
Abstract
Regional changes of metabolite concentrations during human brain development were assessed by quantitative localized proton magnetic resonance spectroscopy in vivo. Apart from measurements in young healthy adults, the study was based on regional spectra from 97 children who were either healthy or suffered from mental retardation, movement disorders, epilepsies, neoplasm, or vascular malformation. Metabolite quantitation focused on cortical gray and white matter, cerebellum, thalamus, and basal ganglia in six age groups from infancy to adulthood. During infancy and childhood, the concentration of the neuroaxonally located N-acetylaspartate increased in gray matter, cerebellum, and thalamus, whereas a constant level was detected in white matter. These findings are in line with regional differences in the formation of synaptic connections during early development and suggest a role of N-acetylaspartate as a marker of functioning neuroaxonal tissue rather than of the mere presence of nerve cells. This view is further supported by high concentrations of taurine in gray matter and cerebellum during infancy, because taurine is also believed to be involved in the process of synapse formation. Remarkably, in basal ganglia both N-acetylaspartate and taurine remain constant at relatively high concentrations. Other metabolite changes during maturation include increases of N-acetylaspartylglutamate, especially in thalamus and white matter, and a decrease of glutamine in white matter. Despite regional differences and some small changes during the first year of life, the concentrations of creatine, phosphocreatine, choline-containing compounds, myo-inositol, and glutamate remain constant afterward. The creatine to phosphocreatine concentration ratio yields 2:1 throughout the human brain irrespective of region or age. The observed increase of the proton resonance line-width with age is most pronounced in basal ganglia and corresponds to the age-related and tissue-dependent increase of brain iron.
Similar content being viewed by others
Main
The development of the human brain extends over a long period of time. For example, myelination in part proceeds until early adulthood, and synaptic connections are formed continuously throughout life in association with learning processes. On the other hand, the total number of neurons already starts to slowly decline after birth. Some of these processes are accompanied by modulations of major metabolite pools, which may be investigated noninvasively by in vivo MRS. In fact, a variety of previous MRS studies of neonates, infants, and children reported developmental changes of tNAA, tCr, Cho, and Ins (1–14). Although the most pronounced metabolite changes during the first year of life have been addressed in detail (3, 5–7, 11), studies of developmental alterations at later stages were performed without taking regional variations into account or without metabolite quantitation (1, 8, 13). The purpose of this work was to quantify regional adjustments of metabolites during brain development with a special emphasis on the period from early childhood to adolescence.
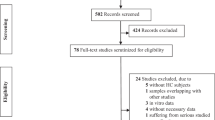
The need for a pediatric database comprising absolute metabolite concentrations arose from our observation of systematic discrepancies between spectral findings in children and those in young adults. Unfortunately, ethical objections hamper the examination of a sufficiently large number of healthy children at different ages and within multiple brain regions (15). We therefore performed a retrospective assessment of 430 of our neuropediatric patients [see (16) for a recent review], based on several selection criteria. Apart from proton MRS studies of healthy children, regional spectra were obtained from patients with unclassified mental retardation, movement disorders, and epilepsies as well as from unaffected brain areas in patients with brain tumors and vascular malformation. Patients with other structural defects were excluded as were children with evidence of a biochemical disorder, an infectious disease or a hypoxic-ischemic condition. In particular, no spectra were taken from children with white matter diseases and mitochondrial disorders.
METHODS
Subjects.
MRS studies of children were approved by the local ethics committee. From a total of 430 neuropediatric patients examined by proton MRS as part of their diagnostic workup, 97 patients were selected who could be classified into one of the following categories:1) children with mental retardation of unknown origin with no progressive clinical course, and without any evidence of metabolic abnormalities;2) patients with ataxia or extrapyramidal movement disorders;3) patients with focal epilepsy, in whom no spectra were taken from regions with a focal disturbance in the EEG (noteworthy, the hippocampus was not part of this study);4) patients with brain tumors; or 5) patients with vascular lesions. In the latter two groups, spectra from unaffected brain areas were included only if the affected tissue was not diffuse but clearly separated from its surrounding. The patients were grouped into five cohorts with ages ranging from 0 to 1 y (n= 11), 1 to 2 y (n= 19), 2 to 5 y (n= 24), 5 to 10 y (n= 17), and 10 to 18 y (n= 26) and supplemented by a group of healthy adult controls aged 18–39 y (n= 72). The composition of each patient group (Table 1) demonstrates that the clinical symptoms are relatively homogeneously distributed across all ages.
Most patients younger than 6 y of age and some older patients were sedated with chloral hydrate and monitored by pulse oximetry throughout the investigation. Before each study written informed consent was obtained from the parents.
Proton MRS.
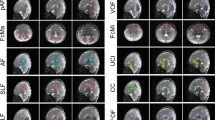
MRS examinations were performed at 2.0-T (Siemens Magnetom SP4000/Vision, Erlangen, Germany) using either the standard imaging head coil or—for children < 20 kg body weight—the extremity coil. VOI positions for localized proton MRS were selected from T1-weighted and in more recent studies also T2-weighted images, as shown in Figure 1. Cortical parietal gray matter (8–18 mL) was measured in a paramedian position spanning 20 mm across the interhemispheric fissure (Fig. 1, A - C ). White matter was investigated mainly in a small VOI (4–5 mL) in parietooccipital locations (Fig. 1, B and D ). The cerebellum (4–8 mL) was examined in a central position covering the vermis (Fig. 1, A and C ). The locations chosen for basal ganglia and thalamus (4–6 mL) are indicated in Figure 1, E and F .

