
Abstract
The usefulness of measurements of IGF-I or IGF-binding protein-3 (IGFBP-3) in the clinical management of growth disorders is dependent on the extent of physiologic variation in their concentrations. Our purpose was therefore to investigate the longitudinal intraindividual variation in serum concentration of IGF-I and IGFBP-3 in healthy prepubertal children. Monthly serum samples and auxologic measurements were taken over a period of 1 y from 65 prepubertal children (38 boys, 27 girls; mean age 9.1 y, range 7.8-10.8). Concentrations of IGF-I and IGFBP-3 were measured by RIA. The mean (±SD) serum concentration of IGF-I in the children was 165 ± 42.0 µg/L, with a mean coefficient of variation (CV) of 13.9% around the annual mean serum concentration for each child. The corresponding mean concentration of IGFBP-3 was 3273 ± 604.5 µg/L, and the mean CV for each child was 9.7%. These monthly longitudinal variations in IGF-I and IGFBP-3 were parallel to changes in longitudinal growth. Short-term changes (1 mo) in IGF-I were positively correlated with changes in weight (rs = 0.42, p < 0.0005) and body mass index (rs = 0.45, p < 0.0005), and negatively correlated with minor intercurrent illnesses (-0.32; p < 0.05). Seasonal fluctuations also occurred, with short term changes in IGF-I (1 mo) and IGFBP-3 (3 mo), increasing with increasing outdoor temperatures (rs = 0.30, p < 0.05 and rs = 0.39, p < 0.005, respectively). We conclude, that there are significant changes in both IGF-I and IGFBP-3 that occur in association with growth, and that IGF-I is more sensitive than IGFBP-3 to short-term changes in weight, body mass index, and intercurrent illnesses. Physiologic short-term changes must therefore be taken into consideration when using serum levels of IGF-I or IGFBP-3 in the evaluation of the short or slowly growing child.
Similar content being viewed by others
Main
Serum concentrations of IGF-I and its major binding protein, IGF-binding protein-3 (IGFBP-3), are correlated with the level of GH secretion(1,2). Consequently, it has been proposed that IGF-I or IGFBP-3 could be used as markers of GH status in situations of disturbed GH secretion, such as acromegaly(3) or decreased GH secretion(4–7). It has, however, been difficult to establish distinct cut-off values for IGF-I or IGFBP-3 that distinguish short normal children from children with GH insufficiency(8,9), at least when GH-stimulation tests are used as golden standard. If other tests are included, such as evaluating of the effect of GH therapy, low IGF-I gives high suspicion of GH deficiency(9).
The clinical evaluation of serum concentrations of IGF-I or IGFBP-3 is usually based on a single serum sample. It is known, however, that various factors influence the serum concentrations of the proteins; e.g. significant, although minor, diurnal variations have been found for both IGF-I(10) and IGFBP-3(11) in normal healthy individuals. Furthermore, cross-sectional studies have shown that changes in IGF-I and IGFBP-3 occur with age and pubertal development(12,13).
IGF-I and IGFBP-3 have been used to investigate changes in nutritional status(14). IGF-I levels are low in children with anorexia nervosa(15), whereas increased levels are found in obese children(16). Moreover, during fasting, there is a decline in the plasma concentration of IGF-I in adults, followed by a prompt rise after refeeding(17). It has also been shown that changes in energy intake, and to a somewhat lesser degree, changes in the protein content of the diet, affect IGF-I concentrations in adults(18,19). In addition, critical illness results in decreased IGF-I levels(20), which normalize during recovery(21). It is not known whether changes in food intake and minor illnesses in otherwise healthy children influence the levels of IGF-I and IGFBP-3.
In this study we have investigated monthly changes in serum concentrations of IGF-I and IGFBP-3 over a period of 1 y in healthy prepubertal children, to determine whether such changes are related to nutrition, intercurrent infections, season, and growth.
