
Abstract
There is a growing body of literature that describes the use of dual-energy x-ray absorptiometry (DXA) for bone mineral content (BMC) and fat mass (FM) assessment in neonates, but the reproducibility and accuracy of the method are still controversial. Two different software programs have been developed for use on Hologic densitometers: the Pediatric Whole Body (PWB) and the Infant Whole Body (IWB) programs. They differ in scan time, radiation exposure, and in the algorithm used to assess BMC. We evaluated the reproducibility and accuracy of PWB and IWB in newborn piglets. Reproducibility of body mass (BM), FM, and BMC measurements from PWB and IWB were similar. BM agreed well with scale weight with both software programs; IWB was within ± 0.5% and PWB was within ± 0.3% of scale weight. FM was highly correlated with carcass fat (PWB:r= 0.962; IWB:r= 0.980). Errors in the DXA estimation of fat were similar with PWB and IWB. With both software programs, BMC was highly correlated with carcass calcium (PWB:r= 0.925, IWB:r= 0.987), but errors in the DXA estimation of calcium were about twice as high with PWB (±16.9%) than with IWB (±9.2%). In four piglets, the addition of a layer of porcine lard was associated with an increase in BMC; this effect was more pronounced with PWB (+156%) than with IWB (+15%). The IWB software provided BMC measurements that were more precise, accurate, and stable in the presence of added fat than the measurements obtained with PWB, indicating that IWB is superior to PWB for in vivo determination of BMC and body composition.
Similar content being viewed by others

Main
DXA is capable of measuring BM and whole body composition in preterm and term infants (1). However, controversy still surrounds the reproducibility and accuracy of DXA measurements in neonates. Reproducibility relates to the number of infants who must be assessed to detect a significant effect in nutritional studies. Accuracy is directly related to the reliability of the results provided by DXA systems.
The accuracy of DXA measurements of BMC has been shown in adult-sized animal models (2–4). There was an excellent correlation between BMC and total body calcium determined by in vivo neutron activation analysis (5). In large pigs, there was a highly significant correlation between FM measured by DXA and chemical fat extraction (r> 0.98) (3, 4, 6). In newborn piglets (less than 6 kg) scanned with DXA equipment, whole-body BMC assessment has consistently demonstrated its high quantitative accuracy (7–9). The first reliability study in piglets compared BMC with total ash weight (7). However, in our first study we showed that the determination of whole-carcass calcium content was more appropriate than total ash weight as a measurement to show the accuracy of BMC assessment by DXA (8). There was a close correlation between FMf and chemical determinations of body fat, but whole-carcass fat content was generally overestimated (7–9), indicating the need for a correction formula (8). For Hologic densitometers, two software programs have been developed: the PWB program (7, 10) and the more recently developed IWB program (8, 11, 12). Scanning time, radiation exposure, and BMD detection thresholds differ between the two programs. Furthermore, an infant table pad was used during the IWB scans; this pad was not used during measurements with the PWB software. Results reported in preterm and term human infants appear to differ between PWB (10, 13) and IWB (8, 11, 14).
The aim of the present study was to use young piglets to evaluate the reproducibility and accuracy of the two programs.
METHODS
Study design.
Seven piglets (Landrace × Pieltrain) less than 1 month old were selected to represent the range of body weights in human neonates (1430–5180 g). After 12 h without food, the piglets were given an overdose of pentobarbital (300 mg/kg body weight) according to a protocol approved by the veterinary school of the University of Liege. To increase the range of fat content, layers of porcine lard 0.3 cm thick were applied around the abdomen in four of the piglets, providing 11 different study subjects. For DXA measurements, two different configurations of whole-body densitometers were used. Finally, whole-carcass chemical analysis was performed to evaluate the accuracy of the DXA measurements.
DXA measurements.