Typical VOI locations selected for localized proton MRS using T1-weighted (A, C–E: three-dimensional spoiled fast low-angle shot, TR/TE = 15 ms/6 ms, flip angle 20°, 4 mm thickness) and T2-weighted MR images (B and F: fast spin echo, TR/TE = 2625 ms/98 ms, 4 mm thickness) of young patients. A–C, Parietal gray matter (10 mL);B and D, Parietooccipital white matter (4.1 mL);A and C, Cerebellum (8 mL) of a patient aged 2 y 8 mo;E and F, Basal ganglia (4.1 mL, anterior VOI) and thalamus (4.1 mL, posterior VOI) of a patient aged 3 y 6 mo.
Fully relaxed, short-echo time proton MR spectra (TR/TE = 6000/20 ms, 64 accumulations) were acquired using a single-voxel STEAM localization sequence with TM = 30 ms (SP4000) or 10 ms (Vision) as described previously (10, 17). Except for a correction of residual eddy-current effects (18), the spectroscopic time-domain data were analyzed without further filtering or baseline processing. Absolute metabolite concentrations were obtained with use of LCModel (S. Provencher, Göttingen, Germany), a user-independent fitting routine based on a library of model spectra of all individual metabolites at known concentration (19). To account for differences in instrument sensitivity between subjects, the MR signal intensities were calibrated in proportion to the actual coil loading by using the transmitter reference amplitude of the MR system (20). Concentrations are expressed as millimolar and are not corrected for CSF contributions and residual T2 relaxation effects. T1 saturation was ignored inasmuch as all experiments were performed under fully relaxed conditions using sufficiently long TR. In this study, we further corrected the size of the spectroscopic volume by a calibration curve that accounts for differences in slice profiles when using different voxel sizes. Because model spectra were recorded with relatively large voxels (15 mL), an underestimation of small volumes would lead to an overestimation of metabolite concentrations. Addition of this correction explains some minor discrepancies between concentrations given here and values reported earlier (15), especially for small volumes in white matter and thalamus.
Accessible metabolites included NAA, NAAG, Cr, PCr, Cho, Ins, Glu, Gln, Tau, GABA, aspartate, Glc, Lac, and scyllo-Ins. Apart from the determination of tNAA and tCr levels, LCModel performs a separate quantitation of NAA and NAAG (21) as well as of Cr and PCr by exploiting the existing, although small, spectral differences. Such attempts benefit from the excellent spectral resolution achieved in most brain regions for children at a young age. Pertinent results provide additional information on age-related metabolic adjustments that contribute to the respective tNAA and tCr levels.
Another feature of LCModel is a zero- and first-order phase correction and the identification of a frequency reference defined by the intense methyl resonances from tNAA, Cho, or tCr. These variables can be used to average original time-domain data across examinations and subjects. Pertinent data have been used mainly for display purposes because mean spectra facilitate a detailed qualitative inspection of regional age dependencies owing to considerable improvements in SNR.
Data analysis.
A quantitative description of metabolite age dependencies was achieved by fitting concentrations c (t) (in millimolar) as a function of age t (in years) to a monoexponential function according to a proposal by Kreis et al. (5) as follows:EQUATION 1 with c0 the adult concentration, c1 the concentration difference to birth, and τ the corresponding time constant. The sum c0 +c1 represents the concentration at birth.

A statistical assessment of differences between age groups was performed with an unpaired t test assuming not necessarily equal variances. Linear correlations, i.e. concentrations versus age or versus other concentrations as well as line-widths versus age, are expressed as rank correlation coefficients, ρ, calculated according to Spearman.
RESULTS
The left column of Figure 2 displays spectra from an 8-mo-old child (gray matter, white matter, and cerebellum) and a 3-y-old child (thalamus and basal ganglia) in comparison with data from young adult control subjects. Visual inspection reveals regional and age differences that are confirmed by quantitative evaluation. Absolute concentrations of major metabolites as well as mean line-widths of the Cr resonance at 3.02 ppm (FWHM) are summarized in Tables 2-Tables 6 for gray matter, white matter, cerebellum, thalamus, and basal ganglia, respectively. In addition, Figure 3 shows scatterplots of regional metabolites that exhibit a pronounced age dependence.

Proton MR spectra from single subjects (STEAM, TR/TE/TM = 6000 ms/20 ms/10 ms, 64 accumulations) representing parietal gray matter (Left, 10 mL, 8 mo;Right, 12.5 mL, 24 y), parietooccipital white matter (Left, 4.1 mL, 8 mo;Right, 4.1 mL, 26 y), cerebellum (Left, 5.1 mL, 8 mo;Right, 8 mL, 27 y), thalamus (Left, 4.1 mL, 3 y 6 mo;Right, 5.1 mL, 38 y), and basal ganglia (Left, 4.1 mL, 3 y 6 mo;Right, 5.1 mL, 38 y). For display purposes only, spectral postprocessing involved zero-filling to 4000 complex data points (2048 ms), Gaussian filtering (half-width 317 ms), and manual phase-correction. All spectra are scaled in proportion.

