
Abstract
During the course of human pregnancy, glucocorticoid (GC) treatment is given when preterm delivery is expected. This treatment is successful in stimulating the development of the fetal lung. However, in animal studies, a number of side effects of perinatal GC treatment have been described. The aim of the present study was to evaluate in humans the effects of antenatal GC treatment on development of the immune system. In addition, we examined the development of immune reactivity in infants born preterm and at term who did not receive GC treatment antenatally. We tested mitogen-induced T cell proliferation, natural killer cell activity, and lipopolysaccharide-induced IL-6 production in cord blood samples. We found that there is a significant effect of gestational age on the capacity of T cells to proliferate and of natural killer cells to kill K562 tumor cells. The capacity to produce IL-6 does not change between gestational age 26 and 41 wk. Moreover, our results show that antenatal treatment with GC does have immunomodulatory effects: T cell proliferation is decreased in infants born very preterm (gestational age 26-31 wk) as well as in infants born between 32 and 36 wk of gestation. In contrast, the activity of natural killer cells is only increased in GC-treated infants born between 26 and 31 wk. We did not observe a significant effect of antenatal GC treatment on the capacity to produce IL-6.
Similar content being viewed by others


Main
GC are frequently administered to pregnant women to accelerate maturation of the fetal lung when preterm delivery is expected to occur. Antenatal GC treatment has been shown to be successful in stimulating fetal lung maturation and in preventing respiratory distress syndrome, neonatal death, and intraventricular hemorrhage(1–3). However, GC are known to influence the activity of virtually all organ systems in the body, possibly resulting in adverse side effects.
In animal studies, it has been shown that antenatal or early neonatal administration of GC can have profound and long-lasting effects on the development of the neuroendocrine system, on behavior, and on the cardiovascular system(4,5).
Acute effects of administration of betamethasone on the human fetus include inhibition of fetal breathing, body movements, and heart rate variation(6). These effects are of transient nature; on d 4 after treatment, baseline values are observed again(6). In humans, a long-term follow-up study of the effects of antenatal GC on social and emotional development, psychomotor development, and growth found no differences between the control and treatment group until the age of 12 y(7,8). However, it became evident from this study that there were a higher number of hospital admissions because of infectious diseases during the first year of life in the group of children that had been exposed to GC antenatally(8). Interference of antenatal GC treatment with the development of the immune system may be partially responsible for this effect. Such concerns have been expressed in early reports(9), but very little evidence has been presented. In pregnant mice, long-term GC administration interferes with both T and B cell reactivity in the offspring(10). In rats, exposure to GC during late pregnancy resulted in substantial but transient decreases in PHA-induced T cell proliferation and IL-2 production in the offspring(11). We have previously shown that short-term neonatal administration of GC to rats results in prolonged changes in both thymic development and reactivity of the neuroendocrine system(12,13).
In human adults, GC are frequently used as immunosuppressive drugs. Exposure to GC is known to result in transient inhibition of cytokine production both in vivo and in vitro(14,15). In addition, GC inhibit the proliferative activity of T cells and are potent inducers of apoptosis in the thymus(16,17). From previous studies, we know that neonatal T cells are far more sensitive to the acute inhibitory effects of GC than are adult T cells(18,19). Therefore, it is possible that antenatal GC administration will interfere with the development of T cell reactivity.
The aim of the present study was to evaluate the effect of antenatal administration of GC on immune function at birth. In addition, we examined the development of immune reactivity without interference of GC treatment in infants born very preterm (gestational age 26-31 wk), preterm (gestational age 32-36 wk), and at term (37-41 wk). We chose to examine the proliferative capacity of T cells, IL-6 production by monocytes, and the activity of NK cells in human cord blood samples.
METHODS
Subjects and blood sampling. Heparinized venous cord blood samples were collected at the Department of Obstetrics and Gynecology of the University Hospital Utrecht. In the GC treatment group (n = 38), mothers received betamethasone in two doses of 12 mg intramuscularly on 2 consecutive days. The interval between administration of the second dose of betamethasone and delivery was <1 d in 12 cases, 1 to 7 d in 13 cases, and >1 wk in 13 cases.