SUBJECTS AND METHODS
Subjects
An invitation to participate in this 1-y growth study was distributed to all 8- to 11-y-old children in Rosendal primary school, Göteborg, Sweden; 66% of the children agreed to participate. Two children were excluded from the analysis due to chronic disorders (GH deficiency and cystic fibrosis), and seven children did not complete the follow-up. Blood sampling was optional, and was carried out systematically in 88% of the participating children. Two boys and 22 girls entered puberty during the year of the growth study, and were excluded from the analysis. The remaining study population thus consisted of 65 prepubertal healthy children (38 boys and 27 girls). The characteristics of the children are given in Table 1. Height, weight, and weight-for-height (W/HSDSSDS; weight SDS-β × height SDS) were expressed in SD scores compared with Swedish reference values(22,23).
Study Protocol
The study was performed between October 1992 and December 1993. Measurements of height, weight, and lower leg length were recorded monthly by the same person (I.L.) and at the same time of day (0800-1000 h). The children collected morning urine samples over 3 d preceding each follow-up visit, and recorded the number of hours from the time of the previous voiding and the exact urine volume. At each follow-up visit, blood samples were taken and the children were interviewed and completed a questionnaire. A physical examination was performed at the start of the study, at 6 mo and at completion at 13 mo. The study was approved by the Ethical Committee of the Medical Faculty, University of Göteborg. Informed consent was obtained from each child and his/her parents.
Lower Leg Length
The length of the right lower leg length was measured using a knemometer as previously reported(24). At each time point, four measurements were taken, between which the child left the measuring chair. The mean of the last three measurements was then used in the analysis. The lower leg length velocity was calculated for the periods between the monthly measurements.
Biochemical Analyses
IGF-I. IGF-I was measured by an IGFBP-blocked RIA without extraction and in the presence of an approximately 250-fold excess of IGF-II (Mediagnosis GmbH, Tübingen, Germany)(25). All samples from each child were analyzed in the same assay. The intraassay CV was 9.4% at 54 µg/L, 4.4% at 219 µg/L, and 4.1% at 475 µg/L, respectively. The corresponding interassay CV was 8.7, 7.7, and 5.0%, respectively.
IGFBP-3. IGFBP-3 was measured by RIA (Mediagnost GmbH)(25). All samples from each child were analyzed in the same assay. The intraassay CV was 8.6% at 1027 µg/L, 5.6% at 2927 µg/L and 5.4% at 3956 µg/L, respectively. The corresponding interassay CV was 10.0, 9.0, and 8.0%, respectively.
Urinary GH. Urinary GH was measured using an ELISA (NordiTest; Novo Nordisk AS, Gentofte, Denmark). The urine samples were stored in the dark at 4°C and analyzed within 3 wk, as described previously(26). Repeated analysis showed that samples were unaffected by storage. The intraassay CVs were 7.9, 4.1, and 3.8% and the interassay CVs were 12.4, 9.5, and 9.9% at GH concentrations of 3, 9, and 26 ng/L, respectively. The urinary excretion of GH was evaluated using an SD score (SDS) reference that eliminates the influence of urinary volume on urinary GH measurements(27).
Questionnaire
At each follow-up visit, children were questioned about recent illnesses and food intake the day before the follow-up visit. A specific set of questions was developed for this study, because there was no appropriate questionnaire available. The questionnaires consisted of two parts. The first part was given to the parents and was used as a diary covering the month between examinations. The parents were asked about illnesses and changes in the child's appetite during the period from the last follow-up visit. The information from these questionnaires was evaluated using a scoring system, with values between 1 and 5. The second part was given to the children at the follow-up visit. Five opposite expressions were given using VAS, relating to meal size, overall appetite, and specific appetite for sweets. For example, the question "Do you have a strong desire for sweets" was answered by putting a cross on the 100 mm line between the phrases "not at all" and "very much." In the same way the questions "How much did you eat for breakfast/lunch/dinner/supper" were answered by marking the VAS scales between the phrases "nothing at all" and "very much."
Weather Data
Weather data from the area of Göteborg was obtained from the Swedish weather service. The data included the mean daily temperature and the number of hours of sunshine (i.e. hours of cloud-free sky).
Statistics
Values are given as means ± SD, if not stated otherwise, rs was used for correlation analysis. Mean values for each child over the year were used for interindividual statistical analyses.