Scatterplots of selected metabolite concentrations as a function of age in gray matter (Top), white matter (Top middle), cerebellum (Bottom middle), and thalamus (Bottom). The data reveal an age-dependent increase of NAA and a decrease of Tau in gray matter, constant NAA and an increase of NAAG in white matter, an increase of tNAA and a decrease of Tau in cerebellum, and increases of tNAA and NAAG in thalamus.
Gray matter.
Table 2 confirms previous reports that the most pronounced changes of cerebral metabolites with age occur within the first year of life. Compared with older children, our small group of infants reveals lower tNAA concentrations (p< 0.001) as well as lower tCr (p< 0.05) but not PCr levels in gray matter. The concentrations of Ins, Glu, Gln, and GABA remain constant, which also applies to tCr and Cho after 1 y of age. The only metabolites with developmental changes during childhood are NAA and Tau as indicated in Figure 3. In fact, the gradual increase of the concentration of tNAA by about 50% from infancy to adulthood (ρ = 0.65, p< 0.001) entirely reflects an increase of NAA alone expressed by c (t) = 8.80 − 3.14 · exp(−t/2.6), whereas the contribution of NAAG remains very small in gray matter independent of age. The Tau level monotonically decreases with age toward adulthood (ρ = −0.79, p< 0.001) as described by c (t) = 0.90 + 2.46 · exp(−t/10.9).
Many of the quantitative differences in metabolite levels are also well appreciated in mean spectra averaged across subjects within selected age groups. Apart from the alterations of tNAA and tCr, the mean gray matter spectra in Figure 4 show the attenuation of the Tau signal, i.e. the quartet pattern between 3.25 ppm (left shoulder of the Cho resonance) and 3.41 ppm, and also allow the observation of minor metabolites that are difficult to recognize in individual spectra. A prominent example is the unambiguous detection of the doublet resonance of Lac centered at 1.33 ppm (compare Figs. 2 and 4) despite its occurrence atop a broader signal from unknown macromolecular contributions. In gray matter, the mean Lac concentration yields 0.4–0.5 mM in all age groups. Aspartate is identified by the methylene resonance at about 2.8 ppm. Its concentration is constant at about 1.8 mM. GABA is more difficult to observe because its triplet pattern centered at 3.01 ppm is partly obscured by the tCr methyl resonances. Quantitation yields constant values of about 1.6 mM in all age groups. Finally, Glc (3.43 ppm) and scyllo-Ins (3.35 ppm) partly overlap with the quartet resonances of Tau. However, separate concentrations may be determined because of further nonoverlapping resonances at other chemical shifts yielding 1.3 mM for Glc and 0.1 mM for scyllo-Ins.

Mean proton MR spectra (STEAM, TR/TE = 6000 ms/20 ms) representing summed data of parietal gray matter in the age groups 0–1 y (n= 6), 2–5 y (n= 16), 10–18 y (n= 22), and 18–39 y (n= 45). Note the developmental increase of NAA and the decrease of Tau. To demonstrate the excellent SNR of mean spectra, the inset for the age group 2–5 y shows a 4-fold magnification of the 7-Hz doublet resonance from the Lac methyl group atop a broader signal from unknown macromolecular contributions.
White matter.
Age-related changes in parietooccipital white matter are summarized in Table 3 as quantitative metabolite concentrations. Corresponding mean spectra are shown in Figure 5. In apparent similarity to gray matter, the tNAA concentration gradually increases during childhood and adolescence by about 30% (ρ = 0.69, p< 0.001). However, in clear contrast to gray matter, this elevation is entirely related to the steady increase of NAAG given by c (t) = 2.94 − 2.45 · exp(−t/25.6), whereas the concentration of NAA remains constant at 6.1 mM (compare Fig. 3). This effect is also qualitatively recognized by the appearance of an NAAG shoulder of the tNAA resonance in white matter spectra from adults (Fig. 5).

Mean proton MR spectra (STEAM, TR/TE = 6000 ms/20 ms) representing summed data of parietooccipital white matter in the age groups 0–1 y (n= 10), 2–5 y (n= 12), 10–18 y (n= 12), and 18–39 y (n= 61). Note the developmental decrease of Gln (as evidenced by the Glu/Gln methine resonance) and the increase of NAAG.
No developmental changes are observed for tCr (i.e. constant levels of Cr and PCr), Ins, and Glu. The Cho concentration is mildly elevated in infants and young children (0–5 y, 1.86 ± 0.21 mM) and then slowly decreases to adult levels (5–39 y, 1.63 ± 0.22 mM;p< 0.001). The Gln concentration in white matter equals that in gray matter during early infancy. However, although Gln stays constant in gray matter, its level decreases in white matter by a factor of two toward adulthood (ρ = −0.49, p< 0.001). This age-dependent decrease is qualitatively confirmed by inspection of mean spectra showing reduced Gln contributions in spectra of adult control subjects in both the methylene (about 2.4 ppm) and methine (about 3.75 ppm) regions where Glu and Gln resonances overlap. Both Tau and GABA gradually decrease from relatively high concentrations in infants toward very low values in adults.
Cerebellum.
Although the number of cerebellar spectra from children is limited because of the preference of cerebral MRS locations in our patient population, developmental metabolite alterations during infancy and childhood are observed for tNAA, Ins, and Tau as indicated in Table 4 and visualized in Figures 3 and 6. The increase of tNAA (ρ = 0.60, p< 0.001) is caused by increases of both NAA and NAAG and may be described by c (t) = 7.93 − 3.84 · exp(−t/2.6). As in gray matter, the elevation of NAA is accompanied by a decrease of the Tau level by at least a factor of two (ρ = −0.80, p< 0.001) according to c (t) = 1.57 + 2.72 · exp(−t/10.1). In fact, in all age groups the cerebellum has the highest Tau concentration compared with any of the other brain regions investigated.