To measure DXA, we used two different configurations of whole-body densitometer by Hologic (Hologic Inc, Waltham, MA). The first DXA measurement was taken in Lyon, within 2 h of death. The piglets were measured with a QDR 1000W equipped with the PWB software. The piglets were then frozen and transported to Liege, where they were thawed and scanned with a QDR 2000 equipped with the IWB software. It has been shown previously that freezing and thawing do not influence DXA measurements (7). Animals were examined in a similar prone position in Lyon and Liege, by the same researcher (J.C.P.) (Fig. 1). Subsequently, whole-carcass chemical analysis was performed. QDR 1000W and QDR 2000 densitometers use the same scanning technology, and it has been reported that BMC and FM measurements from the two systems are comparable (14). For all measurements, whole-body scanners in single-beam mode were used. DXA analysis gave measurements of BA (cm2), BMD (g/cm2), FM (g, %), and LM (g). From these measurements, BMC (= BMD/BA) (g) and BM (= LM + BMC + FM) (g) were calculated with the system software. The term “bone mineral density” is the expression used by the software and is generally recognized in DXA literature. Subjects scanned with IWB were laid out on an infant table pad specifically designed for whole-body measurements of human infants up to 1 y of age. It filters the low-energy beam to improve system linearity in small subjects and to reduce the radiation dose (11). The dose was lowered from 0.7 mRem (10) (0.1 mRem = 1 μsV) to 0.3 mRem (11), which is much lower than the dose used for neonate chest x-rays (10 mRem) (10) and is well below other common radiographic procedures. Scan time was 10 min for PWB and 6 min for IWB. The bone detection threshold was lower with IWB (0.05–0.15 g/cm2) than with PWB (0.25 g/cm2). All piglets were scanned 3 times consecutively without repositioning to evaluate DXA reproducibility. From these data, the CV% of the various DXA measurements was calculated.

DXA scans using Infant Whole Body and Pediatric Whole Body programs in the same piglet (body weight = 1980 g).
Electronic scale and whole-carcass chemical analysis.
The piglets were weighed before and after the DXA scan, and mean body weight was compared with the DXA-measured BM. After the DXA scan in Liege (Belgium), a whole-body chemical analysis was performed on each piglet to assess the accuracy of BMC and fat DXA measurements. The whole carcass was homogenized as previously described (8). The total fat content of the homogenized carcass was determined by chemical fat extraction (6-g samples, in triplicate) with chloroform-methanol (15). The CV of the chemical fat measurement was 3.0 ± 1.7%. Total calcium content was determined by atomic absorptiometry after the whole carcass samples had been reduced to ash at 550°C for at least 24 h, until only a fine powder remained. Mean CV (±SD) of chemical calcium determinations was 4.6 ± 3.0%.
Statistical analysis.
The Wilcoxon signed rank test was used for the comparison of DXA results obtained with PWB and IWB;p< 0.05 was considered significant. Reproducibility was calculated as the CV% from triplicate DXA measurements. Linear regression analysis and Pearson product moment correlation coefficient (r) were used to compare DXA measurements with carcass analysis. As in our previous study, data conversion was calculated to assess DXA accuracy (16). Conversion formulas for BM, BMC, and FM were generated by the linear relationship between the reference data (scale BW, carcass fat, and carcass calcium) and DXA estimation. The dispersion around the regression line represents the error of estimation and can be expressed as the difference between the corrected DXA value and the reference value in terms of percentage of the reference value. All data were given as the mean ± 1 SD.
RESULTS
Mean scale body weight of the piglets was 1431–5179 g. As measured by chemical analysis, calcium content ranged between 11 and 40 g, and fat content was 54–770 g (3.8–14.9% body weight) and increased up to 1424 g (24%) in fat-padded piglets.
Reproducibility of BM, FM, and BMD measurements was similar with IWB (mean CV% = 0.1%, 6.8%, and 1.9%) and PWB (mean CV% = 0.1%, 5.5%, and 1.5%). Mean CV% of BA and BMC measurements were lower with IWB (1.1% and 2.3%) than with IWB (4.7% and 4.1%), but the difference was statistically significant only for BA (p= 0.03). The reproducibility of BMC measurements improved with increased BMC (Fig. 2A). This was statistically significant for IWB (r= 0.93, p= 0.002) but not for PWB (r= 0.36, p= 0.428). The reproducibility of FM measurements improved significantly with increased FM only for IWB (IWB, r= 0.69, p= 0.02; PWB, r= 0.52, p= 0.10) (Fig. 2B).

Reproducibility of DXA measurement using the Pediatric Whole Body program (dark circles) or Infant Whole Body program (open circles). (A) Reproducibility of bone mineral content measurement in seven piglets. (B) Reproducibility of FM measurement in 11 (7 + 4 fat-padded) piglets. Squares are fat-padded piglets. The dotted line represents the identity line for PWB, and the solid line represents the identity line for IWB.