As serum concentrations of IGF-I and IGFBP-3 are age dependent(12), values were converted into SDS using prepubertal reference values, obtained in our laboratory from healthy children of normal (± 2 SD) stature(28). Adjustment was made for this age dependency when intraindividual variation was calculated.
To study the variation between two serum samples of IGF-I or IGFBP-3, the median and maximum differences for each child between two samples taken 1 and 3 mo apart, regardless of sign, was selected. The maximum changes in IGF-I or IGFBP-3 were also tested for correlation with changes in other variables during the same time period.
Stepwise linear regressions analyses were performed using the stepwise selection option of the regular procedure in the SAS (Statistical Analysis System) software. A contribution of the variable to the regression models at a level of significance of less than 0.05 was required for the variable to be included in the model and only variables significant at a level of less than 0.05 were retained in the final model.
RESULTS
Longitudinal measurements of serum concentrations of both IGF-I and IGFBP-3 in all 65 children throughout the 1-y study period are shown in Figure 1.

Longitudinal serum concentrations of IGF-I (a) and IGFBP-3 (b) in healthy prepubertal children. All analyzed samples in individual children are joined with a line. Measurements in three children are highlighted. These children were selected because they had an intraindividual CV of IGF-I at the 5th, median, and 95th percentile. Seven children had separate values of less than -2 SD and five children had separate values of more than 2 SD of either IGF-I or IGFBP-3. Reference lines are drawn according to our IGF-I and IGFBP-3 reference values(28), and show the mean ± 1 SD and ± 2 SD, respectively.
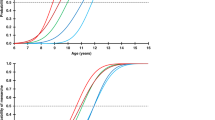
Characterization of individual mean levels of IGF-I. The mean level of IGF-I in the 65 children (calculated as the mean of the mean IGF-I levels during the year for each child) was 165 ± 42 µg/L, corresponding to -0.04 ± 0.76 SDS. The mean for the girls (182 ± 41 µg/L) was significantly higher than that for the boys (153 ± 39 µg/L) (Kruskall-Wallis, p < 0.05). The size of the child, measured as either height SDS (Fig. 2a) or weight SDS (Fig. 2b), as well as height velocity (Fig. 2c) and weight gain (Fig. 2d) correlated with the yearly individual mean IGF-I SDS (Table 2). Multiple stepwise regression analyses, including all variables with significant univariate correlation (p < 0.05) from Table 2, selected height SDS, gender and height velocity as significant parameters that, together, could explain 45% of the variation in the IGF-I SDS (r2 = 0.45, p < 0.0001, Table 3).

The mean serum level of IGF-I SDS during the year in all children correlated with height SDS (a), weight SDS (b), height velocity (c), and weight gain (d).
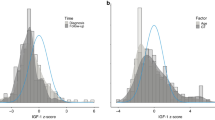
Changes in IGF-I levels within each child. The mean CV for IGF-I, adjusted for age, for each child was 13.9% (range 6.0-28.9%) [without age adjustment 13.6% (range 6.9-28.3)]. Auxologic variables and gender could not explain differences in the magnitude of variation between the children. When samples during illness were excluded from the analysis, the mean variation reduced to ± 13.1% (range 3.5-27.0%). The median and maximum variation between samples was analyzed using pairs of samples from each child at intervals of 1 and 3 mo. The 5th and 95th percentile for median differences in SDS in IGF-I were -0.4 to +0.4, although for the maximum changes were -1.2 to +1.3 SDS over 1 mo (Fig. 3a). The median difference in SDS between samples taken at 3-monthly intervals was -0.4 to +0.3, although the maximum change was -1.9 to +0.9 (Fig. 3a). The maximum change were correlated with changes in BMI (rs = 0.44, p < 0.0005), but was also influenced by illness (rs = -032, p < 0.01) and outdoor temperature (rs = 0.28, p < 0.01, Table 4). Maximum changes over 3 mo were only related to changes in outdoor temperature (rs = 0.40, p < 0.01, Table 4). No correlation was found with changes in urinary GH or in the child's ranking of meal sizes.