Mean proton MR spectra (STEAM, TR/TE = 6000 ms/20 ms) representing summed data of cerebellum in the age groups 0–1 y (n= 3), 2–5 y (n= 3), 10–18 y (n= 3), and 18–39 y (n= 19). Note the developmental increase of tNAA and the decrease of Tau and Ins.
The concentrations of tCr, Cho, Glu, Gln, and GABA remain constant from infancy to adulthood, but Ins gradually decreases with age (ρ = −0.58, p< 0.001). This observation again differs from findings in cortical gray and white matter. A further discrepancy emerges from the fact that the mean resonance line-width does not increase with age. Instead, even the spectra of young children are already characterized by a relatively large line-width of > 4 Hz (at 2.0 T), whereas gray and white matter show excellent spectral resolution during infancy and childhood. In those regions, line-widths of 2.5–3 Hz become only mildly degraded during adolescence and adulthood (line-widths of 3.5 Hz, compare Tables 2-Tables 4).
Thalamus.
Metabolite concentrations and mean spectra of thalamus are available for four age groups in Table 5 and Figure 7, respectively. In early infancy, the concentrations of tCr and Tau are elevated in comparison with constant levels in children and adults, but the differences do not reach significance because of the small number of subjects in our infant group. The developmental increase of tNAA according to c (t) = 9.14 − 4.52 · exp(−t/2.8) is similar to that in the cerebellum. It reflects an increase of both NAA and NAAG, i.e. mainly of NAA during early childhood and mainly of NAAG during adolescence, as expressed by its larger time constant in c (t) = 3.58 − 2.83 · exp(−t/15.8) and illustrated in Figure 3. For Cho, Ins, Glu, Gln, and GABA with slightly scattering concentrations, no clear age dependence is discernible.

Mean proton MR spectra (STEAM, TR/TE = 6000 ms/20 ms) representing summed data of thalamus in the age groups 0–1 y (n= 3), 2–5 y (n= 7), 10–18 y (n= 5), and 18–39 y (n= 44). Note the developmental increase of tNAA and decrease of tCr.
As in gray and white matter, the spectral resolution in thalamus decreases with age (compare Fig. 7 with Figs. 4 and 5). Although the effect is more pronounced than in cortical regions, adult spectra still have an acceptable mean line-width of about 5.4 Hz, which allows a reliable quantitation of metabolite concentrations with use of the present methodology.
Basal ganglia.
Age-related metabolite concentrations and mean spectra of basal ganglia ranging from infants to adolescents are indicated in Table 6 and Figure 8, respectively. In contrast to thalamus, adult spectra in basal ganglia are generally so broad as to preclude a reliable quantitation of metabolite concentrations. An exception is the spectrum from a 38-y-old volunteer shown in Figure 2 which exhibits line-widths that are clearly below average. The scatterplot in Figure 9 demonstrates a strong linear increase of the spectral line-width in basal ganglia with age (ρ = 0.89, p< 0.001).

Mean proton MR spectra (STEAM, TR/TE = 6000 ms/20 ms) representing summed data of basal ganglia in the age groups 0–1 y (n= 3), 2–5 y (n= 13), and 10–18 y (n= 5). Apart from the increased line-widths, the spectra reveal no metabolic changes.

Scatterplot of the mean resonance FWHM from proton MR spectra of basal ganglia as a function of age indicating a strong linear correlation.
Although the resonance line-widths increase, the actual metabolite concentrations of tCr, tNAA, Cho, Ins, Glu, and Gln remain constant during development. The age dependence in basal ganglia that we reported in a preliminary study (22) arose from the failure to distinguish between spectra from basal ganglia and thalamus. Spectra from basal ganglia belonged mainly to young children, whereas in adolescents and adults more spectra from thalamus were measured, which accidentally suggested an age dependence of tCr, tNAA, and Gln.
As a result of decreasing spectral resolution, the accuracy for determining minor metabolites such as Tau and GABA also diminishes with age. But despite larger SD in older age groups, the mean concentration of GABA remains constant at a high level of 2.5 mM. Also, Tau remains constant around 1.8 mM in contrast to its decrease observed in all other brain regions.
DISCUSSION
Detailed knowledge about the regional age dependence of brain metabolites is indispensable for a correct interpretation of proton MRS examinations in a pediatric patient population. It is a prerequisite for an assessment of true metabolic disturbances and, in a broader sense, may contribute to a better functional understanding of MRS-detectable metabolites. Although the determination of age-dependent metabolite levels from healthy children will always be preferable, the present study of a selected group of neuropediatric patients gives a clear impression of developmental changes of brain metabolites from infancy to adulthood. This is also supported by the observation that the standard deviations of the resulting metabolite levels are very similar in the patient and control groups and the finding that regional developmental changes are observed for only a few metabolites with most other concentrations remaining constant, i.e. identical to those obtained for a large number of young healthy adults.
NAA and NAAG.
An increase of tNAA is observed in all investigated brain regions with the exception of the basal ganglia. However, NAA and NAAG are distinct with respect to their regional developmental changes. For instance, in gray matter NAA increases and NAAG remains low, whereas the opposite is true for white matter, which shows a constant level of NAA and an increase of NAAG.