Blood was collected in heparinized tubes for immunologic measurements and in EDTA tubes for cortisol determination within 10 min after delivery. The collection of blood was approved by the Ethics Committee of the Academic Hospital, and parents gave informed consent.
T cell proliferation. The proliferative capacity of T cells was determined in whole blood cultures. Whole blood was diluted 1:10 in medium [RPMI 1640 (GIBCO, Grand Island, NY) supplemented with glutamine (2 mmol/L), 100 U/mL penicillin, and 100 µgram/mL streptomycin]. One hundred microliters of diluted blood was cultured for 96 h in round-bottom 96-well plates (Nunc, Glostrup, Denmark) with 50 µL PHA (Murex Diagnostics, Darford, UK) in medium (final concentration 25 µg/mL) or with medium alone. At 16-18 h before the end of the culture, 1 µCi (37 kBq) 3H-thymidine [specific activity 75 gBq/mmol (Amersham, Amersham, UK)] was added. At the end of the culture period, cultures were harvested by use of an automated cell harvester and incorporated radioactivity was determined in a liquid scintillation counter.
The stimulation index was calculated as cpm in the presence of PHA divided by cpm in cultures with medium only.
NK cell activity. NK cell activity was determined as the capacity of diluted cord blood to kill K562 cells. K562 cells were labeled with Na51CrO4 (Amersham). 104-labeled K562 cells in 100 µL were dispensed into 96-well round-bottom tissue culture plates and 100 µL of blood diluted 1:2 in medium was added. Plates were centrifuged for 5 min (100 × g) and were incubated at 37°C for 4 h. At the end of the incubation, plates were centrifuged again and supernatants of triplicate samples were counted in a gamma counter. Total 51Cr release and spontaneous release were determined in wells containing 1% Triton X-100 or medium, respectively. NK cell activity was calculated as follows: % killing = (ER - SR)/(TR - SR) × 100, where ER = mean cpm experimental release, SR = means cpm spontaneous release, and TR = mean cpm total release.
Monocyte IL-6 production. The capacity of monocytes to produce IL-6 was determined in whole blood cultures that were stimulated with LPS (Escherichia coli O127:B8, Difco Laboratories, Detroit, MI). Whole blood was diluted 1:10 in medium and 150 µL of the diluted blood was stimulated with 50 µL of LPS (10 µg/mL) for 18 h. Supernatants were harvested and IL-6 was determined by ELISA (Pelikine, CLB, Amsterdam, The Netherlands).
Cellular composition of cord blood. Absolute numbers of lymphocytes per sample were determined. For lymphocytes subset analysis, whole blood was incubated with conjugated MAb against CD4, CD8, CD3, and CD16/56 (Simultest, Becton and Dickinson, Mountain View, CA). Subsequently, red blood cells were lysed and samples were analyzed with a flow cytometer (FACS-Star+, Becton and Dickinson).
Plasma cortisol. The concentration of cortisol in plasma was determined with a commercially available kit (Abbott).
Statistical analysis. To evaluate whether there were differences between very preterm newborns (26-31 wk), preterm newborns (32-36 wk), and term newborns (37-41 wk) in the function of cord blood cells, univariate analyses of covariance (ANCOVA) were performed with sex and birth weight percentiles as covariates. These three parameters were chosen as covariates because initial analysis revealed that they contributed in a marginally significant way to part of the outcome measures. Birth weight percentiles are divided into three groups. Newborns with a birth weight between 10th percentile (P10) and 90th percentile (P90) are APA, those with a birth weight below P10 are SGA, and those with a birth weight above P90 are LGA. To index these groups, two dummy variables, "SGA" and "LGA," were formed. SGA is coded 1 in case of a birth weight below P10 and coded 0 otherwise. LGA is coded 1 in case of a birth weight above P90 and coded 0 otherwise. Significant main effects of gestational age on immunologic outcome were followed by Tukey tests(20) to determine which pairs of groups, i.e. very preterm (26-31 wk), preterm (32-36 wk), and full-term (37-41 wk), are significantly different at the 0.05 level.
