = 23.718; p < 0.001), effect of block (F4,232 = 59.472; p < 0.001), and a group × block interaction (F12,232 = 1.654; p < 0.05, data not shown). Post hoc analysis using Tukey's test revealed that the pretraining HI group had a significantly shorter swimming time during the third and fourth blocks (third, p < 0.01; fourth, p < 0.05) compared with the no training HI group (Fig. 2A). The average swimming time in all blocks was 31.1 ± 2.0 s and 25.7 ± 1.5 s in no training control and pretraining control, and 65.7 ± 6.6 s and 51.7 ± 3.3 s in no training HI and pretraining HI groups, respectively (F3,58 = 23.604; p < 0.01, Fig. 2B). The pretraining HI group had a significantly shorter average swimming time than the no training HI group (p < 0.05, Tukey's test). The no training control group had an equivalent swimming time to the pretraining control group.

Acquisition curves in the water maze task in rats. Each block: swimming time (A), swimming length (C), swimming speed (E). Average of the all blocks: swimming time (B), swimming length (D), swimming speed (F). The task was started after 16 wk of recovery from HI treatment, and three trials were performed per day for 5 d. The no training HI group (□; n = 16) had significantly greater swimming lengths compared with the pretraining HI group (▪; n = 15), whereas the no-training control group (○; n = 16) showed the equivalent time and length to the pretraining control group (•; n = 15). Repeated-measures two-way ANOVA was also used to evaluate the results of water maze, followed by Tukey's test for post hoc analysis.*p < 0.05 and **p < 0.01 comparing the no training HI and pretraining HI groups in A and C. Tukey's test after one-way ANOVA was used in comparison of all blocks averages between four groups.
With regard to swimming length, repeated-measures two-way ANOVA revealed a group difference (F3,58 = 20.043; p < 0.001), effect of block (F4,232 = 60.652; p < 0.001), and a group × block interaction (F12,232 = 2.007; p < 0.05, Fig. 2C). Post hoc analysis using Tukey's test revealed that the pretraining HI group had a significantly decreased swimming length during the third to fifth blocks (third, p < 0.01; fourth, fifth, p < 0.05) compared with the no training HI group. The average swimming length in all blocks was 599.0 ± 40.4 cm and 467.7 ± 24.2 cm in no-training control and pretraining control and 1299.4 ± 144.3 cm and 947.4 ± 61.0 cm in no training HI and pretraining HI groups, respectively (F3,58 = 20.137; p < 0.01, Fig. 2D). The pretraining HI group significantly decreased the average swimming length than the no training HI group (p < 0.01, Tukey's test).
Repeated-measures two-way ANOVA of the swimming speed showed that there were no differences between the four groups (Fig. 2E). The average swimming speed in all blocks was 19.4 ± 0.7 cm/s and 18.5 ± 0.3 cm/s in no training control and pretraining control and 18.2 ± 0.4 cm/s and 18.4 ± 0.2 cm/s in no training HI and pretraining HI groups, respectively (Tukey's test, Fig. 2F).
There were no differences between the groups in the right (nonligated) hemispheric areas (60.1 ± 1.2 mm2, 59.8 ± 1.1 mm2, 55.9 ± 1.7 mm2, and 57.0 ± 0.7 mm2, 6 mm from the anterior pole of the cerebrum, and 67.0 ± 1.1 mm2, 65.8 ± 0.9 mm2, 63.8 ± 1.8 mm2, and 65.0 ± 0.6 mm2, 8 mm from the anterior pole of the cerebrum, for the no training control, pretraining control, no training HI, and pretraining HI groups, respectively). On the left (ligated) side, the no training HI group showed a significantly smaller hemispheric area compared with the no training control group at both the 6-mm level (38.4 ± 3.6 mm2 versus 57.1 ± 1.0 mm2, p < 0.01) and 8-mm level (42.4 ± 4.3 mm2 versus 65.1 ± 0.9 mm2, p < 0.01). The pretraining HI group also showed a significantly smaller hemispheric area than did the pretraining control group at the 6-mm level (37.5 ± 2.2 mm2 versus 56.2 ± 0.8 mm2, p < 0.01) and 8-mm level (41.0 ± 3.4 mm2 versus 64.4 ± 0.7 mm2, p < 0.01). There were no differences in the hemispheric areas at each level between the no training HI and pretraining HI groups.
The above-mentioned results were the same at 4-, 10-, and 12-mm levels from the anterior cerebral pole (data not shown).