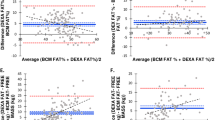
Between PWB and IWB, the BM, BA, BMD, and LM values measured in seven piglets were significantly different (Table 1). There was a close correlation between BW and BM with both IWB [BM (g) = 0.996 × BW (g) − 5.9, r= 0.999, p= 0.0001] and PWB [BM (g) = 0.989 × BW (g) − 28.4, r= 0.999, p= 0.0001] (Fig. 3A). Body weight was slightly underestimated by DXA, but values measured with IWB were closer to scale BW than values measured with PWB. However, the error of estimation was very small with both PWB (±0.3%) and IWB (±0.5%) (Fig. 3B).

Body weight assessment by DXA using the Pediatric Whole Body (dark circles) or Infant Whole Body program (open circles) in seven piglets. (A) Relationship between scale body weight and DXA body mass. (B) Error of body weight estimate by DXA (absolute values). Dotted line represents the identity line for PWB, and solid line represents the identity line for IWB.
Bone area was significantly higher with IWB than with PWB, in contrast to BMD, which was significantly lower with IWB than with PWB. As a result, BMC measurements (estimated as BMD × BA) from IWB and PWB were similar (Table 1). There was a significant correlation between BMC and carcass Ca [IWB: BMC (g) = 2.0 × Ca (g) + 1.8, r= 0.99, p= 0.0001; PWB: BMC (g) = 2.3 × Ca (g) − 5.3, r= 0.93, p= 0.003] (Fig. 4A). From these values, calcium content can be estimated from BMC as DXA Ca (g) = 0.5 × BMC (g) + 0.25 for IWB and DXA Ca (g) = 0.4 × BMC (g) + 5.4 for PWB. The error of estimation for whole-carcass calcium content with IWB was nearly twice as low (± 9%) as with PWB (± 16.9%) (Fig. 4B).

Whole-carcass calcium content assessment by DXA using the Pediatric Whole Body program (dark circles) or Infant Whole Body program (open circles) in seven piglets. (A) Relationship between chemical calcium and DXA BMC. (B) Error of whole-carcass calcium estimate by DXA (absolute values). Squares are fat-padded piglets. Dotted line represents the identity line for PWB, and solid line represents the identity line for IWB.
To determine the influence of increased fat content on the BMC assessment, we analyzed the two sets of data obtained from piglets with, and from those without, the layers of porcine lard. There was an increase of BA and BMD in fat-padded piglets compared with those without a layer of porcine lard (Fig. 5). The mean increase in BA was +7% (IWB) and + 121% (PWB). It was similar for BMD: +7.5% (IWB) and +8.3% (PWB). As a result, the mean increase in BMC was +15% (IWB) and +155% (PWB).

Effect of added porcine lard on whole-body mineralization assessment by DXA in piglets scanned with the Pediatric Whole Body (dark bars) or Infant Whole Body (white bars) program. (*) Significantly different (p< 0:05).
Mean DXA FM was measured in 11 subjects (7 + 4 fat-padded). No statistically significant difference could be detected between IWB and PWB (415 ± 267 g vs 409 ± 278 g, p= 0.53). FM was highly and similarly correlated with chemical fat content in both software programs (IWB:r= 0.98; PWB:r= 0.96) (Fig. 6A). The error of estimation for fat was similar: 40% with IWB and 41% with PWB. It decreased with increased fat content in both software programs (Fig. 6B).

Whole-carcass fat content assessment by DXA using the Pediatric Whole Body (dark circles) or Infant Whole Body program (open circles) in 11 piglets (7 + 4 fat-padded). (A) Relationship between chemical fat and DXA FM. (B) Error of whole-carcass fat estimate by DXA (absolute values). Squares are fat-padded piglets. Dotted line represents the identity line for PWB, and solid line represents the identity line for IWB.
DISCUSSION
The assessment of whole-body BMC and FM by DXA is a rapid and safe technique that could become widely used in the evaluation of nutritional status and growth in neonates (1, 17). The reliability of DXA measurements from Hologic scanners has been evaluated in newborn piglets, using whole-body chemical analysis as the reference method (7, 8, 11). Recently, we used a QDR 2000 with the IWB software to evaluate BMC in preterm and term infants shortly after birth (12). We showed that BMC was close to reference values previously reported from carcass analysis and neutron activation (18). Similar observations were obtained for whole-body FM (12) after correction of DXA overestimation by means of data from our validation study on newborn piglets. The current position is that most of the DXA data reported in preterm and term infants have been determined with Hologic QDR 1000W or QDR 2000 DXA scanners, using PWB or IWB, with or without the infant table pad. Many studies have compared DXA with other methods that are not considered the gold standard for BMC or FM assessment in newborns. At present, DXA whole-body phantoms that give reliable cross-calibration for BMC and soft tissue results are not available. Therefore, animal studies remain the only way to evaluate DXA measurements (7–9, 11).