The observed elevation of NAA in gray matter, cerebellum, and thalamus occurs mainly during the first few years of life, yielding correspondingly small exponential time constants of 2.5–2.8 y. NAA is considered a neuronal marker (23–25), but its increase during infancy and early childhood cannot be explained by a respective increase in the number of neurons inasmuch as these start to decrease shortly after birth. Instead, because NAA is not only present in neuronal cell bodies, but also in axons, dendrites, and synaptic terminals (24), the observed increase might be explained by the formation of dendritic arborizations and synaptic connections as suggested before for a developmental increase of tNAA without distinguishing between NAA and NAAG (1, 8). In this view, NAA is taken as a marker of functioning neurons rather than as a mere indicator of the presence of nerve cells. In fact, the NAA increase in cortical gray matter, cerebellum, and thalamus corresponds to the wealth of synaptic connections in these brain regions. In complementary fashion, the constant concentration of NAA in white matter is in line with its relative poverty of synaptic connections. The constant NAA level in basal ganglia seems surprising, but the basal ganglia do not have such a prominent function in synaptic transmission as the thalamus (26).
During development, the concentration of NAAG increases, especially in thalamus and white matter. This enhancement is much slower than the NAA increase as indicated by time constants of 15–25 y. Also, animal studies revealed an increase of NAAG with age, being more pronounced in cerebellum and brain stem than in the cerebrum (27). Here, an increase in the central cerebellum is observed, although the effect might be larger in the cerebellar hemisphere because this region has the highest NAAG concentration in adults (15).
NAAG is assumed to be located exclusively in neurons but generally not in the same nerve cells as NAA (24, 25). This distinction between NAA and NAAG with respect to location and function is supported by our observations of regional and temporal differences of their respective developmental increases. So far, the link between the NAAG increase in white matter and its assumed function in neurotransmission remains unclear (23–25, 28).
Cr and PCr.
Because no developmental changes occur for tCr after the age of 1 y, the regional differences reported for adults (15) also apply to children and adolescents. The highest concentration of tCr is found in the cerebellum, followed by basal ganglia, thalamus, gray matter, and white matter. During the first year of life, the tCr concentration increases in gray matter by approximately 15% and decreases in thalamus by almost 20%, whereas the levels in cerebellum and basal ganglia remain high from infancy to adulthood.
The amount of tCr is often interpreted in terms of energy metabolism. This understanding reflects the roles of its two components, Cr and PCr, which are in exchange via the creatine kinase-catalyzed phosphate transfer between ADP and ATP. Thus, the high concentration of tCr in cerebellum has tentatively been connected with the distribution of creatine kinase in this tissue (15). The high tCr level in the basal ganglia and thalamus of infants is in agreement with corresponding data from autopsy material from term infants (7).
The ability to separately quantify Cr and PCr levels strongly depends on the achievable spectral resolution and SNR. These conditions are best met in cortical gray matter, as evidenced by the small SD and the high reproducibility of the Cr and PCr concentrations in Table 2. Noteworthy, and in contrast to an earlier study reporting a 2-fold increase of PCr between infants and adults (29), the evaluation yields constant PCr levels in all tissue types, e.g. about 2.2 mM in gray matter and 3.3 mM in cerebellum. However, no definitive statements can be made about putative changes in early infancy because large changes in tCr have been observed in neonates (5, 7). Although the present PCr concentrations are slightly lower than in vivo phosphorus MRS determinations of 2.5 mM in mixed gray and white matter of midbrain (30) or 2.9 mM in white matter, 3.1 mM in gray matter, and 3.9 mM in cerebellum of young adults (31), the latter study qualitatively confirms the observed regional differences.
Intersubject averaging of all spectra obtained for a specific tissue yields Cr-to-tCr concentration ratios of 0.65 ± 0.08 in gray matter, 0.66 ± 0.11 in white matter, 0.61 ± 0.08 in cerebellum, 0.64 ± 0.25 in thalamus, and 0.63 ± 0.13 in basal ganglia. Thus, despite regional differences in absolute Cr and PCr concentrations, these results indicate an almost constant Cr-to-PCr ratio of 2:1 throughout the human brain, i.e. irrespective of tissue type, cellular composition, or developmental stage (after 1 y of age). In contrast, the combination of in vivo and in vitro phosphorus MRS data of piglets and rats suggested a much lower Cr-to-PCr ratio in white matter than in gray matter (32).
Cho.
In all brain regions investigated, the concentration of Cho tends to be highest in the youngest infants. During childhood and adolescence, Cho remains constant at the adult level and therefore exhibits the same regional distribution as described for adulthood (15). In particular, for white matter, the Cho concentrations in older children (5–18 y) are about 15% below the levels in infants and young children (0–5 y). This difference has been attributed to the fact that myelination during early childhood (1, 5) causes a pronounced turnover of membrane precursor molecules. Although there is also a continuous turnover of myelin in adults, the initial process of myelination requires a considerably larger amount of phosphocholine, which is both a key substrate for the glycerophospholipids in myelin and a major contributor to the proton MRS-detected Cho resonance. Similar observations have been made using phosphorus MRS in which high phosphocholine levels may be identified by their contribution to the phosphomonoester region of the phosphorus spectrum (29).
Ins.