Variation of IGF-I (a) and IGFBP-3 (b) over 1- and 3-mo intervals. The median and maximum variation was calculated from all eleven differences during 1 y.
Characterization of individual mean levels of IGFBP-3. The mean serum concentration of IGFBP-3 was 3272 ± 605 µg/L, which is comparable with the IGFBP-3 reference value (-0.10 ± 0.90 SDS). There was no difference between boys and girls in the mean level of IGFBP-3. The size of the child, evaluated as height SDS (Fig. 4a) or weight SDS (Fig. 4b), as well as height velocity (Fig. 4c) and weight gain (Fig. 4d), correlated with the level of IGFBP-3 (Table 2). Using stepwise multiple regression analysis, 33% of the level of IGFBP-3 could be explained by gender, height SDS, and weight gain (r2 = 0.33, p < 0.0001, Table 3).

The mean level of IGFBP-3 SDS during the year in all children was correlated with the height SDS (a), weight SDS (b), height velocity (c), and weight gain (d).
Changes in IGFBP-3 levels within each child. The mean CV for IGFBP-3 was 9.7% (range 4.1-36.0%) [without age adjustment 9.3% (range 4.7-35.6)]. No decrease in the CV was achieved when samples taken after illness were excluded. The 5th and 95th percentile for median changes in IGFBP-3, measured every month, were -0.6 to +0.3 SDS compared with maximum changes of -1.3 to +1.3 SDS. When samples are measured every 3 mo, the 5th and 95th percentiles for median differences were -0.7 to +0.4 SDS and for maximum changes -1.2 to +1.2 SDS (Fig. 3b). In contrast to the changes in IGF-I, changes in IGFBP-3 were not related to recent illness and changes in BMI, although there was a correlation with growth over a 3-mo interval (Table 4). Changes in IGFBP-3 over both 1 and 3 mo correlated with season, evaluated as changes in either outdoor temperature or hours of sunshine, although no correlation to changes in urinary GH was found (Table 4).
DISCUSSION
Our main finding was that there is a considerable monthly variation in both IGF-I and IGFBP-3 in individual children, although the serum concentrations in monthly samples from individual children cluster around a certain level that is dependent on the size of the child. These longitudinal changes in IGF-I and IGFBP-3 parallel changes in height velocity and weight and are influenced by illnesses and outdoor temperature. Thus, biologic variation exceeds the analytical precision and should be considered when evaluating single IGF-I or IGFBP-3 values in clinical practice.
In our study, short-term changes in IGF-I and IGFBP-3 were related to physiologic events, i.e. weight changes, height gain, and illness. It is well known that serum concentrations of both IGF-I and IGFBP-3 increase with age and change during puberty(12). A clear finding from our study is that short-term changes in serum concentrations of IGF-I and IGFBP-3 correlates to changes in weight and BMI rather than to longitudinal bone growth. IGF-I and IGFBP-3 in serum originates from most tissues in the body. It is therefore possible that short-term variations in the concentrations in serum of IGF-I do not closely mirror the amount and activity of IGF-I within the bone tissue. It can therefore be speculated that the mean level of IGF-I in an individual child is regulated differently than the short-term variations around this level. Many studies have shown that the mean level of IGF-I correlates to height (i.e. long-term height velocity)(2,12). Our results suggest that the changes around this overall level are more closely related to changes in weight, body composition, and to illnesses. In addition, it has been shown that dietary changes affect IGF-I and IGFBP-3(17). Although there was no significant correlation between concentrations of IGF-I or IGFBP-3 and changes in the appetite or meal sizes reported by the parents or their children in our study, methodologic problems in this evaluation do not rule out that such correlations may exist. The finding that short-term changes in IGF-I and IGFBP-3 are not circumstantial, emphasizes the importance of following the child's growth process and the limitations of evaluating only one auxologic or biochemical variable in a child.