We performed univariate ANCOVA with sex and the above-mentioned dummy variables SGA and LGA as covariates to determine whether there were differences in the effect of antenatal GC treatment on distribution and function of cord blood cells of early preterm infants born before 32 wk of gestation and of preterm infants born between 32 and 36 wk of gestation. This is a 2 (treatment, betamethasone versus no treatment) × 2 (gestational age 26-31 versus 32-36 wk) design. Data of outcome variables did not meet the assumption of normality and, therefore, a square root or logarithmic transformation was applied to these data before the above-described analyses.
RESULTS
Subject characteristics. To analyze the effect of gestational age on immune function, we studied two groups of untreated preterm infants (gestational age 26-31 and 32-36 wk) and one group of untreated full-term newborns (gestational age 37-41 wk). Subject characteristics are summarized in Table 1.
The effect of antenatal GC treatment was analyzed only in cord blood samples obtained from the two groups of preterm infants born at gestational age 26-31 and 32-36 wk.
Effect of gestational age on T cell reactivity. To investigate the effect of gestational age on the proliferative capacity of T cells at birth, we examined T cell proliferative responses in cord blood samples. Whole blood cultures were stimulated with the T cell mitogen PHA, and the incorporation of 3H-thymidine was determined as a measure of T cell proliferative capacity.
The effect of gestational age on T cell proliferation was analyzed in cord blood samples of infants who did not receive GC treatment antenatally. The results in Table 2 show that there is a small but significantly effect of gestational age on T cell proliferation after covariance adjustment. Post hoc testing shows that T cells of children born at gestational age 32-36 wk show a significantly larger proliferative response than the other two groups examined (p < 0.05).
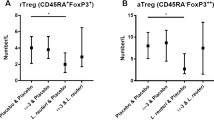
Effect of GC treatment on T cell proliferation. The proliferative capacity of T cells was examined in cord blood samples of infants born at gestational age 26-31 and 32-36 wk who had been exposed to antenatal GC treatment and in cord blood samples of infants born at the same gestational age who had not received GC prenatally. Our data show that antenatal exposure to GC results in a reduced capacity of cord blood T cells to proliferate (Table 3 and Fig. 1). Inhibition of the proliferative capacity of T cells is observed both at 26-31 and at 32-36 wk. Moreover, the magnitude of the inhibition of T cell proliferation by antenatal GC administration is similar in both groups.

Effect of antenatal GC treatment on T cell proliferation in cord blood. Cord blood samples were stimulated with PHA for 96 h and incorporation of 3H-thymidine was determined. Data are expressed as stimulation index and represent mean and SEM. Open bars, no treatment. Hatched bars, antenatal GC treatment. For details, see Table 3 and text.
It seems that the dummy variable LGA contributes in a marginally significant way to the explained variance of PHA-stimulated T cell proliferation. The positive raw regression coefficient (1.37) suggests that neonates who are LGA have significantly higher PHA-induced proliferation than AGA and SGA infants.
Effect of gestational age on NK cell activity. The activity of NK cells was investigated by testing the capacity of cord blood samples to kill the NK-cell-sensitive target cell line K562. The data summarized in Table 2 show that there is a significant effect of gestational age on NK cell activity in the absence of GC treatment. Post hoc testing revealed that NK activity is significantly lower at 26-31 wk than after 32 wk (p < 0.05).
Effect of antenatal treatment with GC on NK cell activity. The effect of prenatal GC treatment on NK cell activity was analyzed in infants born preterm. Interestingly, we observed a significant gestational age by antenatal GC-treatment interaction for NK cell activity (Table 3). These results strongly suggest that antenatal GC treatment accelerates the development of NK cell activity in infants born between 26 and 31 wk (Fig. 2).

Effect of antenatal betamethasone treatment on NK cell activity. Cord blood samples were tested for the capacity of NK cells to kill K562 target cells. Data represent mean and SD. Open bars, no treatment. Hatched bars, betamethasone. For details see Table 3 and text.