The concentration of Ins remains constant in most brain regions except for the cerebellum. In all age groups, the cerebellum shows the highest Ins levels of the brain regions investigated. The reason for this observation remains unclear but may be caused by its glial composition, e.g. a high proportion of astrocytes, or may reflect the function of Ins as an osmoregulator (15). Despite the large SD in the youngest age groups, which are caused by only a small number of subjects, the Ins level in the cerebellum decreases from its highest value during early development by about 30% toward adolescence and adulthood. The only other study of age-dependent metabolite levels in the cerebellum mentioned no Ins differences between infants and adults using a VOI located in the cerebellar hemisphere (3).
Glu and Gln.
Within experimental accuracy, none of the investigated brain regions shows a developmental increase or decrease of Glu. Glu is an important excitatory neurotransmitter in the CNS, but it is also involved in the synthesis of proteins and fatty acids as well as in the metabolism of Gln and GABA (33). Because the transmitter pool of Glu constitutes only approximately 30% of the total Glu concentration, possible developmental changes of Glu as a neurotransmitter are unlikely to be observable by proton MRS.
As far as Gln quantitation is concerned, its concentration also remains constant except for a 50% reduction in white matter from early childhood to adulthood. Because Gln is synthesized from Glu in astrocytes, a reaction catalyzed by glutamine synthetase, one may speculate that the reason for this observation is related to a maturational change in function or density of white matter glial cells.
Other metabolites.
A clear developmental decrease of Tau is observed in the cerebellum and gray matter, which have the highest concentrations in infancy. These findings are in agreement with in vitro determinations in occipital gray matter yielding 3.3 mmol/kg wet weight in children aged 1–5 y and only 1.4 mmol/kg wet weight in adults (34). Noteworthy, the reduction of Tau accompanies the elevation of NAA with age, although with a larger time constant of about 10 y. In fact, a linear correlation between Tau and NAA is found both in gray matter (ρ = −0.41, p< 0.001) and in cerebellum (ρ = −0.37, p< 0.05). In white matter and thalamus, the concentration of Tau is lower, but also shows a trend for a decrease with age. Remarkably, in basal ganglia, both NAA and Tau remain constant. Although these observations do not prove a direct correlation, a link between changes in NAA and Tau is not unlikely. Tau has been suggested to play a role in neuronal differentiation, arborization, and the formation of synaptic connections (34). All these processes probably lead to an increase of NAA. From another point of view, assuming that Tau and NAA are metabolically inert amino acids, it has been proposed that the exchange of Tau by NAA facilitates the cytosolic transport of the high-energy phosphates PCr and ATP, supporting the increased energy demand during maturation (35).
The concentration of GABA is highest in basal ganglia, cerebellum, and gray matter. In these regions, its level remains constant during development. GABA is the major inhibitory neurotransmitter in the CNS (36). Its concentration in the millimolar range is maintained by uptake of GABA into nerve terminals and synthesis from Glu in neurons.
The observation of only small concentrations of Lac in all brain regions is in line with the common understanding that the metabolism of well-oxygenated brain tissue is unlikely to accumulate large amounts of Lac under physiologic conditions (37). The use of mean spectra facilitates the in vivo determination of steady-state concentrations of 0.4–0.5 mM.
Resonance line-widths.
An increase of the proton MRS line-widths with age is observed in all brain regions, except for the cerebellum, in which resonances are already broad in infants. The effect is relatively small in gray and white matter and most pronounced in the basal ganglia, leading to adult spectra with poor spectral resolution.
The line-width is determined by the magnetic field homogeneity within the VOI. It depends both on the regional field homogeneity of the magnet and on tissue-specific factors such as iron content, which has been shown to vary regionally and developmentally (38). An increase of paramagnetic iron, e.g. in the form of ferritin, causes a corresponding decrease of the effective spin-spin relaxation time T2* (and also of T2) of surrounding water and metabolite protons, which is inversely proportional to the respective spectral line-widths. The observed line-width increase is indeed in good agreement with the reported regional increase of nonheme iron (38). In infants the iron content is low throughout the brain. A linear increase during the first 20–30 y of age results in highest concentrations in the basal ganglia, i.e. especially in globus pallidus and somewhat less in putamen and caudate nucleus, followed by thalamus and parietal cortex. A qualitative confirmation of the present findings stems from magnetic resonance imaging studies of the developing human brain, in which differences in signal intensity and contrast are based on a regionally dependent increase of iron (39).
In the cerebellum, a possible increase of iron has little effect because the spectral line-width is already large in infants. The reason for this observation is not entirely clear but may be caused by cellular as well as structural inhomogeneities caused by extensive gyration, i.e. susceptibility transitions between brain and CSF, and VOI contributions from several anatomic structures including the vermis, the dentate nuclei, and part of the gray and white matter of the cerebellar hemispheres.