Seasonal variation in growth occurs, with the height velocity of healthy children being greatest when the days are longest(29,30). The finding that GH-insufficient children receiving GH therapy follow the same seasonal growth pattern(31) suggests that the regulatory mechanism behind the seasonal growth changes are not due mainly to differences in GH secretion. In our study, correlations were found between changes in IGF-I, IGFBP-3, and short-term height velocity, as well as with changes in outdoor temperature, which indicates that seasonal variation in growth is associated with changes in IGF-I and IGFBP-3. No significant parallel changes occurred in urinary GH, although the large daily variation in urinary GH measurements may hide such a relationship. The increased levels of IGF-I and IGFBP-3 in relation to season, evaluated as outdoor temperature, without changes in GH, indicates that there is an increase in GH sensitivity during this time. This may be due to an effect induced by sunlight, but it is also possible that higher outdoor temperatures are associated with increased physical activity resulting in increased GH sensitivity.
It has been proposed that concentrations of IGF-I and IGFBP-3 may be used to diagnose children with GH insufficiency(6,7). Several useful reference charts have been developed to improve diagnosis, as the levels of IGF-I and IGFBP-3 change with age and pubertal development(12,28). In addition to the large intraindividual variation, interpretation of IGF-I and IGFBP-3 levels is confounded by the fact that the levels are related to the size of the child. As most children with GH IGFBP-3 levels is confounded by the fact that the levels are related to the size of the child. As most children with GH insufficiency are short, they would be expected to have lower levels of both IGF-I and IGFBP-3 than taller children(2), although studies on twins have shown that there is a strong genetic influence on the level of IGF-I, and that only a small proportion of the variation in IGF-I and IGFBP-3 can be explained by growth(32). The monthly variation in both IGF-I and IGFBP-3 in individual children must be taken in account into clinical evaluations. Thus, if repeated IGF-I concentrations are to be used to evaluate treatment, changes have to exceed -0.4 to +0.4 SDS to be considered significant. Similarly, for IGFBP-3, a change of -0.6 to +0.3 SDS is required to reflect a significant treatment effect. An even larger magnitude of variation is expected if samples are analyzed in different assays. Thus, in situ, when the interest is to evaluate longitudinal changes, samples taken in an individual should be analyzed in a single assay and all possible factors, such as variations related to season, weight changes, and infections must be considered. Because multiple factors influences short-term changes in IGF-I and IGFBP-3, it is not possible to adjust for such factors in the clinical interpretation. Instead, changes must either exceed the normal intraindividual variation shown here, or be compared with matched controls followed in parallel.
Despite the intraindividual variation, repeated measurements of serum concentrations of IGF-I or IGFBP-3 cluster around a specific level in individual children. This level depends on the size of the child and, in the case of IGF-I, on gender and height velocity(2,12).
The results of this study show that short-term changes in IGF-I correlate with short-term changes in growth and are influenced by season and minor illness. These factors, with the exception of illness have a subsequent effect on IGFBP-3. It is known that more than 95% of circulating IGF-I is bound in a heterotrimer to IGFBP-3 and an acid-labile glucoprotein, and only about 1% of IGF-I exists in the free form under normal conditions(33). The concentration of IGFBP-3 is dependent on the amount of GH secretion(34), and the IGF-I bound to the heterotrimer ALS-IGFBP-3 in the circulation is believed to increase the biologic half life of IGF-I(35). The IGF-I that is not bound to IGFBP-3 or free in the circulation, forms binary complexes mainly with IGFBP-1, -2, -3, -4, and -6(14,36,37). These binding proteins have a high turnover(38) and are sensitive to proteolysis(39). Increased proteolytic activity in serum during severe illness may, however, also influence the reliability of IGFBP-3 evaluations(40). It is not possible, from this study to evaluate how these different mechanisms affect the observed variation in IGF-I and IGFBP-3. Our data are in agreement with changes found during critical illnesses; minor illnesses occurring between two IGF-I samples decreased the serum concentration of IGF-I, although similar sensitivity to infections was not found for IGFBP-3. In addition to infections affecting proteolytic activity, studies in critically ill patients have shown that GH insensitivity occurs, which may explain why IGF-I is more sensitive to infections than IGFBP-3(20). Thus, IGF-I is more sensitive than IGFBP-3 to short-term physiologic changes. IGF-I should be measured in clinical situations where it is important to evaluate short-term changes. Measurements of IGFBP-3 provide more information during the long-term follow-up.