Software-related differences were observed for bone mineral assessment (BA, BMD), LM, and BM (Table 1). IWB was more precise and more accurate than PWB. The reproducibility of IWB BMC measurements was high and improved with increased BMC. Whole-carcass calcium DXA estimates were about twice as accurate with IWB (± 9.2%) than with PWB (±16.9%). The higher BA values observed with IWB can be explained by differences in the threshold used for bone detection between PWB and IWB. According to the manufacturer, IWB software uses in its analysis a dynamically adjusted bone detection threshold that is lower (0.05–0.15 g/cm2) than the PWB threshold (0.25 g/cm2) (11). The addition of porcine lard dramatically influenced BA and BMC estimation with PWB. Although the reason for this effect needs further examination, we cannot exclude the effect of interface interference caused by the addition of the layer of porcine lard, which was an experimental artifact in our measurement system. The direct influence of body FM on the accuracy of BMC cannot be evaluated in the present study. However, a higher degree of differentiation was observed with IWB than with PWB, and the change in BA value was lower with IWB than with PWB. In our previous study with IWB, the error of estimation in calcium content was 4.4% in 13 piglets (8). Compared with reference values obtained with neutron activation (19) and chemical analysis (20), whole-body calcium content was accurately estimated in vivo, independent of FM content, in preterm and term infants at birth (12, 18).
Whole-body fat assessment by DXA was less reproducible and accurate than BMC assessment. The reproducibility and accuracy of FM measurement were very similar with PWB and IWB. Accuracy improved with increased fat content of piglets, but a correction equation was needed. The following formula was calculated for IWB measurements: corr DXA fat (g) = [−101 + 1.21 DXA fat (g)] × (DXA fat < 569 g) + [162 + 0.79 DXA fat (g)] × (DXA fat > 569 g), r= 0.99 (12). Because we have observed in the present study that FM values measured with IWB and PWB were similar, the previous correction formula can be applied to PWB measurements.
DXA is probably the best technique available for body composition assessment in small subjects at the present time. We have shown that FM measured by DXA in preterm and term infants was close to the reference values obtained from cadaver analysis (12, 18). Other techniques such as total-body electrical conductivity, bioelectrical impedance analysis, and isotope dilution techniques are indirect methods measuring total body water. Calculation of lean body mass from total body water is based upon the assumption of a fixed hydration factor of fat-free mass, which is not appropriate in neonates. Therefore, the accuracy of individual fat estimates by these indirect methods is relatively poor. In a 3500-g term infant, an error of 5% in fat-free mass corresponds to an error of 30% in calculated FM (21), which is much more than the 12% error we calculated for DXA (8). We have previously shown that FM assessment by DXA (IWB) is not influenced by LM hydration factor (8).
The authors conclude that in newborn piglets, DXA was more accurate for whole-body mineralization assessment than for whole-body FM assessment. IWB measurements of bone mineral content were more reproducible and accurate than PWB measurements, and they were less influenced by fat content. A correction formula was developed for fat assessment in small subjects for the IWB software. DXA values in human neonates have to be compared with reference data obtained with the same software. At the time of writing, reference curves for BMC (11, 12) and FM (12) have been published only for IWB software. For these reasons and because of lower radiation exposure and shorter scan times, the IWB software is recommended for clinical use in newborns and infants.