Effect of gestational age on IL-6 production by monocytes. To investigate the effect of gestational age on the capacity of monocytes to produce the cytokine IL-6, whole blood cultures were stimulated with LPS and IL-6 levels in the culture supernatant were determined by ELISA. Comparison of IL-6 production in samples obtained from the three groups of untreated infants revealed that there is no statistically significant relation between gestational age and IL-6 production (Table 2).
Effect of antenatal GC treatment on IL-6 production. Antenatal GC treatment does not have any significant effect on the capacity of monocytes to produce IL-6 after ex vivo stimulation with LPS (Table 3).
Effect of antenatal GC on cellular composition of cord blood. To examine whether the effects of GC treatment on T cell function and NK cell activity can be attributed to changes in the cellular composition of the cord blood samples, we analyzed absolute numbers of CD3, CD4, CD8, and CD16/56 positive cells in the same blood samples.
Our data show that the number of CD3, CD4, CD8, and CD16/56 positive cells is lower in infants born between 26 and 31 wk than in infants born between 32 and 36 wk or at term (Table 4). However, we did not observe any effect of GC treatment on CD3, CD4, CD8, and CD16/56 positive cells.
Effect of antenatal GC on cortisol levels in cord blood. Plasma cortisol concentrations were determined in cord blood samples of children born at gestational age 26-31 and 32-36 wk who had or had not been exposed to betamethasone antenatally. The results summarized in Table 5 show that antenatal treatment with betamethasone results in decreased levels of cortisol in cord blood. The effect is most pronounced in the group with gestational age 32-36 wk.
DISCUSSION
In the first part of the present study, we compared immune reactivity in cord blood samples of infants born at gestational age 26-31, 32-36, and 37-41 wk. Our data show that during the second and third trimester of pregnancy, the capacity of NK cells to kill target cells is still developing: NK cell activity in cord blood from infants born between 26 and 31 wk is very low compared with the activity observed in samples from infants born after 32-36 wk or at term. In contrast, the capacity to produce the cytokine IL-6 has already reached its full capacity in the youngest group.
The second part of the present study was designed to investigate whether, in humans, antenatal exposure to GC results in changes in the development of the fetal immune system. Our data show that administration of GC during the second and third trimester of pregnancy has differential effects on immune effector functions.
Antenatal exposure to GC results in increased NK cell activity in the infants born very preterm. However, in infants born between 32 and 36 wk, we did not observe any effect of antenatal GC treatment. Moreover, NK cell activity at gestational age 32-36 wk is similar to the activity at term. These data strongly suggest that GC can accelerate the maturation of NK cells in the infants born very preterm.
With respect to accelerated maturation of the fetal lung, a number of mechanisms seem to be involved. GC stimulate surfactant synthesis, differentiation of alveolar epithelial cells, connective tissue maturation, and production of antioxidant enzymes(21). Another important effect of GC in the lung is induction of increased β-adrenergic receptor expression on alveolar cells(22). These receptors play an important role in regulating lung function at birth. Interestingly, NK cells also express β-adrenergic receptors, and in vivo exposure to β-adrenergic β-adrenergic agonists enhances NK cell activity in the blood of adults(23,24). If may be possible that the enhanced NK cell activity in the infants born very preterm is the result of increased levels of β-adrenergic receptors on NK cells due to GC treatment. At birth, these receptors will be activated by the increased levels of catecholamines, resulting in enhanced NK cell activity.
In contrast with the increased activity of NK cells, T cell function is inhibited after antenatal GC treatment. Our data show that GC treatment results in a significant reduction of the capacity of T cells to proliferate in response to incubation with the mitogen PHA in cord blood samples of infants born preterm (gestational age 26-31 wk as well as 32-36 wk). The inhibition of T cell proliferative responses after antenatal treatment with GC is in line with data on rats from Murthy and Moya(25). These authors showed that betamethasone treatment at d 19 and 20 of pregnancy results in significant decreases in splenic T cell proliferative responses in the fetuses at term (on d 21). The inhibitory effect on T cell proliferation could still be observed at d 6 after birth(25).