In conclusion, there are significant monthly fluctuations in IGF-I and IGFBP-3 in healthy children, although the serum concentrations in individual children are clustered around a certain level. Interestingly, the longitudinal changes in IGF-I and IGFBP-3 occur in parallel to changes in growth and weight. Furthermore, IGF-I concentrations decrease after illness and during changes in outdoor temperature. This means that the individual biologic variations exceed the analytical precision, and have to be considered when evaluating single IGF-I or IGFBP-3 concentrations in clinical practice. IGF-I and IGFBP-3 should be considered together, as they provide different information: IGF-I provides information about influences during the previous month and IGFBP-3 during the last 3 mo.
Abbreviations
- BMI :
-
body mass index
- C.V. :
-
coefficient of variation
- GH :
-
growth hormone
- GHBP :
-
growth hormone binding protein
- IGFBP-3 :
-
IGF-binding protein-3
- VAS :
-
visual analogue scales
- W/H SDS SDS :
-
weight for height SD-scores
References
Rinderknecht E, Humbel RE 1978 The amino acid sequence of human insulin-like growth factor I and its structural homology with proinsulin. J Biol Chem 153: 2769–2776.
Blum WB, Albertsson-Wikland K, Rosberg S, Ranke MB 1993 Serum levels of insulin-like growth factor I (IGF-I) and IGF binding protein 3 reflect spontaneous growth hormone secretion. J Clin Endocrinol Metab 76: 1610–1616.
Grinspoon S, Clemmons D, Swearingen B, Klibanski A 1995 Serum insulin-like growth factor-binding protein-3 levels in the diagnosis of acromegaly. J Clin Endocrinol Metab 80: 927–932.
Smith WJ, Nam TJ, Underwood LE, Busby WH, Celnicker A, Clemmons DR 1993 Use of insulin-like growth factor-binding protein-2 (IGFBP-2), IGFBP-3, and IGF-I for assessing growth hormone status in short children. J Clin Endocrinol Metab 77: 1294–1299.
Lee PDK, Wilson DM, Roundtree L, Hintz RL, Rosenfeld RG 1990 Efficacy of insulin-like growth factor I levels in predicting the response to provocative growth hormone testing. Pediatr Res 27: 45–51.
Rosenfeld RG, Albertsson-Wikland K, Cassorla F, Frasier SG, Hasegawa Y, Hintz RL, Lafranchi S, Lippe B, Loriaux L, Melmed S, Preece MA, Ranke MB, Reiter EO, Rogol AD, Underwood LE, Werther GA 1995 Diagnostic controversy: the diagnosis of childhood growth hormone deficiency revisited. J Clin Endocrinol Metab 80: 1532–1540.
Kriström B, Jansson C, Rosberg S, Albertsson-Wikland K 1997 Growth response to growth hormone (GH) treatment relates to serum insulin-like growth factor-I (IGF-I) and IGF-binding protein-3 in short children with various GH secretion capacities. J Clin Endocrinol Metab 82: 2889–2898.
Cianfarani S, Boemi S, Spagnoli A, Cappa M, Argiro G, Vaccaro F, Manca Bitti ML, Boscherini B 1995 Is IGF binding protein-3 assessment helpful for the diagnosis of GH deficiency?. Clin Endocrinol (Oxf) 43: 43–47.
Ranke MB, Blum WF, Bierich JR 1988 Clinical relevance of serum measurements of insulin-like growth factors and somatomedin binding protein. Acta Paediatr Scand Suppl 347: 114–126.
Minuto F, Underwood LE, Grimaldi P, Furlanetto RW, van Wyk JJ, Giordano G 1981 Decreased serum somatomedin C concentrations during sleep: temporal relationship to the nocturnal surges of growth hormone and prolactin. J Clin Endocrinol Metab 52: 399–403.
Jörgensen JOL, Möller N, Lauritzen T, Alberti KGMM, Örskov H, Christiansen JS 1990 Evening versus morning injections of growth hormone (GH) in GH-deficient patients: effects of 24-hour patterns of circulating hormones and metabolites. J Clin Endocrinol Metab 70: 207–214.