Abbreviations
- DXA:
-
dual energy x-ray absorptiometry
- BMC:
-
bone mineral content
- FM:
-
fat mass
- QDR:
-
quantitative digital radiology
- BMD:
-
bone mineral density
- PWB:
-
pediatric whole body software
- IWB:
-
infant whole body software
- BM:
-
body mass
- LM:
-
lean mass
- BW:
-
body weight
- CV%:
-
coefficient of variation
- BA:
-
bone area, Ca, calcium
References
Specker BL, Beck A, Kalkwarf H, Ho M 1997 Randomized trial of varying mineral intake on total body bone mineral accretion during the first year of life. Pediatrics 99: 1–7
Mitchell AD, Conway JM, Scholz AM 1996 Incremental changes in total and regional body composition of growing pigs measured by dual-energy x-ray absorptiometry. Growth Dev Aging 60: 95–105
Svendsen OL, Haarbo J, Hassager C, Christiansen C 1993 Accuracy of measurements of body composition bu dual-energy x-ray absorptiometry in vivo. Am J Clin Nutr 57: 605–608
Mitchell AD, Conway JM, Potts WJE 1996 Body composition analysis of pigs by dual-energy x-ray absorptiometry. J Anim Sci 74: 2663–2671
Ellis KJ, Shypailo RJ, Hergenroeder A, Perez M, Abrams S 1996 Total body calcium and bone mineral content: comparison of dual-energy x-ray absorptiometry with neutron activation analysis. J Bone Miner Res 11: 843–848
Ellis KJ, Shypailo RJ, Pratt JA, Pond WG 1994 Accuracy of by dual-energy x-ray absorptiometry for body composition measurements in children. Am J Clin Nutr 60: 660–665
Brunton JA, Bayley HS, Atkinson SA 1993 Validation and application of dual-energy x-ray absorptiometry to measure bone mass and body composition in small infants. Am J Clin Nutr 58: 839–845
Picaud JC, Rigo J, Nyamugabo K, Milet J, Senterre J 1996 Evaluation of dual-energy x-ray absorptiometry for body-composition assessment in piglets and term human neonates. Am J Clin Nutr 63: 157–163
Brunton J, Weiler HA, Atkinson SA 1997 Improvement in the accuracy of dual-energy x-ray absorptiometry for whole-body regional analysis of body composition: validation using piglets and methodologic considerations in infants. Pediatr Res 41: 590–596
Venkataraman PS, Ahluwallia BW 1992 Total bone mineral content and body composition by x-ray densitometry in newborns. Pediatrics 90: 767–770
Koo WWK, Massom LR, Walters J 1995 Validation of accuracy and reproducibility of DXA for infants. J Bone Miner Res 10: 1111–1115
Rigo J, Nyamugabo K, Picaud JC, Gerard P, Pieltain C, De Curtis M 1998 Reference values of body composition obtained by dual-energy x-ray absorptiometry in preterm and term neonates. J Pediatr Gastroenterol Nutr 27: 184–190
Lapillonne A, Braillon P, Claris O, Chatelain PG, Delmas PD, Salle BL 1997 Body composition in appropriate and in small for gestational age infants. Acta Paediatr 86: 196–200
Abrahamsen B, Gram J, Hansen TB, Heck-Nielsen H 1995 Cross calibration of QDR-2000 and QDR-1000 dual-energy x-ray densitometers for bone mineral and soft tissue measurements. Bone 16: 385–390
Folch J, Lees M, Sloane Stanley GH 1957 A simple method for the isolation and purification of total lipids from animal tissues. J Biol Chem 226: 497–509
Bland JM, Altman DG 1986 Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1: 307–310
Wauben IP, Atkinson SA, Grad TL, Paes B 1998 Moderate nutrient supplementation of mother's milk for preterm infants supports adequate bone mass and short-term growth: a randomized, controlled trial. Am J Clin Nutr 67: 465–472
Rigo J, De Curtis M, Picaud JC, Nyamugabo K, Senterre J 1998 Whole body calcium content in term and preterm neonates. Eur J Pediatr 157: 259–260
Ellis KJ, Shypailo RJ, Schanler RJ, Langston C 1994 Body composition of preterm infant. Am Hum Biol 21: 533–545
Widdowson EM 1962 Importance of nutrition in development with special reference to feeding low birth weight infants. In: Sauls HS, Berison JD (eds) Nutritional Goals for Low Birth Weight Infants. Proceedings of the Second Ross Clinical Research Conference 2–3 October 1980, Ross, Columbus, OH, pp 4–11
De Bruin NC, Van Velthoven KAM, Stijnen J, Juttmann RE, Degenhart HJ 1995 Body fat and fat-free mass in infants: new and classic anthropometric indexes and prediction equation compared with total-body electrical conductivity. Am J Clin Nutr 61: 1195–1205
Acknowledgements
The authors thank Thomas Kelly and Geraint Jones for their contribution to the preparation of this manuscript.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Picaud, JC., Nyamugabo, K., Braillon, P. et al. Dual-Energy X-Ray Absorptiometry in Small Subjects: Influence of Dual-Energy X-Ray Equipment on Assessment of Mineralization and Body Composition in Newborn Piglets. Pediatr Res 46, 772 (1999). https://doi.org/10.1203/00006450-199912000-00011
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199912000-00011