In the present study, GC did not affect total T cell numbers or numbers of CD4 and CD8 positive T cells. Thus, the reduced proliferative response after prenatal exposure to GC cannot be attributed to GC-induced changes in the cellular composition of the blood samples but is presumably because of interference with the functional capacity of T cells.
In adults, T cell function is known to be inhibited by GC via direct effects on the T cell as well as indirect effects on accessory cells(15,26–29). These indirect effects mainly involve inhibition of production of cytokines like IL-1 and IL-6 by accessory cells that enhance T cell proliferation. However, our data show that the capacity of monocytes to produce IL-6 is not affected by antenatal GC treatment (Table 3), suggesting that monocyte functioning is not altered by the treatment. Therefore, we propose that the effects of GC treatment on T cell reactivity in the newborn are mediated via direct effects on T cell functioning and do not involve accessory cells. Adult T cells express intracellular GC receptors, the triggering of which results in inhibition of IL-2 production and T cell proliferation(28–30). The question arises whether T cells of preterm infants express functional GC receptors. In a previous study, we showed that cord blood T cells of full-term newborns express high-affinity GC receptors. Moreover, we showed that T cells of preterm and full-term newborns are far more sensitive to the acute inhibitory effects of GC than are adult T cells(18,19). During the first year of life, the adult response pattern to GC is acquired(18). Thus, we propose that T cells of human newborns express functional GC receptors and that in vivo binding of GC to these receptors may result in decreased T cell proliferation, as found in the cord blood samples of GC-treated preterms.
Although GC can have direct effects on cells of the immune system, it is also possible that the effects of antenatal GC treatment are mediated via effects of GC on other systems, e.g. the CNS. In rats, it has been shown that exposure to GC early in development can result in changes in the reactivity of the hypothalamus-pituitary-adrenal axis, which is reflected by altered stress levels of corticosterone(4,12,13). The alterations in corticosterone response may, in turn, result in changes in the reactivity of the immune system. In the present study, plasma levels of cortisol in cord blood are significantly lower in the betamethasone-treated individuals than in the untreated controls (Table 5). In general, inhibition of T cell proliferation would be associated with increased cortisol levels. Therefore, we do not expect that the lower plasma cortisol levels we observed are responsible for the observed effects of antenatal betamethasone exposure on immune function.
The question arises whether the effects of antenatal betamethasone on functional activity of the immune system are long-lasting. Therefore, using an ANCOVA model, we analyzed whether the interval between the last treatment and the actual birth of the infant contributed to the observed effects of betamethasone. The results of this analysis showed that the duration of the interval did not contribute significantly to the effects observed (data not shown). Therefore, we can conclude that the effects on the immune system do indeed last for at least weeks.
In summary, antenatal GC treatment accelerates NK cell activity in very preterm newborns. In the first defense against viruses, NK cell activity is of major importance. Therefore, GC-induced accelerated maturation of NK cells may be beneficial beneficial for the very preterm newborn. In contrast, however, treatment with GC results in decreased T cell proliferative proliferative responses. Impaired T cell responses can be associated with inappropriate cellular immune responses that may be harmful for the newborn. We conclude that the beneficial effects of antenatal GC treatment on lung function of the preterm newborn are accompanied by adverse effects on T cell function. Currently, we are following-up the infants through the first years of life to get more insight into possible effects later in life.
Abbreviations
- GC :
-
glucocorticoids
- NK :
-
natural killer
- PHA :
-
phytohemagglutinin
- LPS :
-
lipopolysaccharide
- SGA :
-
small for gestational age
- LGA :
-
large for gestational age
- AGA :
-
appropriate for gestational age
References
Liggins G, Howie R 1972 Prevention of respiratory distress syndrome in premature infants by antepartum glucocorticoid treatment. Pediatrics 50: 515–525.