Juul A, Dalgaarn P, Blum WF, Bang P, Hall K, Michaelsen KF, Müller J, Skakkebæk NE 1995 Serum levels of insulin-like growth factor (IGF)-binding protein-3 (IGFBP-3) in healthy infants, children, and adolescents: the relation to IGF-I, IGF-II, IGFBP-1, IGFBP-2, age, sex, body mass index, and pubertal maturation. J Clin Endocrinol Metab 80: 2534–2542.
Blum WF, Ranke MB 1990 Use of insulin-like growth factor binding protein-3 for the diagnosis of growth disorders. Horm Res 33: 31–37.
Clemmons DR 1993 IGF binding proteins and their functions. Mol Reprod Dev 35: 368–375.
Rappaport R, Previot C, Czernichow P 1980 Somatomedin activity and growth hormone secretion; changes related to body weight in anorexia nervosa. Acta Paediatr Scand 69: 37–41.
Loche S, Cappa M, Borrelli P, Faedda A, Crinò A, Cella SG, Corda R, Müller EE, Pintor C 1987 Reduced growth hormone response to growth hormone-releasing hormone in children with simple obesity: evidence for somatomedin-C mediated inhibition. Clin Endocrinol (Oxf) 27: 145–153.
Clemmons DR, Klibanski A, Underwood LE, McArthur JW, Ridgway EC, Beitins IZ, van Wyk JJ 1981 Reduction of plasma immunoreactive somatomedin-C during fasting in humans. J Clin Endocrinol Metab 53: 1247–1250.
Isley WL, Underwood LE, Clemmons DR 1983 Dietary components that regulate serum somatomedin-C concentrations in humans. J Clin Invest 71: 175–182.
Clemmons DR, van Wyk JJ 1984 Factors controlling blood concentration of somatomedin C. Clin Endocrinol Metab 13: 113–143.
Ross RJM, Miell J, Freeman E, Jones J, Matthews D, Preece M, Buchanan C 1991 Critically ill patients have high basal growth hormone levels with attenuated oscillatory activity associated with low levels of insulin-like growth factor-I. Clin Endocrinol (Oxf) 35: 47–54.
Hawker FH, Stewart PM, Baxter RC, Borkmann M, Tan K, Caterson ID, McWilliam DB 1987 Relationship of somatomedin-C/insulin-like growth factor I levels to conventional nutrition indices in critically ill patients. Crit Care Med 15: 732–736.
Karlberg P, Taranger J, Engström I, Lichtensten H, Svennberg-Redegren I 1976 The somatic development of children in a Swedish urban community. Acta Paediatr Suppl. 258: 1–70.
Karlberg J, Albertsson-Wikland K 1996 Nutrition and linear growth in childhood. In: Bindels JG, Goedgart AC, Visser HKA (ed) Recent Developments in Infant Nutrition. Kluwer Academic Publishers, Dordrecht,. pp 112: 127
Valk IM, Chabloz AM, Smals AG, Kloppenborg PW, Cassorla FG, Schutte EA 1983 Accurate measurements of the lower leg length and the ulnar length and its application in short term growth measurement. Growth 47: 53–66.
Blum WF, Breier BH 1994 Radioimmunoassays for IGFs and IGFBPs. Growth Regul 4: 11–19.
Main KM, Jarden M, Angelo L, Dinesen B, Hertel NT, Juul A, Mueller J, Skakkebaek NE 1994 The impact of gender and puberty on reference values for urinary growth hormone excretion: a study of 3 morning urine samples in 517 healthy children and adults. J Clin Endocrinol Metab 79: 865–871.
Gelander L, Karlberg J, Larsson LA, Albertsson-Wikland K 1998 Overnight urinary growth hormone in normally growing prepubertal children: effect of urine volume. Horm Res 49: 8–16.
Boguszewski M, Jansson C, Rosberg S, Albertsson-Wikland K 1996 Changes in serum insulin-like growth factor I (IGF-I) and IGF-binding protein levels during growth hormone treatment in prepubertal short children born small for gestational age. J Clin Endocrinol Metab 81: 3902–3908.