DISCUSSION
In this study, rats aged 17 wk that experienced a series of rehabilitative training tasks had significantly shorter swimming times and lengths than did rats that had not undergone the rehabilitative training tasks. This behavioral improvement was not accompanied by recovery of cerebral hemispheric volume loss. These results indicate that physical and mental exercise prevented slowly progressive learning and memory disability, even when the rehabilitative training was started later than 5 wk after HI insult in the rat, an age that approximately corresponds to adolescence in humans.
It is important to cautiously appraise the experimental design. First, the trained animals could have been physically much stronger and therefore have performed better in the water maze. It was unlikely because swimming speed was equivalent between pretraining and no training rats. Second, as trained animals were handled much more, there might been difference in anxiety levels between the trained and untrained animals and this could also have affected performance in the water maze. Third, the pretraining group received more training in performing spatial learning and memory tasks and therefore might do better in the water maze. These possibilities seemed to be insignificant because there was no behavioral improvement in the water maze task in the pretraining control group compared with the no training control rats.
In our previous study of slowly progressive learning and memory disability, the acquisition curve of swimming length in the water maze at 16 wk after HI was significantly longer than at 7 wk following HI (our unpublished data). The results of swimming length at wk 7 after HI in the previous study were almost the same as those for the pretraining HI rats in the present study, indicating that the rehabilitative training tasks fully prevented the slow progression of learning and memory disability. It is important to note that the rehabilitative training tasks were commenced when the rats were 7 wk of age, an age that corresponds to adolescence or the young adult in humans. These findings entice us to speculate that the physical and mental rehabilitative exercise may prevent the late-onset slowly progressive learning and memory disability caused by neonatal HI encephalopathy, even when the exercise is started rather late in life. Such a therapeutic time window, revealed by the data from our present study, is different from the time window of “until postnatal d 14” in studies on “early life handling,” which is daily manipulation with brief maternal separation, which is well-known to enhance learning and memory ability in the adult rat, independent of HI insult in the neonatal period (6,7). Furthermore, there is no element of spatial learning and memory training in “early life handling.” Therefore, the mechanisms underlying the beneficial rehabilitative effect in the present study appear somewhat different from the mechanisms in “early life handling.”
It is interesting that the bilateral hemispheric areas in the pretraining HI group were equivalent to those in the no training HI group. This concurs with previous studies of physical and mental exercise in experimental rats (8,10,13). In the adult rat model of cerebral infarction due to middle cerebral artery occlusion, infarct volumes were equivalent regardless of whether the rat underwent environment enrichment (8), rehabilitative training (10), or voluntary exercise with running wheels (13), even though each rehabilitation paradigm benefited the behavioral recovery.
The underlying mechanisms of the rehabilitative effect remain unclear, and the mechanisms causing neonatal HI-induced late-onset slowly progressive learning disability and hemispheric volume loss have not been elucidated. However, from previous reports of animal rehabilitation, there are several plausible explanations for the rehabilitative effect. These are as follows: 1) The environmental enrichment increased levels of neurotrophic factors such as nerve growth factor and basic fibroblast growth factors in the brain (14,15). 2) Dendrite arbor and synaptic connections were increased in the enriched rehabilitation (10). 3) Long-term potentiation in the hippocampus, an important mechanism for memory consolidation, was facilitated by early life handling (16). 4) The concentration of critical neurotransmitters for synaptogenesis, namely, serotonin and 5-hydroxyindoleacetic acid, were increased in the hippocampus after early neonatal handling (9). 5) The enriched or running-facilitated environment enhanced neurogenesis and activated transcription factors(17,18).
In conclusion, the present study clearly demonstrates that rehabilitative behavioral tasks improved and prevented the neonatal HI-induced late-onset slowly progressive learning and memory disability. From a therapeutic perspective, these results give encouragement to those caregivers who dedicate their time to persons handicapped because of perinatal HI insult.

Representations of the brains of no training control, pretraining HI, and no training HI groups.

The areas (mm2) of the right (open bars) and the left (closed bars) hemispheres in each brain section (6 mm [A] and 8 mm [B] from the brain anterior pole) were measured by NIH Image software, after 17 wk of recovery from HI insult. There were no differences in the hemispheric areas at each level between the no training HI and pretraining HI groups. Tukey's test after one-way ANOVA was used. **p < 0.01 comparing the no training control and no training HI groups, and the pretraining control and pretraining HI groups.