Abbreviations
- Cr:
-
creatine
- Cho:
-
choline-containing compounds
- FWHM:
-
full line-width at half maximum
- GABA:
-
γ-aminobutyric acid
- Glc:
-
glucose
- Glu:
-
glutamate
- Gln:
-
glutamine
- Ins:
-
myo-inositol
- Lac:
-
lactate
- MRS:
-
magnetic resonance spectroscopy
- NAA:
-
N-acetylaspartate
- NAAG:
-
N-acetylaspartylglutamate
- PCr:
-
phosphocreatine
- ppm:
-
parts per million
- scyllo-Ins:
-
scyllo-inositol
- SNR:
-
signal-to-noise ratio
- STEAM:
-
stimulated echo acquisition mode
- Tau:
-
taurine
- tCr:
-
total creatine
- T1:
-
spin-lattice relaxation time
- T2:
-
spin-spin relaxation time
- TE:
-
echo time
- TM:
-
mixing time
- tNAA:
-
total N-acetylaspartyl compounds
- TR:
-
repetition time
- VOI:
-
volume-of-interest
References
van der Knaap MS, van der Grond J, van Rijen PC, Faber JAJ, Valk J, Willemse K 1990 Age-dependent changes in localized proton and phosphorus MR spectroscopy of the brain. Radiology 176: 509–515.
Peden CJ, Cowan FM, Bryant DJ, Sargentoni J, Cox IJ, Menon DK, Gadian DG, Bell JD, Dubowitz LM 1990 Proton MR spectroscopy of the brain in infants. J Comput Assist Tomogr 14: 886–894.
Hüppi PS, Posse S, Lazeyras F, Burri R, Bossi E, Herschkowitz N 1991 Magnetic resonance in preterm and term newborns: 1H spectroscopy in developing human brain. Pediatr Res 30: 574–578.
Bruhn H, Kruse B, Korenke GC, Hanefeld F, Hänicke W, Merboldt KD, Frahm J 1992 Proton NMR spectroscopy of cerebral metabolic alterations in infantile peroxisomal disorders. J Comput Assist Tomogr 16: 335–344.
Kreis R, Ernst T, Ross BD 1993 Development of the human brain: in vivo quantification of metabolite and water content with proton magnetic resonance spectroscopy. Magn Reson Med 30: 424–437.
Toft PB, Leth H, Lou HC, Pryds O, Henriksen O 1994 Metabolite concentrations in the developing brain estimated with proton MR spectroscopy. J Magn Reson Imaging 4: 674–680.
Hüppi PS, Fusch C, Boesch C, Burri R, Bossi E, Amato M, Herschkowitz N 1995 Regional metabolic assessment of human brain during development by proton magnetic resonance spectroscopy in vivo and by high-performance liquid chromatography/gas chromatography in autopsy tissue. Pediatr Res 37: 145–150.
Hashimoto T, Tayama M, Miyazaki M, Fujii E, Harada M, Miyoshi H, Tanouchi M, Kuroda Y 1995 Developmental brain changes investigated with proton magnetic resonance spectroscopy. Dev Med Child Neurol 37: 398–405.
Kimura H, Fujii Y, Itoh S, Matsuda T, Iwasaki T, Maeda M, Konishi Y, Ishii Y 1995 Metabolic alterations in the neonate and infant brain during development: : evaluation with proton MR spectroscopy. Radiology 194: 483–489.
Frahm J, Hanefeld F 1996 Localized proton magnetic resonance spectroscopy of cerebral metabolites. Neuropediatrics 27: 1–6.
Hüppi PS, Schuknecht B, Boesch C, Bossi E, Felblinger J, Fusch C, Herschkowitz N 1996 Structural and neurobehavioral delay in postnatal brain development of preterm infants. Pediatr Res 39: 895–901.
Cady EB, Penrice J, Amess PN, Lorek A, Wylezinska M, Aldridge RF, Franconi F, Wyatt JS, Reynolds EOR 1996 Lactate, N-acetylaspartate, choline and creatine concentrations, and spin-spin relaxation in thalamic and occipito-parietal regions of developing human brain. Magn Reson Med 36: 878–886.
Lu D, Pavlakis SG, Frank Y, Bakshi S, Pahwa S, Gould RJ, Sison C, Hsu C, Lesser M, Hoberman M, Barnett T, Hyman RA 1996 Proton MR spectroscopy of the basal ganglia in healthy children and children with AIDS. Radiology 199: 423–428.
Holshouser BA, Ashwal S, Luh GY, Shu S, Kahlon S, Auld KL, Tomasi LG, Perkin RM, Hinshaw DB 1997 Proton MR spectroscopy after acute central nervous system injury: : outcome prediction in neonates, infants, and children. Radiology 202: 487–496.
Pouwels PJW, Frahm J 1998 Regional metabolite concentrations in human brain as determined by quantitative localized proton MRS. Magn Reson Med 39: 53–60.
Frahm J, Hanefeld F 1997 Localized proton magnetic resonance spectroscopy of brain disorders in childhood. In: Bachelard HS (ed) Advances in Neurochemistry, Vol. 8. Plenum, New York, 329–402.
Frahm J, Michaelis T, Merboldt KD, Bruhn H, Gyngell ML, Hänicke W 1990 Improvements in localized 1H NMR spectroscopy of human brain. J Magn Reson 90: 464–473.
Klose U 1990 In vivo proton spectroscopy in presence of eddy currents. Magn Reson Med 14: 26–30.
Provencher SW 1993 Estimation of metabolite concentrations from localized in vivo proton NMR spectra. Magn Reson Med 30: 672–679.
Michaelis T, Merboldt KD, Bruhn H, Hänicke W, Frahm J 1993 Absolute concentrations of metabolites in the adult human brain in vivo: : quantification of localized proton MR spectra. Radiology 187: 219–227.
Pouwels PJW, Frahm J 1997 Differential distribution of NAA and NAAG in human brain as determined by quantitative localized proton MRS. NMR Biomed 10: 73–78.