Crowley P, Chalmers I, Keirse MJNC 1990 The effects of corticosteroid administration before preterm delivery: an overview of the evidence from controlled trials. Br J Obstet Gynaecol 97: 11–25.
Crowley PA 1995 Antenatal corticosteroid therapy: a meta-analysis of the trials, 1972 to 1995. Am J Obstet Gynecol 173: 322–334.
De Kloet ER, Rosenfeld P, Van Eekelen JAM, Sutanto W, Levine S 1988 Stress, glucocorticoids, and development. In: Boer GJ, Feenstra MGP, Mirmiran M, Swaab DF, Van Haaren F (eds) Progress in Brain Research, Vol. 73. Elsevier Science Publishers, Amsterdam, 101–120.
Bian X, Seidler FJ, Slotkin TA 1993 Fetal DEX exposure interferes with establishment of cardiac noradrenergic innervation and sympathetic activity. Teratology 47: 109–117.
Derks JB, Mulder EJH, Visser GHA 1995 The effects of maternal betamethasone administration on the fetus. Br J Obstet Gynaecol 102: 40–46.
Schmand B, Neuvel J, Smolders-De Haas H, Hoeks J, Treffers PE, Koppe JG 1990 Psychological development of children who were treated antenatally with corticosteroids to prevent respiratory distress syndrome. Pediatrics 86: 58–64.
Smolders-De Haas H, Neuvel J, Schmand B, Treffers PE, Koppe JG, Hoeks J 1990 Physical development and medical history of children who were treated antenatally with corticosteroids to prevent respiratory distress syndrome: 10-12 year follow-up. Pediatrics 86: 65–70.
Cote JC, Meuwissen HJ, Pickering RJ 1974 Effects on neonate of prednisone and azathioprine administered to mother during pregnancy. J Pediatr 85: 324–328.
Eishi Y, Hirokawa K, Hatakeyama S 1983 Long-lasting impairment of immune and endocrine systems of offspring induced by injection of dexamethasone into pregnant mice. Clin Immunol Pathol 26: 335–349.
Levine Ross J, Schulte HM, Galucci WT, Cutler GBJ, Loriaux DL, Chrousos GP 1986 Ovine corticotropin-releasing hormone stimulation test in normal children. J Clin Endocrinol Metab 62: 390–392.
Bakker JM, Donne-Smidt E, Kavelaars A, Heijnen CJ, Tildres FJH, Van Rees EP 1995 Effects of short-term dexamethasone treatment during pregnancy on the development of the immune system and the hypothalamo-pituitary adrenal axis in the rat. J Neuroimmunol 63: 183–192.
Bakker JM, Donne Schmidt E, Kroes H, Kavelaars A, Heijnen CJ, Tilders FJH, Van Rees EH 1997 Effects of neonatal dexamethasone treatment on hypothalamo-pituitary-adrenal axis and immune system of the rat. J Neuroimmunol 74: 69–76.
Lew W, Oppenheim JJ, Matsushima K 1988 Analysis of the suppression of IL-1 alpha and IL-1 beta production in human peripheral blood mononuclear adherent cells by a glucocorticoid hormone. J Immunol 140: 1895–1902.
Waage A, Slupphag G, Shalaby R 1990 Glucocorticoids inhibit the production of interleukin-6 from monocytes, endothelial cells, and fibroblasts. Eur J Immunol 20: 2439–2443.
Gillis S, Wong-Staal F, Crabtree GR, Smith KA 1994 Glucocorticoid-induced inhibition of T cell growth factor production. I. The effects on mitogen-induced lymphocyte proliferation. J Immunol 123: 1624–1629.
Wyllie AH 1979 Glucocorticoid-induced thymocyte apoptosis is associated with endogenous endonuclease activation. J Immunol 123: 1624–1631.
Kavelaars A, Cats B, Visser GHA, Zegers BJM, Bakker JM, Van Rees EP, Heijnen CJ 1996 Ontogeny of the response of human peripheral blood T cells to glucocorticoids. Brain Behav Immun 10: 288–297.