Abbreviations
- CRT:
-
choice reaction time
- HI:
-
Hypoxia-ischemia, or hypoxic-ischemic
References
Rice JE 3rd, Vannucci RC, Brierley JB 1981 The influence of immaturity on hypoxic-ischemic brain damage in the rat. Ann Neurol 9: 131–141
Ikeda T, Mishima K, Yoshikawa T, Iwasaki K, Fujiwara M, Xia YX, Ikenoue T 2001 Selective and long-term learning impairment following neonatal hypoxic-ischemic brain insult in rats. Behav Brain Res 118: 17–25
Arteni NS, Salgueiro J, Torres I, Achaval M, Netto CA 2003 Neonatal cerebral hypoxia-ischemia causes lateralized memory impairments in the adult rat. Brain Res 973: 171–178
Hagberg H, Bona E, Gilland E, Puka-Sundvall M 1997 Hypoxia-ischaemia model in the 7-day-old rat: possibilities and shortcomings. Acta Paediatr Suppl 422: 85–88
Mishima K, Ikeda T, Aoo N, Takai N, Takahashi S, Egashira N, Ikenoue T, Iwasaki K, Fujiwara M 2005 Hypoxia-ischemic insult in neonatal rats induced slowly progressive brain damage related to memory impairment. Neurosci Lett 376: 194–199
Levine S, Haltmeyer GC, Karas GG, Denenberg VH 1967 Physiological and behavioral effects of infantile stimulation. Physiol Behav 2: 55–59
Chou IC, Trakht T, Signori C, Smith J, Felt BT, Vazquez DM, Barks JD 2001 Behavioral/environmental intervention improves learning after cerebral hypoxia-ischemia in rats. Stroke 32: 2192–2197
Dahlqvist P, Ronnback A, Bergstrom SA, Soderstrom I, Olsson T 2004 Environmental enrichment reverses learning impairment in the Morris water maze after focal cerebral ischemia in rats. Eur J Neurosci 19: 2288–2298
Fernandez-Teruel A, Gimenez-Llort L, Escorihuela RM, Gil L, Aguilar R, Steimer T, Tobena A 2002 Early-life handling stimulation and environmental enrichment: are some of their effects mediated by similar neural mechanisms?. Pharmacol Biochem Behav 73: 233–245
Biernaskie J, Corbett D 2001 Enriched rehabilitative training promotes improved forelimb motor function and enhanced dendritic growth after focal ischemic injury. J Neurosci 21: 5272–5280
Mortola JP, Dotta A 1992 Effects of hypoxia and ambient temperature on gaseous metabolism of newborn rats. Am J Physiol 263: R267–R272
Morris RG 1981 Spatial localization dose not require the presence of local cues. Learn Motiv 12: 239–260
Marin R, Williams A, Hale S, Burge B, Mense M, Bauman R, Tortella F 2003 The effect of voluntary exercise exposure on histological and neurobehavioral outcomes after ischemic brain injury in the rat. Physiol Behav 80: 167–175
Dahlqvist P, Zhao L, Johansson IM, Mattsson B, Johansson BB, Seckl JR, Olsson T 1999 Environmental enrichment alters nerve growth factor-induced gene A and glucocorticoid receptor messenger RNA expression after middle cerebral artery occlusion in rats. Neuroscience 93: 527–535
Rowntree S, Kolb B 1997 Blockade of basic fibroblast growth factor retards recovery from motor cortex injury in rats. Eur J Neurosci 9: 2432–2441
Wilson DA, Willner J, Kurz EM, Nadel L 1986 Early handling increases hippocampal long-term potentiation in young rats. Behav Brain Res 21: 223–227
van Praag H, Kempermann G, Gage FH 1999 Running increases cell proliferation and neurogenesis in the adult mouse dentate gyrus. Nat Neurosci 2: 266–270
Faverjon S, Silveira DC, Fu DD, Cha BH, Akman C, Hu Y, Holmes GL 2002 Beneficial effects of enriched environment following status epilepticus in immature rats. Neurology 59: 1356–1364
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ikeda, T., Mishima, K., Aoo, N. et al. Rehabilitative Training Tasks Improve Spatial Learning Impairment in the Water Maze Following Hypoxic-Ischemic Insult in Neonatal Rats. Pediatr Res 59, 61–65 (2006). https://doi.org/10.1203/01.pdr.0000190582.49589.14
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/01.pdr.0000190582.49589.14
This article is cited by
-
Differential Progression of Magnetization Transfer Imaging Changes Depending on Severity of Cerebral Hypoxic-Ischemic Injury
Journal of Cerebral Blood Flow & Metabolism (2008)
-
ROCK inhibition produces anxiety-related behaviors in mice
Psychopharmacology (2006)