Gelander L, Karberg J, Albertsson-Wikland K 1995 Seasonality in lower length and height velocity in prepubertal children. Acta Paediatr 83: 1249–1254.
Marshall WA, Swan AV 1971 Seasonal variation in growth rates of normal and blind children. Hum Biol 43: 502–516.
Rudolf MC, Zadik Z, Linn S, Hochberg Z 1991 Seasonal variation in growth during growth hormone therapy. Am J Dis Child 145: 769–772.
Kao PC, Matheny APJ, Lang CA 1994 Insulin-like growth factor-I comparison in healthy twin children. J Clin Endocrinol Metab 78: 310–312.
Baxter RC, Martin JL 1989 Structure of the Mr 140:000 growth hormone-dependent insulin-like growth factor binding protein complex: determination by reconstitution and affinity labeling. Proc Natl Acad Sci USA 86: 6898–6902.
Copeland KC, Underwood LE, van Wyk JJ 1980 Induction of immunoreactive somatomedin C in human serum by growth hormone: dose-response relationships and effect on chromatographic profiles. J Clin Endocrinol Metab 50: 690–697.
Blum WF, Ranke MB 1990 Insulin-like growth factor binding proteins (IGFBPs) with special reference to IGFBP-3. Acta Paediatr Scand 367: 55–62.
Kiefer MC, Ioh RS, Bauer DM, Zapf J 1991 Molecular cloning of a new human insulin-like growth factor binding protein. Biochem Biophys Res Commun 176: 219–225.
Rechler MM, Brown AL 1992 Insulin-like growth factor binding proteins: gene structure and expression. Growth Regul 2: 55–60.
Guler HP, Zapf J, Schmid C, Froesch ER 1989 Insulin-like growth factors I and II in healthy man. Estimation of half-life and production rates. Acta Endocrinol (Copenh) 121: 753–758.
Conover CA, Freemark MC, Zapf J 1993 Posttranslational regulation of insulin-like growth factor binding protein-4 in normal human fibroblasts. Insulin-like growth factor dependance and biological studies. J Clin Invest 91: 1129–1137.
Davies SC, Wass JA, Ross RJ, Cotterill AM, Buchanan CR, Coulson VJ, Holly JM 1991 The induction of a specific protease for insulin-like growth factor binding protein-3 in the circulation during severe illness. J Endocrinol 130: 469–473.
Acknowledgements
The authors thank Ingela Larsson and Birgit Lidvall for excellent technical support. We also express our gratitude to the teachers and staff at Rosendal school and to the children and parents who made this study possible.
Author information
Authors and Affiliations
Additional information
Supported by grants from the Swedish Medical Research Council (7509), Medical Faculty, University of Göteborg, Frimurare Barnhusdirektionen i Göteborg, Göteborgs Barnklinikers Forskningsfond, Wilhelm & Martina Lundgren Foundation, the First of May Flower Annual Campaign, "Förenade Liv" Mutual Group Life Insurance Company, Stockholm, Stiftelsen Samariten, Svenska Sällskapet för Medicinsk forskning Novo Nordisk Svenska AB and Novo Nordisk AS and Pharmacia and Upjohn.
Rights and permissions
About this article
Cite this article
Gelander, L., Blum, W., Larsson, L. et al. Monthly Measurements of Insulin-Like Growth Factor I (IGF-I) and IGF-Binding Protein-3 in Healthy Prepubertal Children: Characterization and Relationship with Growth: The 1-Year Growth Study. Pediatr Res 45, 377–383 (1999). https://doi.org/10.1203/00006450-199903000-00015
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199903000-00015
This article is cited by
-
Seasonal variations in growth and body composition of 8–11-y-old Danish children
Pediatric Research (2016)
-
Growth hormone (GH) dose-dependent IGF-I response relates to pubertal height gain
BMC Endocrine Disorders (2015)
-
Growth factors, adiponectin, leptin and body mass index in pre-pubertal children born large for gestational age
Journal of Endocrinological Investigation (2011)
-
Seasonality of growth in Shanghai infants (n=4128) born in 11 consecutive years
European Journal of Clinical Nutrition (2001)