Kavelaars A, Zijlstra J, Bakker JM, Van Rees EP, Visser GHA, Zegers BJM, Heijnen CJ 1995 Increased dexamethasone sensitivity of neonatal leukocytes: different mechanisms of glucocorticoid inhibition of T cell proliferation in adult and neonatal cells. Eur J Immunol 25: 1346–1351.
Hand DJ, Taylor CC 1993 Multivariate Analysis of Variance and Repeated Measures. A Practical Approach for Behavioural Scientists. Chapman & Hall, London, 109–145.
Liggins GC 1994 The role of cortisol in preparing the fetus for birth. Reprod Fert Dev 61: 141–150.
Barnes P, Jacobs M, Roberts JM 1984 Glucocorticoids preferentially increase fetal alveolar -adrenoreceptors: autoradiographic evidence. Pediatr Res 18: 1191–1194.
Schedlowski M, Jacobs R, Stratmann G, Richter S, Hadicke A, Tewes U, Wagner TOF, Schmidt RE 1993 Changes of natural killer cells during acute psychological stress. J Clin Immunol 13: 118–126.
Benschop RJ, Oostveen FG, Heijnen CJ, Ballieux RE 1993 Beta 2-adrenergic stimulation causes detachment of natural killer cells from cultured endothelium. Eur J Immunol 23: 3242–3247.
Murthy KK, Moya FR 1994 Effect of betamethasone on maternal, fetal, and neonatal rat cellular immunity. Early Hum Dev 36: 1–11.
Cupps TR, Fauci AS 1982 Corticosteroid-mediated immunoregulation in man. Immunol Rev 65: 133–155.
Waage A, Bakke O 1988 Glucocorticoids suppress the production of tumor necrosis factor by lipopolysaccharide-stimulated human monocytes. Immunol 63: 299–302.
Paliogianni F, Raptos A, Ahuja SS, Najjar SM, Boumpas DT 1993 Negative transcriptional regulation of human interleukin 2 (IL-2) gene by glucocorticoids through interference with nuclear transcription factors AP-1 and NF-AT. J Clin Invest 91: 1481–1489.
Northrop JP, Crabtree GR, Mattila PS 1992 Negative regulation of interleukin-2 transcription by the glucocorticoid receptor. J Exp Med 1755: 1235–1245.
Lew W, Oppenheim JJ, Matsushima K 1988 Analysis of the suppression of IL-1 and IL-1 production in human peripheral blood mononuclear adherent cells by a glucocorticoid hormone. J Immunol 140: 1892–1902.
Acknowledgements
The authors thank Jitske Zijlstra, Anita Meijer, and Ilse de Koe for excellent technical assistance. We also thank Dr. J.A.J. Faber for biostatistical advice and the nursing staff of the Department of Obstetrics of the Academic Hospital, Utrecht, for impressive support.
Author information
Authors and Affiliations
Additional information
Supported by “Het Praeventiefonds” grants 28-2198 and 28-2197.
Rights and permissions
About this article
Cite this article
Kavelaars, A., van der Pompe, G., Bakker, J. et al. Altered Immune Function in Human Newborns after Prenatal Administration of Betamethasone: Enhanced Natural Killer Cell Activity and Decreased T Cell Proliferation in Cord Blood. Pediatr Res 45, 306–312 (1999). https://doi.org/10.1203/00006450-199903000-00003
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199903000-00003
This article is cited by
-
Antenatal Steroids and Cord Blood T-cell Glucocorticoid Receptor DNA Methylation and Exon 1 Splicing
Reproductive Sciences (2022)
-
Antenatal corticosteroid administration is associated with decreased growth of the fetal thymus: a prospective cohort study
Journal of Perinatology (2020)
-
Prenatal Betamethasone interferes with immune system development and alters target cells in autoimmune diabetes
Scientific Reports (2019)
-
Dichotomous development of the gut microbiome in preterm infants
Microbiome (2018)
-
Antenatal endogenous and exogenous glucocorticoids and their impact on immune ontogeny and long-term immunity
Seminars in Immunopathology (2016)