Pouwels PJW, Kruse B, Hanefeld F, Frahm J 1997 Age dependence of human cerebral metabolites in gray matter, white matter, and basal ganglia as determined by quantitative localized proton MRS. Proceedings of the 5th annual meeting of the International Society for Magnetic Resonance in Medicine (ISMRM), Vancouver, 482
Birken DL, Oldendorf WH 1989 N-Acetyl- L -aspartic acid: : a literature review of a compound prominent in 1H NMR spectroscopic studies of brain. Neurosci Biobehav Rev 13: 23–31.
Moffett JR, Namboodiri MAA, Neale JH 1993 Enhanced carbodiimide fixation for immunohistochemistry: application to the comparative distributions of N-acetylaspartylglutamate and N-acetylaspartate immunoreactivities in rat brain. J Histochem Cytochem 41: 559–570.
Moffett JR, Namboodiri MAA 1995 Differential distribution of N-acetylaspartylglutamate and N-acetylaspartate immunoreactivities in rat forebrain. J Neurocytol 24: 409–433.
Kelly JP, Dodd J 1991 Anatomical organization of the nervous system. In: Kandel ER, Schwartz JH, Jessell TM (eds) Principles of Neural Science, 3rd Ed. Elsevier, New York, 273–282.
Miyake M, Kakimoto Y 1981 Developmental changes of N-acetyl- L -aspartic acid, N-acetyl-α-aspartylglutamic acid and β-citryl- L -glutamic acid in different brain regions and spinal cords of rat and guinea pig. J Neurochem 37: 1064–1067.
Blakely RD, Coyle JT 1988 Neurobiology of N-acetylaspartylglutamate. In: Smythies JR, Bradley RJ (eds) International review of neurobiology, Vol. 30. Academic Press, San Diego, 39–100.
Buchli R, Martin E, Boesiger P, Rumpel H 1994 Developmental changes of phosphorus metabolite concentrations in the human brain: : a 31P magnetic resonance spectroscopy study in vivo. Pediatr Res 35: 431–435.
Requardt M 1995 In vivo31P-NMR-Spektroskopie der Kreatinkinasereaktion am Skelettmuskel und Gehirn des Menschen. Dissertation, Universität Göttingen, Germany, 69–73.
Buchli R, Duc CO, Martin E, Boesiger P 1994 Assessment of absolute metabolite concentrations in human tissue by 31P MRS in vivo. Magn Reson Med 32: 447–452.
Holtzman D, Mulkern R, Tsuji M, Cook C, Meyers R 1996 Phosphocreatine and creatine kinase in piglet cerebral gray and white matter in situ. Dev Neurosci 18: 535–541.
Dingledine R, McBain CJ 1994 Excitatory amino acid transmitters. In: Siegel GJ, Agranoff BW, Albers RW, Molinoff PB (eds) Basic Neurochemistry, 5th Ed. Raven Press, New York, 367–387.
Sturman JA 1993 Taurine in development. Physiol Rev 73: 119–147.
Nakada T, Kwee IL, Igarashi H 1994 Brain maturation and high-energy phosphate diffusivity: alteration in cytosolic microenvironment and effective viscosity. Dev Brain Res 80: 121–126.
DeLorey TM, Olsen RW 1994 GABA and glycine. In: Siegel GJ, Agranoff BW, Albers RW, Molinoff PB (eds) Basic Neurochemistry, 5th Ed. Raven Press, New York, 389–399.
Clarke DD, Sokoloff L 1994 Circulation and energy metabolism of the brain. In: Siegel GJ, Agranoff BW, Albers RW, Molinoff PB (eds) Basic Neurochemistry, 5th Ed. Raven Press, New York, 645–680.
Hallgren B, Sourander P 1958 The effect of age on the non-haemin iron in the human brain. J Neurochem 3: 41–51.
Aoki S, Okada Y, Nishimura K, Barkovich AJ, Kjos BO, Brasch RC, Norman D 1989 Normal deposition of brain iron in childhood and adolescence: : MR imaging at 1. Radiology 172: 381–385.
Acknowledgements
The authors thank Dr. Stephen Provencher for continuing support in the use of LCModel and Xiangling Mao for developing data processing software.
Author information
Authors and Affiliations
Additional information
P.J.W. Pouwels was supported by a fellowship of the European Community (ERBCHBGCT 940722).
Rights and permissions
About this article
Cite this article
Pouwels, P., Brockmann, K., Kruse, B. et al. Regional Age Dependence of Human Brain Metabolites from Infancy to Adulthood as Detected by Quantitative Localized Proton MRS. Pediatr Res 46, 474 (1999). https://doi.org/10.1203/00006450-199910000-00019
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199910000-00019
This article is cited by
-
Microstructural and Metabolic Changes in Normal Aging Human Brain Studied with Combined Whole-Brain MR Spectroscopic Imaging and Quantitative MR Imaging
Clinical Neuroradiology (2023)
-
Magnetic resonance spectroscopy brain metabolites at term and 3-year neurodevelopmental outcomes in very preterm infants
Pediatric Research (2022)
-
Brain proton magnetic resonance spectroscopy and neurodevelopment after preterm birth: a systematic review
Pediatric Research (2022)
-
Altered brain metabolite concentration and delayed neurodevelopment in preterm neonates
Pediatric Research (2022)
-
Edited magnetic resonance spectroscopy in the neonatal brain
Neuroradiology (2022)
